ulcer formation in ibd difference
Ulcer Formation in IBD: Crohn Disease vs. Ulcerative Colitis
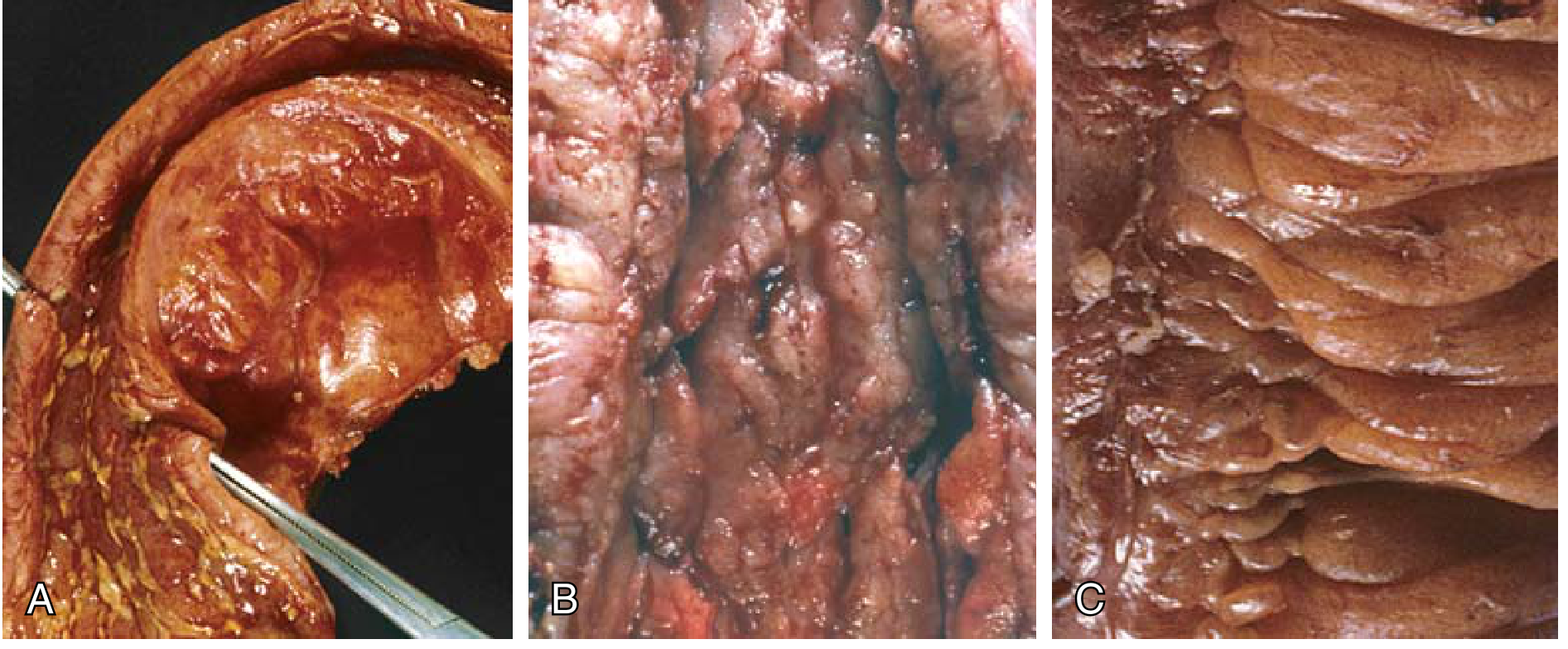
1. Crohn Disease (CD)
- The earliest lesion is the aphthous ulcer - a tiny, discrete superficial erosion overlying a lymphoid aggregate
- Multiple aphthous ulcers coalesce and enlarge into elongated, serpentine ulcers oriented along the long axis of the bowel
- Fissures develop between mucosal folds and can extend deeply through all layers
- Cobblestone mucosa - ulcerated tissue sinks below the level of surviving normal mucosa, creating irregular raised "islands" of normal mucosa between deep ulcers
- Deep knife-like fissures that penetrate into the submucosa, muscularis, and even serosa
- Skip lesions - sharply demarcated areas of disease interspersed with normal bowel (pathognomonic of CD)
- Neutrophil infiltration of crypts → crypt abscesses → crypt destruction
- Abrupt transition between ulcerated and normal mucosa
- Noncaseating granulomas in ~35% of cases (any layer of the wall, or even in mesenteric lymph nodes and skin)
- Transmural inflammation with submucosal fibrosis and muscularis hypertrophy
- Fistula formation (bowel-to-bowel, enterovesical, enterovaginal, perianal)
- Abscesses and perforation
- Strictures (from transmural fibrosis - common)
- Creeping fat (mesenteric fat wraps around the serosal surface due to transmural disease)
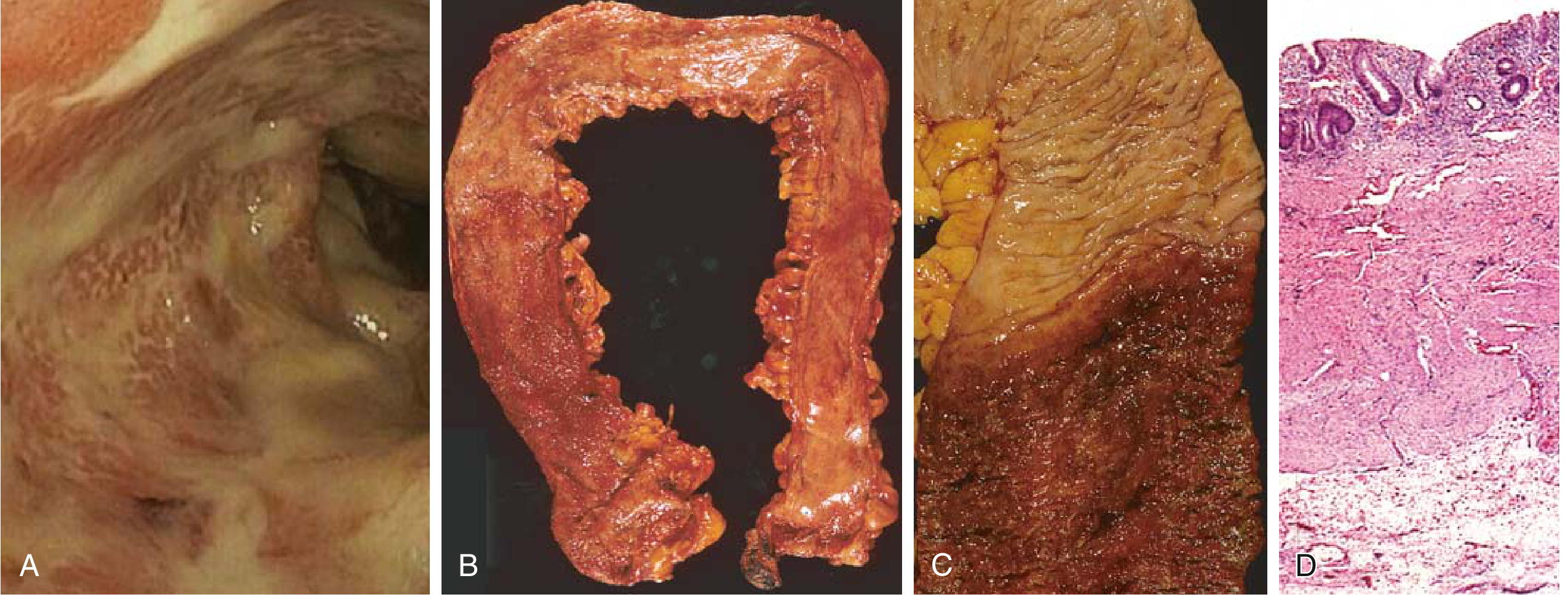
2. Ulcerative Colitis (UC)
- Broad-based, shallow ulcers that do not replicate the deep serpentine pattern of CD
- Ulcers are aligned along the long axis of the colon but remain superficial
- In severe cases, ulcers extend slightly deeper into the submucosa, but the muscularis propria is rarely involved
- Continuous, confluent inflammation starting at the rectum and extending proximally (no skip lesions)
- Mucosa appears red, granular, or with broad ulceration
- Pseudopolyps - isolated islands of regenerating mucosa bulge into the lumen, forming polyp-like projections; their tips may fuse to create mucosal bridges
- No mural thickening, no cobblestoning, no creeping fat
- Abrupt (sharp) transition between inflamed and normal mucosa
- Inflammatory infiltrates, crypt abscesses, crypt distortion (similar to CD)
- Inflammation limited to mucosa and superficial submucosa
- No granulomas
- No transmural involvement
- Toxic megacolon (mucosal damage + neuromuscular dysfunction → colonic dilation; risk of perforation)
- No fistulas (because inflammation does not penetrate deeply enough)
- Strictures are rare (no transmural fibrosis)
Summary Comparison Table
| Feature | Crohn Disease | Ulcerative Colitis |
|---|---|---|
| Earliest ulcer | Aphthous ulcer | Superficial mucosal erosion |
| Ulcer type | Deep, fissuring, serpentine | Shallow, broad-based |
| Ulcer shape | Elongated, linear/serpentine | Longitudinal but shallow |
| Depth | Transmural (all layers) | Mucosa ± superficial submucosa |
| Cobblestoning | Yes (normal mucosa between deep ulcers) | No |
| Skip lesions | Yes (pathognomonic) | No (continuous from rectum) |
| Pseudopolyps | Can occur | Common (regenerating mucosa islands) |
| Granulomas | ~35% (noncaseating) | Absent |
| Fissures/Fistulas | Yes (due to depth) | No |
| Strictures | Common (transmural fibrosis) | Rare |
| Perforation | Can occur via fissures | Only in toxic megacolon |
| Mural thickening | Yes (rubbery, thickened wall) | No (wall normal thickness) |
| Creeping fat | Yes (serosal) | No |
Why the Difference?
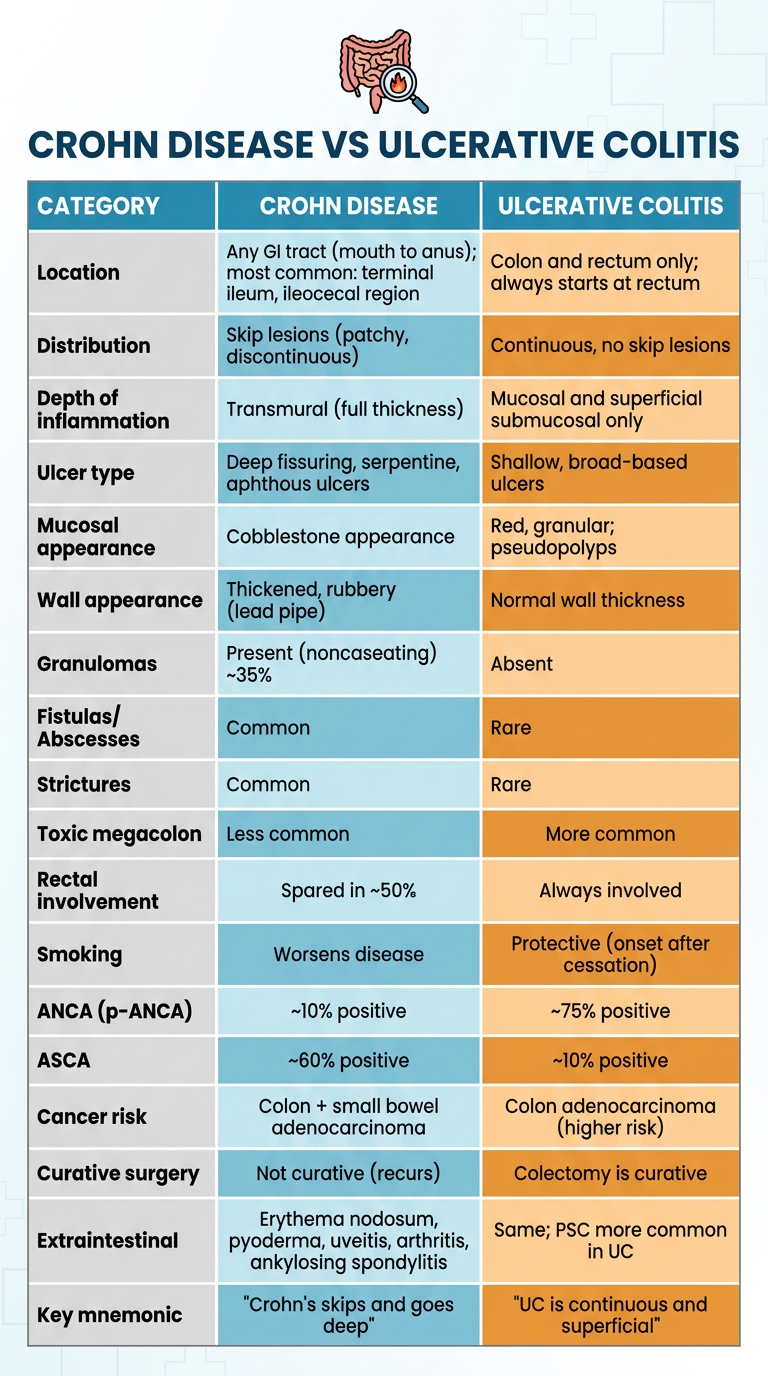
Create a comparison table of CD vs UC for quick clinical reference
A clean, professional clinical quick-reference comparison table poster titled "Crohn Disease vs Ulcerative Colitis" with a medical/academic style. Two-column table comparing the two conditions across the following categories, each as a clearly labeled row: CATEGORY | CROHN DISEASE | ULCERATIVE COLITIS Location | Any GI tract (mouth to anus); most common: terminal ileum, ileocecal region | Colon and rectum only; always starts at rectum Distribution | Skip lesions (patchy, discontinuous) | Continuous, no skip lesions Depth of inflammation | Transmural (full thickness) | Mucosal and superficial submucosal only Ulcer type | Deep fissuring, serpentine, aphthous ulcers | Shallow, broad-based ulcers Mucosal appearance | Cobblestone appearance | Red, granular; pseudopolyps Wall appearance | Thickened, rubbery (lead pipe) | Normal wall thickness Granulomas | Present (noncaseating) ~35% | Absent Fistulas/Abscesses | Common | Rare Strictures | Common | Rare Toxic megacolon | Less common | More common Rectal involvement | Spared in ~50% | Always involved Smoking | Worsens disease | Protective (onset after cessation) ANCA (p-ANCA) | ~10% positive | ~75% positive ASCA | ~60% positive | ~10% positive Cancer risk | Colon + small bowel adenocarcinoma | Colon adenocarcinoma (higher risk) Curative surgery | Not curative (recurs) | Colectomy is curative Extraintestinal | Erythema nodosum, pyoderma, uveitis, arthritis, ankylosing spondylitis | Same; PSC more common in UC Key mnemonic | "Crohn's skips and goes deep" | "UC is continuous and superficial" Use color coding: blue/teal header and alternating light blue rows for Crohn Disease column, orange/warm amber alternating rows for Ulcerative Colitis column. Bold the category names in left column. Make it large, readable, and suitable for clinical exam revision. Include a small bowel anatomy icon or IBD-related medical icon at the top.
- Location & distribution (skip lesions vs. continuous)
- Depth (transmural vs. mucosal)
- Ulcers & wall changes (cobblestone/fissuring vs. pseudopolyps/shallow)
- Serology (ASCA vs. p-ANCA)
- Complications (fistulas/strictures vs. toxic megacolon/PSC)
- Surgery (non-curative vs. curative colectomy)
- Smoking (opposite effects in both)
why bloody diaheera in uc but not in crohns
Why Bloody Diarrhea in UC but NOT (usually) in Crohn's?
Reason 1: UC Ulcers Directly Erode the Submucosal Vascular Plexus
- Blood vessels are directly exposed to the lumen
- Erosion of these vessels causes frank bleeding into the stool
- Because the disease is continuous and extensive (rectum to proximal colon), many bleeding points exist simultaneously
Reason 2: UC Always Involves the Rectum - Blood Can't Be Reabsorbed
- Blood enters the lumen at the most distal point of the colon
- It has no time or distance to be modified - it exits as fresh red blood
- Rectal inflammation also causes urgency, tenesmus, and frequent small-volume stools - the patient is constantly "pushing out" whatever blood and mucus is there
Reason 3: Crohn's Ulcers Go DEEP - Blood Gets Trapped, Not Expelled
- Blood from deep fissures can track into the bowel wall rather than into the lumen
- It may form abscesses or fistulas rather than intraluminal bleeding
- The skip lesion pattern means large areas of normal mucosa exist between ulcers, reducing the surface area actively bleeding into the lumen
Reason 4: Crohn's Often Affects the Small Bowel - Where Bleeding Behaves Differently
- Is much less common and less dramatic than colonic bleeding
- Blood from the terminal ileum travels a long distance through the colon and appears as dark/tarry stool (melena) rather than fresh red blood - often not noticed by patients
- The small bowel's primary function is absorption/secretion, not storage - so diarrhea in small bowel CD is large-volume, watery, and malabsorptive (from bile salt malabsorption, fat malabsorption), not bloody
Reason 5: Colonic Motility Amplifies Bleeding in UC
- Mechanically traumatizes the fragile inflamed mucosa repeatedly
- Prevents hemostasis - clots can't form on moving, repeatedly irritated surfaces
- Drives frequent passage of bloody stool
The Important Caveat: Crohn's CAN Cause Bloody Diarrhea
Summary Mechanism
| Factor | UC | Crohn's (SB-predominant) |
|---|---|---|
| Location of ulcers | Colonic mucosa/submucosa | Often terminal ileum, transmural |
| Vessel exposure | Direct - submucosal capillaries eroded | Deep - blood tracks into wall |
| Rectal involvement | Always - blood exits immediately | Usually spared |
| Mucosal continuity | Entire surface inflamed | Skip areas of normal mucosa |
| Diarrhea type | Small-volume, frequent, bloody + mucus | Large-volume, watery, malabsorptive |
| Motility changes | Hyperactive, constant mass movements | Variable |