Teqch me spleen disorders of surgery subject
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive textbook content and images. Let me compile the full teaching guide on spleen disorders in surgery.
Spleen Disorders - Surgery
Sources: Schwartz's Principles of Surgery 11e, Bailey & Love's Short Practice of Surgery 28e, Current Surgical Therapy 14e, Mulholland & Greenfield's Surgery 7e, Fischer's Mastery of Surgery 8e
1. Surgical Anatomy
The spleen is the largest lymphoid organ in the body, located in the left upper quadrant (LUQ) under the ribs 9-11. Normally weighs 150-200 g and measures ~12 cm.
Blood supply:
- Splenic artery - longest, most tortuous branch of celiac artery
- Distributed type (70%): short trunk, many long branches entering >3/4 of medial surface
- Magistral type (30%): long main trunk dividing near hilum into short terminal branches
- Additional supply from short gastric vessels (via gastrosplenic ligament)
- Splenic vein joins superior mesenteric vein to form portal vein
Microstructure:
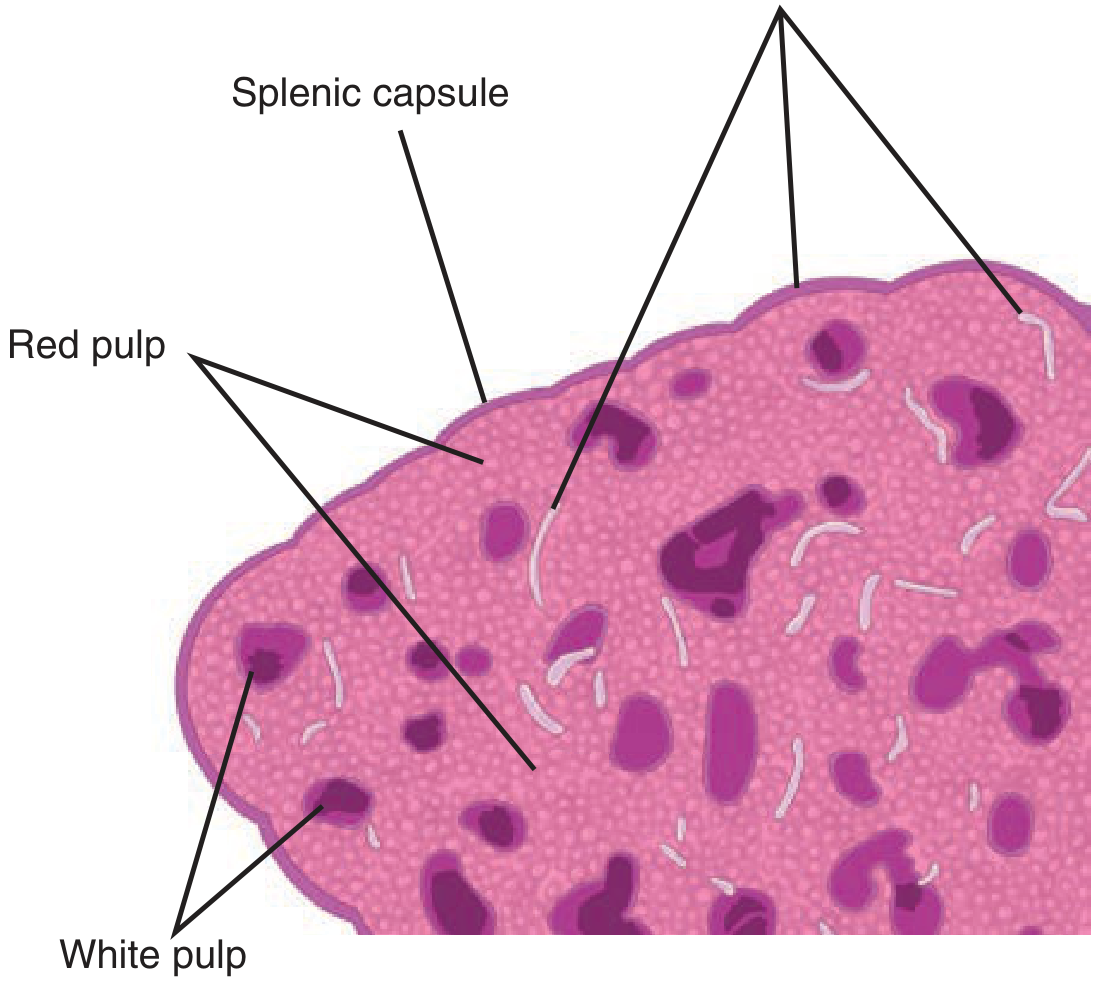
| Component | Proportion | Function |
|---|---|---|
| Red pulp | ~75% | Mechanical filtration, removes senescent RBCs, microorganisms, debris |
| White pulp | ~25% | Immunologic (T & B lymphocytes, germinal centers) |
| Marginal zone | Narrow interface | Loosely aggregated lymphocytes |
2. Functions of the Spleen
- Filtration - macrophages in red pulp remove aged erythrocytes, microorganisms, antigen-antibody complexes
- Immunity - produces IgM, opsonins (tuftsin, properdin), alternative complement pathway activation
- Hematopoiesis - extramedullary in pathologic states
- Reservoir - stores platelets and RBCs
- Phagocytosis - especially effective against poorly opsonized encapsulated bacteria (Pneumococcus, H. influenzae, Meningococcus)
3. Splenomegaly vs. Hypersplenism
These are distinct terms frequently confused:
| Feature | Splenomegaly | Hypersplenism |
|---|---|---|
| Definition | Abnormal enlargement | Cytopenias (any) with normal bone marrow |
| Size criterion | >500 g or >15 cm | Not size-dependent |
| Relationship | May coexist | May occur with or without splenomegaly |
| Massive | >1 kg or >22 cm (palpable <LCSM = at least double normal size, ~750 g) | - |
Causes of splenomegaly (classified by mechanism):
- Congestive: Portal hypertension (cirrhosis, splenic/portal vein thrombosis)
- Hematologic: Hemolytic anemias, thalassemia, sickle cell disease, ITP
- Infectious: Malaria (most common cause worldwide), EBV (infectious mononucleosis), TB, bacterial endocarditis
- Infiltrative/Storage: Gaucher's disease, amyloidosis, hemochromatosis
- Neoplastic: Lymphoma, leukemia (CML - found in ~50% of patients), myelofibrosis
- Autoimmune: Rheumatoid arthritis (Felty syndrome), SLE
4. Splenic Trauma
The most commonly injured solid organ in blunt abdominal trauma.
Grading (AAST Splenic Injury Scale)
| Grade | Description |
|---|---|
| I | Hematoma: subcapsular <10% surface; Laceration: <1 cm depth |
| II | Hematoma: subcapsular 10-50%; Laceration: 1-3 cm depth |
| III | Hematoma: subcapsular >50% or expanding; Laceration: >3 cm depth |
| IV | Laceration involving segmental/hilar vessels with >25% devascularization |
| V | Shattered spleen or hilar vascular injury |
Management Algorithm
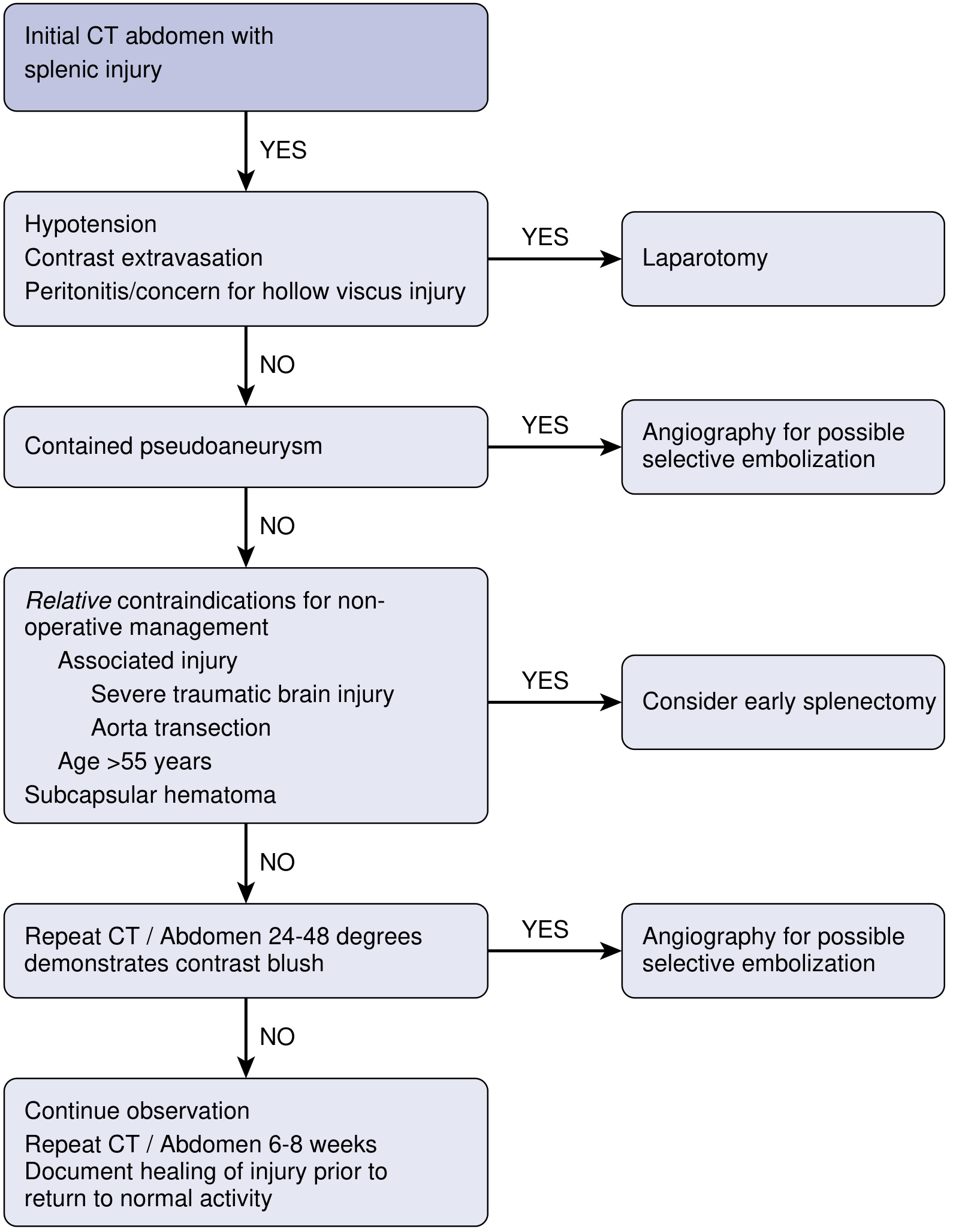
Key decision points:
- Hemodynamically unstable - immediate laparotomy and splenectomy
- Contained pseudoaneurysm - angiography + selective embolization
- Relative contraindications for NOM (age >55, severe TBI, aorta transection, subcapsular hematoma) - consider early splenectomy
- Contrast blush on CT - angioembolization
- Otherwise stable - non-operative management (NOM), repeat CT at 6-8 weeks
NOM (non-operative management) is the standard for most isolated splenic injuries in children; in adults, NOM is appropriate for hemodynamically stable patients.
Splenorrhaphy (splenic repair): In stable patients at laparotomy with small-moderate injury - pack, suture lacerations, partial resection with omental patch. ~50% of splenic mass must be preserved for adequate immune function.
5. Red Blood Cell Disorders & Hemoglobinopathies
Hereditary Spherocytosis
- Autosomal dominant defect in spectrin (red cell cytoskeletal protein)
- RBCs are spherical, rigid, trapped in splenic cords and destroyed
- Features: hemolytic anemia, jaundice, splenomegaly, gallstones
- Blood smear: spherocytes, increased osmotic fragility
- Splenectomy is curative - resolves anemia but does not correct the RBC defect
- Delayed until >4 years of age (immune maturity)
Thalassemia
- Inherited disorder of hemoglobin chain synthesis (most common single-gene genetic disease)
- Most prevalent in "thalassemia belt" (Mediterranean, Middle East, India, Southeast Asia)
- β-thalassemia major presents at 4-6 months (pallor, growth retardation, jaundice, hepatosplenomegaly)
- α-thalassemia symptomatic in utero or at birth
- Treatment: RBC transfusions (Hb >9 g/dL) + deferoxamine chelation
- Splenectomy indicated when:
- Transfusion requirement >200 mL/kg/year
- Symptomatic splenomegaly
- Painful splenic infarction
- Risk: pulmonary hypertension post-splenectomy; high rate of OPSI due to coexisting iron-overload immune deficiency
Sickle Cell Disease
- RBCs contain HbS - sickle in low-oxygen states
- Functional asplenia by age 5-6 due to repeated infarction (autosplenectomy)
- Acute splenic sequestration crisis: sudden trapping of RBCs in spleen, acute massive splenomegaly, life-threatening - treated with transfusion; splenectomy for recurrence
Autoimmune Hemolytic Anemia (AIHA)
- Warm-type (IgG): splenectomy beneficial; ~60-80% response rate
- Cold-type (IgM): splenectomy less effective
6. Platelet Disorders
Idiopathic (Immune) Thrombocytopenic Purpura (ITP)
The most common indication for elective splenectomy.
- Pathophysiology: IgG autoantibodies coat platelets → splenic macrophages destroy platelets + spleen produces anti-platelet antibodies
- Clinical: mucocutaneous bleeding, petechiae, platelet count <100,000/µL (often <20,000)
- Acute ITP: children, follows viral illness, self-limiting (90% resolve spontaneously)
- Chronic ITP: adults (female predominance), persists >6 months
Treatment ladder:
- Corticosteroids (first line) - 60-80% initial response
- IV immunoglobulin (IVIG) - rapid but temporary
- Anti-D immunoglobulin (Rh+ patients)
- Splenectomy - indicated for failure of medical therapy after 6 weeks, or platelet count <10,000 with severe bleeding
- Response rate: ~80-85% (complete + partial)
- Predictors of response: age <45, short disease duration, good initial steroid response
- Rituximab, thrombopoietin receptor agonists (eltrombopag, romiplostim) - second-line medical
- Danazol, azathioprine - third-line
Pre-op: Give vaccines 2 weeks before splenectomy; platelet transfusion given only AFTER splenic artery is ligated (otherwise consumed instantly)
7. White Blood Cell / Lymphoma Disorders
Lymphoma
- Both Hodgkin's and Non-Hodgkin's lymphoma commonly involve the spleen
- Indications for splenectomy in lymphoma:
- Symptomatic massive splenomegaly
- Hypersplenism causing cytopenias prohibiting chemotherapy
- Diagnostic staging (now largely replaced by PET-CT)
Hairy Cell Leukemia (HCL)
- Chronic B-cell lymphoproliferative disorder
- Classic triad: pancytopenia, massive splenomegaly, circulating "hairy" cells on blood smear
- TRAP (tartrate-resistant acid phosphatase) stain positive
- First-line treatment: cladribine (2-CDA) or pentostatin
- Splenectomy provides temporary hematologic improvement but cladribine is now preferred
Chronic Lymphocytic Leukemia (CLL)
- Most common leukemia in adults (Western world)
- Splenectomy indicated for symptomatic splenomegaly + hypersplenism causing cytopenia
8. Bone Marrow (Myeloproliferative) Disorders
Chronic Myelogenous Leukemia (CML)
- t(9;22) - Philadelphia chromosome (bcr-abl fusion)
- Splenomegaly in ~50% of patients
- Treatment: imatinib (tyrosine kinase inhibitor) or allogeneic stem cell transplant
- Splenectomy: palliative only for symptomatic massive splenomegaly; does not prevent blast crisis
Myelofibrosis (Agnogenic Myeloid Metaplasia - AMM)
- Clonal hematopoietic stem cell proliferation → marrow fibrosis → extramedullary hematopoiesis in spleen
- Blood smear: nucleated RBCs, teardrop poikilocytes (dacrocytes), immature myeloid elements (96% of cases)
- Only curative therapy: allogeneic bone marrow transplant (young high-risk patients)
- Splenectomy for: symptomatic splenomegaly, anemia, thrombocytopenia, portal hypertension
- Mayo Clinic 30-year data: 76% response at 1 year, 28% complication rate, 21 perioperative deaths in 314 patients
Polycythemia Vera (PV)
- Clonal proliferation of erythroid, myeloid, and megakaryocytic lineages
- Splenomegaly in majority; splenectomy for symptomatic relief
Essential Thrombocythemia (ET)
- Abnormal megakaryocyte growth → elevated platelets
- Splenomegaly in 1/3 to 1/2
- Splenectomy reserved for later stages (when myeloid metaplasia develops)
9. Splenic Abscess
Causes:
- Hematogenous spread (infective endocarditis, IV drug abuse - most common)
- Ischemia from trauma or infarct
- Direct spread from adjacent organs (pancreas, colon)
- Secondary to splenic cyst/hematoma
Organisms: Staphylococcus aureus, Streptococcus spp., Gram-negatives, Salmonella (in sickle cell patients), fungi (Candida) in immunocompromised
Clinical: fever, LUQ pain, leukocytosis; left pleural effusion on CXR ("gas in spleen" on plain film if gas-forming organisms)
Diagnosis: CT abdomen (investigation of choice)
Treatment:
- Small solitary abscess: CT-guided percutaneous drainage
- Large/multiloculated/ruptured: splenectomy + antibiotics
10. Splenic Cysts
Classification
| Type | Details |
|---|---|
| True (primary) cysts | Lined by epithelium; congenital; ~10% of nonparasitic cysts; elevated CA19-9 and CEA; found in children/teenagers |
| Pseudocysts (false cysts) | No epithelial lining; ~80% of splenic cysts; post-traumatic (liquefactive necrosis of hematoma), infarction, prolonged abscess |
| Parasitic (hydatid) | Echinococcus granulosus; do NOT aspirate (anaphylaxis risk) |
Clinical: usually asymptomatic, found incidentally; large cysts cause LUQ mass, early satiety, left shoulder pain (diaphragm irritation)
Treatment:
- Small, asymptomatic: observation
- Symptomatic or enlarging: surgery
- Preferred approach: spleen preservation (partial splenectomy, cyst decapsulation/fenestration/deroofing)
- Simple unroofing has high recurrence; decapsulation (excise anterior wall circumferentially) preferred
- Recurrent cysts: partial splenectomy
- Percutaneous drainage: controversial due to high recurrence
- Hydatid cyst: careful surgical excision without spillage (scolicidal agents)
11. Splenic Tumors
Benign Tumors
| Tumor | Origin | Notes |
|---|---|---|
| Hemangioma | Vascular (red pulp) | Most common benign splenic tumor |
| Lymphangioma | Lymphatic | Multiple cystic lesions |
| Hamartoma | Mixed | Incidental finding |
| Littoral cell angioma | Sinus lining cells | Unique to spleen |
Malignant Tumors
| Tumor | Notes |
|---|---|
| Lymphoma | Most common malignancy involving spleen (secondary); Hodgkin's and NHL |
| Angiosarcoma | Most common primary splenic malignancy; rare but aggressive; linked to vinyl chloride/thorium dioxide exposure |
| Metastases | Lung, colorectal, ovarian, melanoma, breast, pancreatic |
Splenic Peliosis
- Multiple blood-filled "cystic" cavities in red pulp due to sinusoidal dilation
- Associated with HIV, steroids, OCP, Hodgkin's lymphoma, multiple myeloma
- Risk: spontaneous rupture causing hemorrhagic shock
- Treatment: splenectomy (even when found incidentally due to bleeding risk)
12. Wandering Spleen (Ectopic Spleen)
- Spleen located in lower abdomen or pelvis (not LUQ) due to laxity of peritoneal attachments
- 10x more common in females; also seen in children
- ~50% asymptomatic
- Symptoms: acute torsion (most common) or rupture after trauma
- Treatment:
- Life-threatening hemorrhage: splenectomy
- Incidentally found or torsion without infarct: laparoscopic splenopexy (spleen-preserving)
13. Splenectomy
Indications
| Category | Specific Conditions |
|---|---|
| Trauma | Accidental; iatrogenic (during gastrectomy, pancreatectomy, colectomy) |
| Hematologic | ITP, hereditary spherocytosis, thalassemia, AIHA, HCL |
| Oncological | En bloc resection (gastrectomy, pancreatectomy); staging; symptomatic lymphoma |
| Myeloproliferative | CML, myelofibrosis, PV (palliative) |
| Others | Splenic abscess, cysts, tumors, wandering spleen, portal hypertension |
Approaches
| Approach | Indication | Notes |
|---|---|---|
| Laparoscopic | Elective, non-traumatic (ITP, spherocytosis) | Standard of care; equal hematologic outcomes, less morbidity |
| Open (midline or left subcostal) | Trauma, massive splenomegaly (>22 cm), adhesions | Midline incision for trauma (allows exploration of other injuries) |
| Robotic | Selected elective cases | Emerging |
| Partial splenectomy | Children with hypersplenism; when 50% preservation achievable | Preserves immune function |
Operative Steps (Open)
- Midline or left subcostal incision; self-retaining retractor
- Retract stomach medially; enter lesser sac via gastrosplenic ligament
- Identify and ligate splenic artery first (before vein - allows drainage of blood from spleen, reduces size)
- Control splenic vein
- Mobilize spleen medially, divide ligaments (splenophrenic, splenocolic, splenorenal)
- Careful preservation of the tail of pancreas to avoid pancreatic fistula
- Inspect splenic fossa for hemostasis
Pre-operative Preparation
- Vaccinations at least 2 weeks before elective splenectomy: Pneumococcal (23-valent), H. influenzae type B, Meningococcal, Seasonal influenza
- Blood products ready (FFP, cryoprecipitate, platelets for thrombocytopenic patients)
- For ITP: platelet transfusion given only after splenic artery ligation
- Splenic artery embolization before elective splenectomy: may reduce blood loss for massive splenomegaly (no definitive evidence)
14. Overwhelming Post-Splenectomy Infection (OPSI)
The most feared long-term complication of splenectomy.
Key Facts
| Feature | Details |
|---|---|
| Incidence | ~0.9% (all causes); adults after trauma - lower risk |
| Mortality | ~0.8% (reported); but once established, up to 50-70% mortality |
| Onset | Any time, usually within 2 years post-splenectomy; can occur decades later |
| Mechanism | Loss of opsonization (tuftsin, properdin, IgM) + impaired phagocytosis |
Causative Organisms (in order)
- Streptococcus pneumoniae (~50%) - most important
- Haemophilus influenzae type B
- Neisseria meningitidis
- Gram-negative organisms (E. coli, Klebsiella, Pseudomonas)
- Capnocytophaga canimorsus (dog bite) - classic
Clinical Presentation
- Begins as flu-like illness → rapid deterioration
- Fulminant sepsis, DIC, bilateral adrenal hemorrhage (Waterhouse-Friderichsen syndrome)
- Characteristic feature: severity disproportionate to initial symptoms
High-Risk Groups
- Children (greatest risk - immune system not mature)
- Splenectomy for hematologic malignancy (lymphoma, thalassemia)
- Within first 2 years of splenectomy
Prevention
- Vaccination (most effective strategy): ideally preoperative (2 weeks before); if emergency, give 2-3 weeks post-op when immune response recovers
- Pneumococcal (23-valent PPSV23 + PCV13)
- H. influenzae type B (Hib)
- Meningococcal (MCV4)
- Annual influenza
- Antibiotic prophylaxis:
- Children: Penicillin V 125 mg BD until age 3, then 250 mg BD until age 5 (some guidelines say lifelong)
- Adults: not universally agreed; penicillin V or amoxicillin for 2 years minimum
- Patient education: carry antibiotic card; early antibiotics at first sign of infection; avoid dog bites; take prophylaxis before dental procedures/travel
Treatment of Suspected OPSI
- Immediate IV broad-spectrum antibiotics (e.g., ceftriaxone) - do not wait for culture results
- ICU admission; aggressive resuscitation
15. Post-Splenectomy Blood Changes
Following splenectomy, expect these characteristic blood findings:
| Finding | Cause | Duration |
|---|---|---|
| Thrombocytosis (↑↑ platelets) | Loss of platelet sequestration | Peak at 1-2 weeks (can reach >1 million); may persist |
| Leukocytosis (↑ WBC) | Loss of splenic sequestration | Transient; may mimic sepsis |
| Howell-Jolly bodies | Nuclear remnants in RBCs not removed | Permanent |
| Target cells, acanthocytes | Loss of RBC remodeling | Permanent |
| Siderocytes (Pappenheimer bodies) | Iron-containing RBC inclusions | Permanent |
Note: Post-splenectomy thrombocytosis can mimic sepsis when platelet count is very high. If thrombocytosis >1,000,000/µL, antiplatelet therapy (aspirin) may be needed to reduce thrombotic risk.
16. Summary Table - Surgical Indications by Condition
| Condition | Splenectomy Role |
|---|---|
| ITP | Curative (~85%) - after failed medical therapy |
| Hereditary spherocytosis | Curative - deferred >4 years age |
| Thalassemia | Palliative - for excessive transfusion requirements |
| HCL | Largely replaced by cladribine; palliation |
| CML | Palliative for symptomatic splenomegaly only |
| Myelofibrosis | Palliative - best for symptomatic splenomegaly |
| Lymphoma | Palliative/staging |
| Splenic abscess | Drainage or splenectomy |
| Splenic cysts | Spleen-preserving preferred |
| Wandering spleen | Splenopexy preferred |
| Trauma | Splenorrhaphy or splenectomy per hemodynamic status |
Sources: Schwartz's Principles of Surgery 11e, p. 1547-1560 | Bailey and Love's Short Practice of Surgery 28e, p. 1251 | Current Surgical Therapy 14e, pp. 699, 1322 | Mulholland & Greenfield's Surgery 7e, pp. 3838-3848 | Fischer's Mastery of Surgery 8e
This is a shared conversation. Sign in to Orris to start your own chat.