Portal hypertension anatomy, causes, clinical feature
Reading File
Finding Sources
Searching PubMed
"portal hypertension" pathophysiology management
Reading File
Reading File
Reading File
Searching Images
portal hypertension anatomy collaterals
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Excellent — I now have all the material needed for a comprehensive answer. Let me synthesize everything.
Portal Hypertension
Definition: Portal hypertension is defined as an increase in hepatic sinusoidal pressure, measured by a hepatic venous pressure gradient (HVPG) ≥ 6 mmHg. The threshold for clinically significant portal hypertension (CSPH) is HVPG ≥ 10 mmHg, and the threshold for variceal bleeding risk is HVPG > 12 mmHg.
1. Anatomy of the Portal Venous System
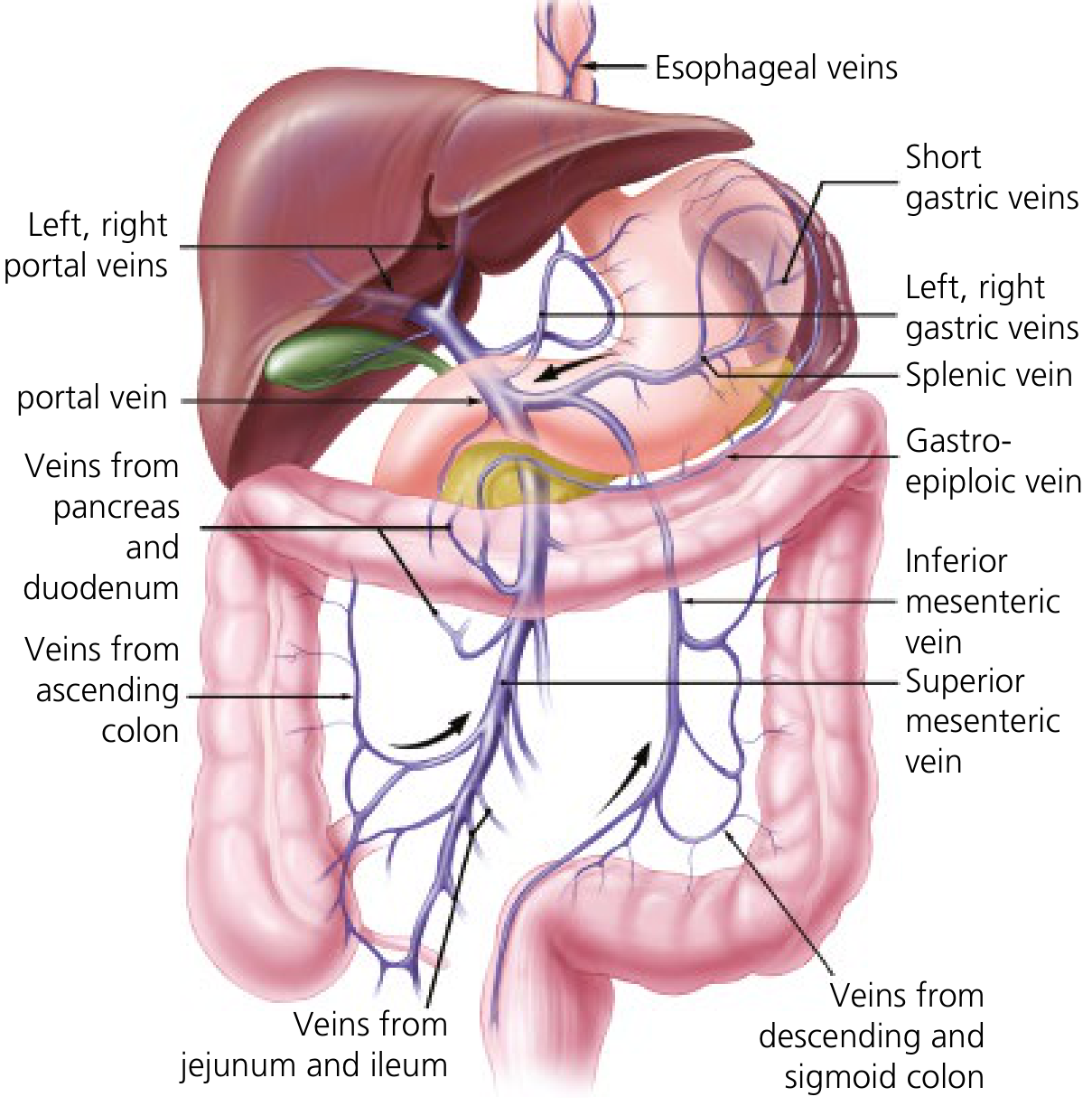
The portal vein is formed by the confluence of the superior mesenteric vein (SMV) and the splenic vein behind the neck of the pancreas. Key tributaries:
| Tributary | Drains into |
|---|---|
| Inferior mesenteric vein (IMV) | Splenic vein (usually) |
| Left gastric (coronary) vein | Portal vein at SMV-splenic confluence |
| Right gastric vein | Portal vein |
| Umbilical vein | Left portal vein |
The portal vein is ~7.5 cm long, has no tributaries in its upper 5 cm, and divides into left and right branches at the hepatic hilum. It carries 75% of hepatic blood flow and supplies ~50% of hepatic oxygen. Blood drains from hepatic sinusoids → hepatic veins → inferior vena cava (IVC).
The sinusoids are highly permeable, lined by fenestrated endothelium, lacking a proper basement membrane. The space of Disse contains hepatic stellate cells (HSCs) and Kupffer cells — key regulators of hepatic hemodynamics.
2. Pathophysiology
Portal pressure = Portal blood flow × Vascular resistance (Ohm's law analogy). Portal hypertension therefore results from:
A. Increased Intrahepatic Resistance (primary mechanism in cirrhosis)
Two components:
Fixed (mechanical):
- Regenerative nodules and fibrotic bands compress and distort sinusoids
- Capillarization of sinusoids (loss of fenestrations)
- Swelling of hepatocytes and Kupffer cells
Dynamic (reversible — therapeutic target):
- Activated HSCs act as perisinusoidal pericytes and contract in response to vasoconstrictor stimuli
- ↓ nitric oxide (NO) production by endothelial cells → impaired vasodilation
- ↑ endothelin-1 (ET-1), angiotensin II → intrahepatic vasoconstriction
- Imbalance: vasoconstrictors dominate over vasodilators within the liver
B. Hyperdynamic Splanchnic Circulation (perpetuating factor)
In portal hypertension, splanchnic arterioles undergo vasodilation driven by:
- ↑ NO in splanchnic circulation (opposite to the liver: NO is increased here)
- Inflammatory mediators (bacterial translocation → PAMPs → cytokines)
- Increased production of prostacyclin and glucagon
This results in:
- Increased splanchnic blood flow → increased portal inflow
- Reduced effective arterial blood volume → activation of RAAS and sympathetic nervous system → sodium retention → ascites
- Cardiac output is initially increased (hyperdynamic state); reduced at late stages
C. Collateral Circulation Development
Because portal pressure exceeds systemic venous pressure, blood is diverted through pre-existing portosystemic anastomoses (hepatofugal flow). These collaterals are inadequate to fully decompress the portal system and give rise to varices.
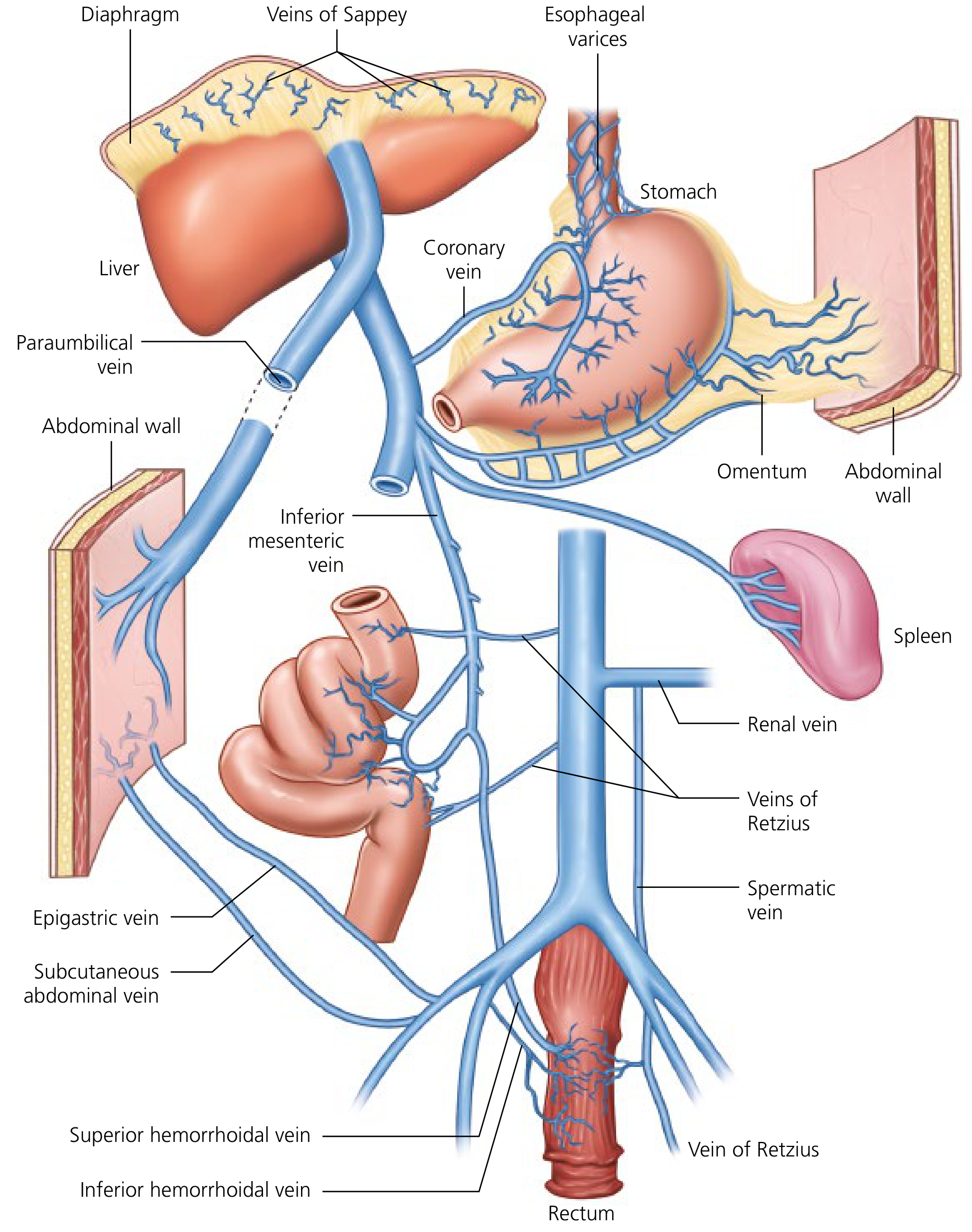
3. Portosystemic Collaterals
| Collateral Site | Portal Tributary | Systemic Vein | Clinical Consequence |
|---|---|---|---|
| Gastroesophageal | Left gastric (coronary) vein, short gastric veins | Esophageal veins (azygos system) | Esophageal & gastric varices — risk of life-threatening hemorrhage |
| Periumbilical | Paraumbilical vein (from left portal vein) → ligamentum teres | Epigastric/abdominal wall veins | Caput medusae |
| Anorectal | Superior rectal vein (IMV) | Inferior & middle rectal veins (IVC) | Hemorrhoids (anorectal varices) |
| Retroperitoneal | Mesenteric branches | Renal veins, spermatic veins, veins of Retzius | Splenorenal shunts — associated with hepatic encephalopathy |
| Diaphragmatic | Veins of Sappey | Diaphragmatic veins | Rarely clinically significant |
A paraumbilical collateral vein is the most specific sign of intrahepatic (parenchymal) portal hypertension, as it indicates obstruction at the liver level rather than extrahepatic obstruction. — Yamada's Gastroenterology
4. Classification by Site of Obstruction
| Level | Site | Examples |
|---|---|---|
| Prehepatic | Portal/splenic vein | Portal vein thrombosis, splenic vein thrombosis, arterioportal fistula |
| Intrahepatic — Presinusoidal | Portal tracts | Schistosomiasis (pipestem fibrosis), primary biliary cholangitis (early), sarcoidosis, congenital hepatic fibrosis, nodular regenerative hyperplasia |
| Intrahepatic — Sinusoidal | Sinusoids | Cirrhosis (most common) — alcoholic, viral, NAFLD, autoimmune, hemochromatosis |
| Intrahepatic — Postsinusoidal | Central veins/terminal hepatic venules | Sinusoidal obstruction syndrome (veno-occlusive disease), alcohol (perivenular injury) |
| Posthepatic | Hepatic veins / IVC / Right heart | Budd-Chiari syndrome, constrictive pericarditis, right heart failure, IVC web |
Note: HVPG measurement is only accurate for sinusoidal and postsinusoidal causes. In prehepatic/presinusoidal portal hypertension, HVPG is normal or only mildly elevated.
5. Causes of Portal Hypertension
Common
- Cirrhosis — accounts for the vast majority in the West (alcoholic liver disease, chronic viral hepatitis B/C, NAFLD/NASH, autoimmune hepatitis, hemochromatosis, Wilson's disease, PBC, PSC)
- Schistosomiasis — most common cause worldwide (presinusoidal); caused by S. mansoni or S. japonicum depositing eggs in presinusoidal portal venules → granulomatous inflammation → "pipestem fibrosis"
Less Common
- Portal vein thrombosis — associated with myeloproliferative neoplasms, hypercoagulable states, intra-abdominal infection, pancreatitis, malignancy
- Splenic vein thrombosis — causes "sinistral" (left-sided) portal hypertension; commonly due to pancreatitis
- Budd-Chiari syndrome — hepatic vein outflow obstruction; causes posthepatic portal hypertension
- Nodular regenerative hyperplasia — sinusoidal obliteration without fibrosis (associated with azathioprine, oxaliplatin, HIV)
- Sinusoidal obstruction syndrome — endothelial damage; associated with bone marrow transplantation, chemotherapy
- Congenital hepatic fibrosis — autosomal recessive; portal hypertension without liver failure
- Right heart failure / constrictive pericarditis — raised hepatic venous pressure transmitted back to sinusoids
- Arterioportal fistula — increased portal inflow
6. Clinical Features
A. Splenomegaly & Hypersplenism
- Elevated portal pressure in the splenic vein → splenomegaly
- Sequestration of blood cells → thrombocytopenia (most common and earliest), leucopenia, anaemia (pancytopenia = hypersplenism)
B. Ascites
- Triggered by splanchnic arterial vasodilation → effective arterial hypovolemia → RAAS & SNS activation → renal sodium retention
- Increased hydrostatic pressure in splanchnic capillaries (Starling forces) promotes transudation
- Hypoalbuminaemia reduces oncotic pressure
C. Variceal Hemorrhage
- Esophageal varices: most important; present in ~50% of cirrhotics; bleeding risk highest when HVPG > 12 mmHg; ~30% mortality per bleeding episode
- Endoscopic appearance: small (≤5 mm) vs. large (>5 mm); red wale marks, cherry red spots, hematocystic spots all indicate high bleeding risk
- Gastric varices (GOV1, GOV2, IGV1, IGV2 — Sarin classification): gastric fundal varices (IGV1) have highest bleeding risk
- Rectal varices (distinguished from hemorrhoids)
D. Caput Medusae
- Dilated paraumbilical veins radiating from the umbilicus
- Pathognomonic of intrahepatic portal hypertension
E. Hepatic Encephalopathy
- Portal blood (containing ammonia and other toxins) bypasses the liver through portosystemic shunts → toxins accumulate in systemic circulation → cross blood-brain barrier → astrocyte dysfunction, cerebral oedema
- Precipitated by infection, GI bleed, renal failure, constipation, excess dietary protein, benzodiazepines
F. Portal Hypertensive Gastropathy (PHG)
- Mosaic pattern of gastric mucosa on endoscopy; submucosal congestion without inflammation
- Can cause chronic occult bleeding
G. Hepatorenal Syndrome (HRS)
- Extreme renal vasoconstriction as a consequence of RAAS/SNS activation and reduced cardiac output
- Functional renal failure without structural kidney damage
H. Cardiopulmonary Complications
- Hepatopulmonary syndrome: intrapulmonary vascular dilatations → shunting → hypoxia; orthodeoxia (desaturation on sitting up)
- Portopulmonary hypertension: pulmonary arterial hypertension due to increased splanchnic mediators reaching the pulmonary circulation
- Cirrhotic cardiomyopathy: systolic dysfunction under stress, diastolic dysfunction, prolonged QT
I. Hepatic Hydrothorax
- Transdiaphragmatic passage of ascitic fluid (usually right-sided pleural effusion)
J. Haematological Features
- Coagulopathy (impaired synthesis of clotting factors)
- Anaemia (multifactorial: hypersplenism, variceal blood loss, poor nutrition)
7. Measurement of Portal Pressure
- HVPG (gold standard): WHVP − FHVP; measured via transjugular or femoral hepatic vein catheterization with balloon-occluding catheter
- Normal: < 6 mmHg
- Portal hypertension: ≥ 6 mmHg
- CSPH: ≥ 10 mmHg (predicts variceal formation)
- Variceal bleeding threshold: > 12 mmHg
- Non-invasive surrogates: liver stiffness (LSM) >20–25 kPa by elastography + low platelets + splenomegaly = CSPH
- HVPG is not accurate for prehepatic or presinusoidal causes
Sources:
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease, Chapter 92 (Shah & Kamath)
- Yamada's Textbook of Gastroenterology, 7th ed., Chapter 124 (Kamath & Wong Kee Song)
- Medical Physiology (Boron & Boulpaep)
- Mulholland & Greenfield's Surgery, 7th ed.
This is a shared conversation. Sign in to Orris to start your own chat.