Discuss pft in detail full details for md exams answer in detail
Reading File
Finding Sources
Finding Sources
Searching PubMed
"pulmonary function tests" AND interpretation
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Searching Images
flow volume loop normal obstructive restrictive spirometry
Loading Image
Loading Image
Now I have comprehensive material. Let me compile a detailed, exam-ready PFT answer.
Pulmonary Function Tests (PFT) — Complete MD Exam Answer
1. DEFINITION & OVERVIEW
Pulmonary function tests (PFTs) are a battery of tests that measure how well the lungs work, encompassing:
- Respiratory mechanics — lung volumes, airflow rates, airway resistance
- Gas exchange — diffusing capacity (DLCO)
- Ventilatory muscle strength — maximal inspiratory/expiratory pressures (MIP/MEP)
PFTs are central to the definition of obstructive and restrictive disorders, and lung function is one of the most important predictors of all-cause mortality.
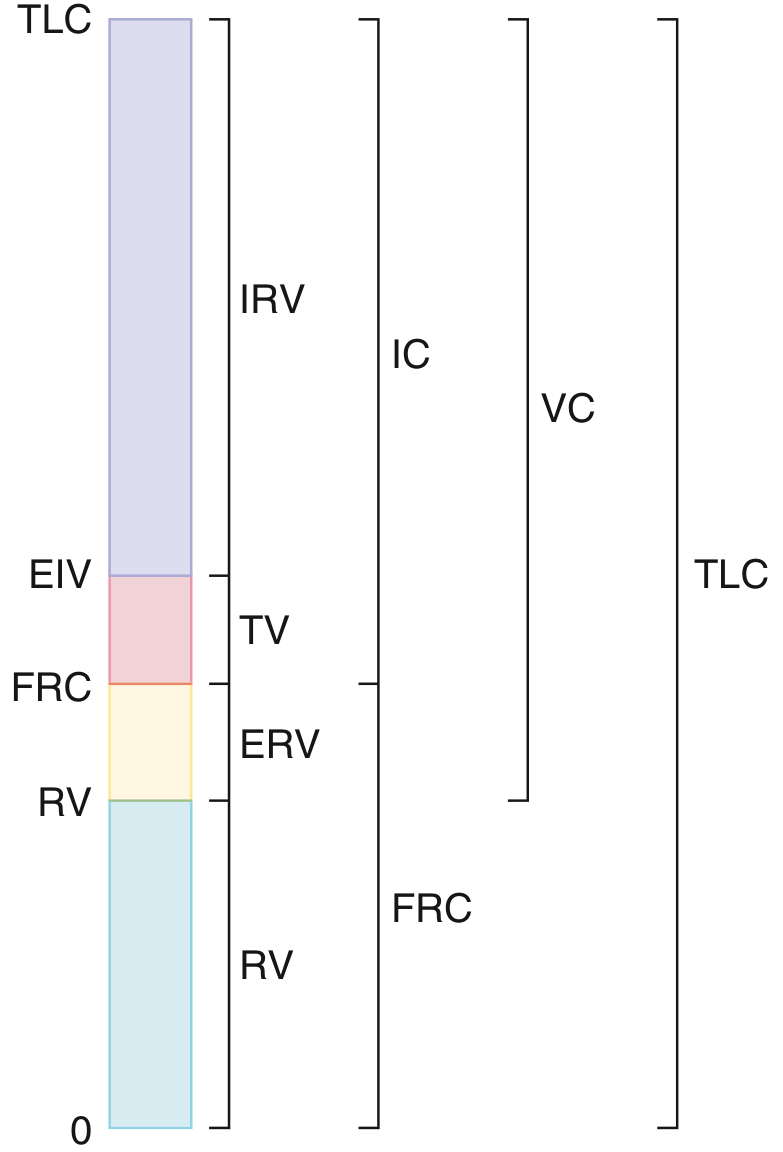
2. LUNG VOLUMES & CAPACITIES
Static Lung Volumes
| Abbreviation | Name | Definition | Normal (approx.) |
|---|---|---|---|
| TLC | Total Lung Capacity | Volume at end of maximal inspiration | ~6 L |
| FRC | Functional Residual Capacity | Volume at relaxation (inward lung pull = outward chest wall pull) | ~2.5 L |
| RV | Residual Volume | Volume after maximal exhalation (FRC − ERV) | ~1.2 L |
| ERV | Expiratory Reserve Volume | Volume expelled from FRC to RV | ~1.2 L |
| IC | Inspiratory Capacity | Volume from FRC to TLC | ~3.5 L |
| IRV | Inspiratory Reserve Volume | Volume above tidal breath to TLC | ~3 L |
| TV | Tidal Volume | Volume of a normal quiet breath | ~0.5 L |
| VC | Vital Capacity | TLC − RV | ~4.8 L |
Key relationship: TLC = VC + RV = IC + FRC
Why RV cannot be measured by simple spirometry
RV is the gas remaining after maximal exhalation — you cannot "blow it out." Therefore absolute lung volumes require:
- Body plethysmography (most accurate; can overestimate in severe obstruction if panting is too rapid)
- Inert gas dilution (helium equilibration; underestimates in bullous disease/poor communicating spaces)
- Nitrogen washout (patient breathes 100% O₂ from FRC until N₂ plateau; also underestimates in poorly communicating spaces)
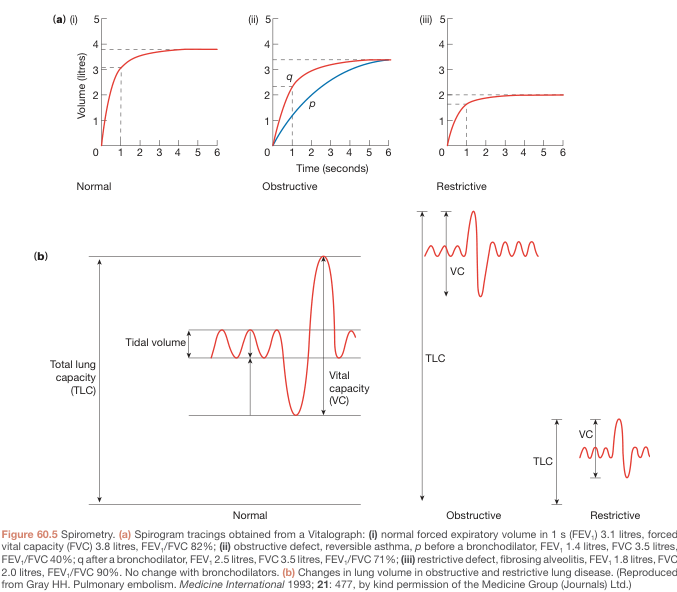
3. SPIROMETRY
FVC Maneuver
The patient inhales to TLC, then blasts out as hard and fast as possible to RV. Key parameters derived:
| Parameter | Full Name | Clinical Significance |
|---|---|---|
| FVC | Forced Vital Capacity | Total volume forcefully expelled |
| FEV₁ | Forced Expiratory Volume in 1 second | Most important single spirometric parameter |
| FEV₁/FVC | Tiffeneau index | Core ratio for obstructive vs. restrictive differentiation |
| FEF₂₅₋₇₅% | Forced expiratory flow 25–75% | Reflects small airway function; high variability (60–140% predicted normal) |
| PEF | Peak Expiratory Flow | Effort-dependent; used in asthma monitoring |
| FEV₃/FVC | — | More sensitive than FEV₁/FVC for mild obstruction (captures longer time constants) |
Normal Values
- FEV₁/FVC: ≥ 0.70 (or above the lower limit of normal, LLN)
- FVC: ≥ 80% predicted
- FEV₁: ≥ 80% predicted
ATS/ERS Standard: At least 3 acceptable spirograms; the 2 largest FVC and 2 largest FEV₁ values should be within 150 mL of each other (up to 8 efforts permitted).
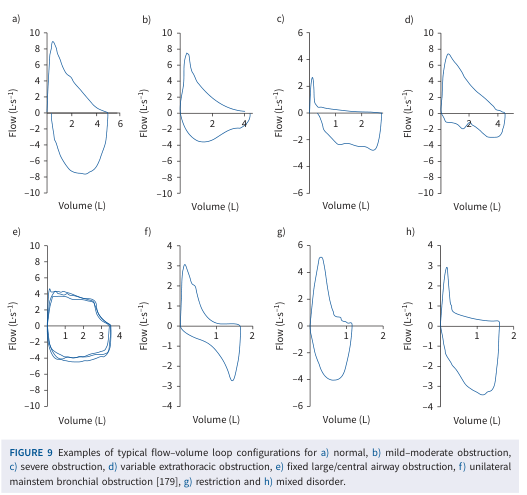
Volume–Time Curve vs. Flow–Volume Loop
- Volume–time curve: Volume on Y-axis vs. time on X-axis; plateau indicates maximal exhalation
- Flow–volume loop: Flow (L/s) on Y-axis vs. volume (L) on X-axis; the expiratory limb descends from peak flow to zero
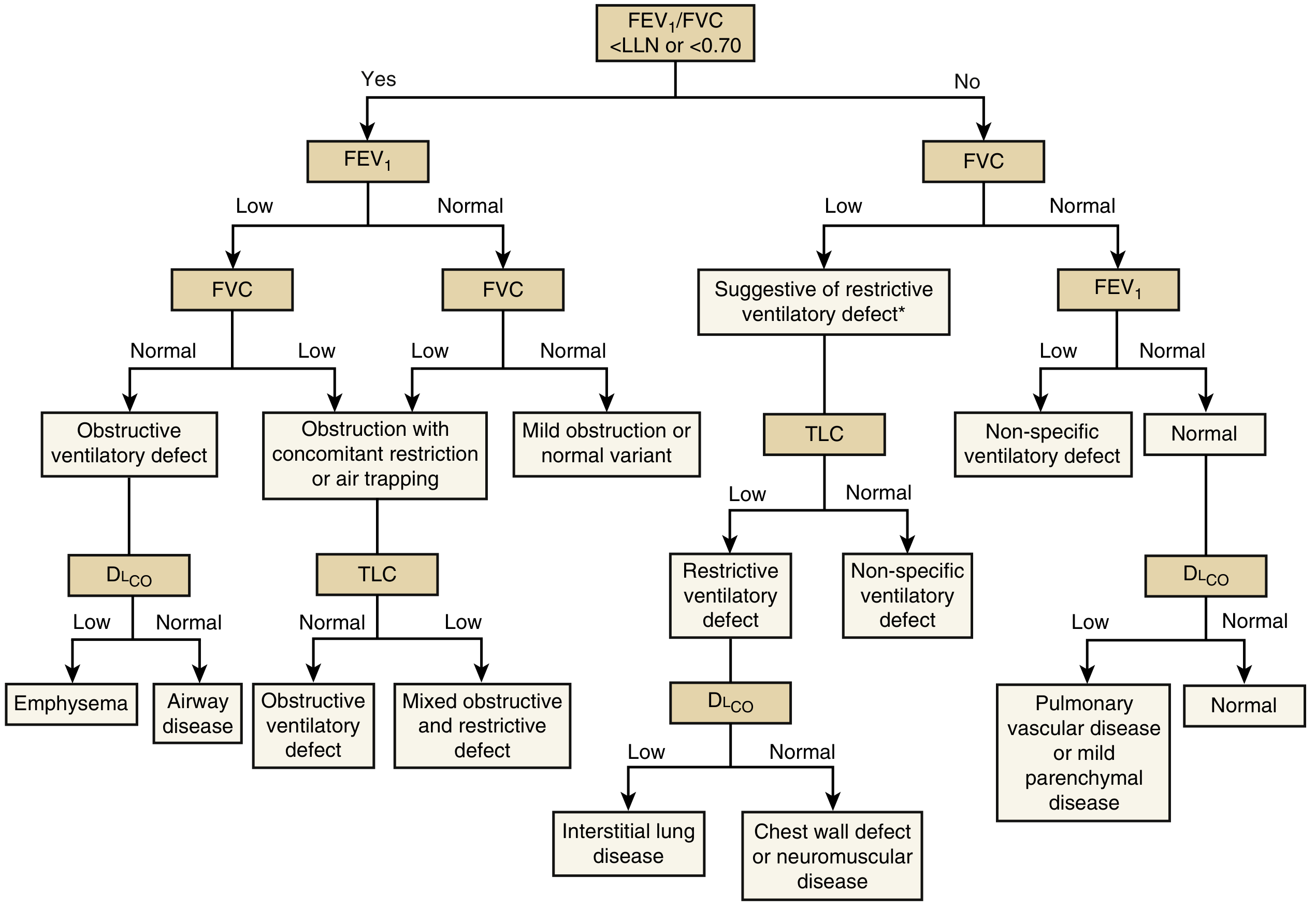
4. INTERPRETATION ALGORITHM
Step 1: Evaluate FEV₁/FVC ratio
5. PATTERNS IN DETAIL
A. Obstructive Ventilatory Defect
Diagnosis: FEV₁/FVC < LLN (or < 0.70 by fixed ratio — GOLD criteria)
Mechanism: Increased airway resistance → airflow limitation → air trapping → hyperinflation
Findings:
- ↓ FEV₁/FVC (hallmark)
- ↓ FEV₁ (reduced)
- FVC: normal or reduced (due to air trapping)
- ↑ RV, ↑ FRC, ↑ TLC (hyperinflation/air trapping)
- RV/TLC ratio elevated
- Flow–volume curve: scooped-out concave expiratory limb (characteristic)
Severity grading by FEV₁ (% predicted):
| Severity | FEV₁ % predicted |
|---|---|
| Mild | ≥ 70% |
| Moderate | 60–69% |
| Moderately severe | 50–59% |
| Severe | 35–49% |
| Very severe | < 35% |
Causes: Asthma, COPD (chronic bronchitis, emphysema), bronchiectasis, cystic fibrosis, obliterative bronchiolitis
DLCO in obstruction:
- Emphysema → ↓↓ DLCO (destruction of alveolar walls = ↓ surface area)
- Chronic bronchitis/asthma → DLCO normal or mildly reduced
B. Restrictive Ventilatory Defect
Diagnosis: FVC reduced + FEV₁/FVC normal or elevated + TLC < LLN (TLC is mandatory to confirm restriction)
Mechanism: Reduced lung compliance or chest wall restriction → small lung volumes → proportional decrease in FVC and FEV₁
Findings:
- ↓ FVC
- ↓ FEV₁ (proportionally reduced)
- FEV₁/FVC: normal or ↑ (≥ 0.70)
- ↓ TLC (confirmatory — MUST have TLC < LLN)
- RV may be normal or reduced
- Flow–volume curve: narrow, tall loop (reduced volume, preserved flows)
Causes:
| Intrinsic (parenchymal) | Extrinsic (chest wall/neuromuscular) |
|---|---|
| IPF, sarcoidosis, asbestosis, silicosis | Kyphoscoliosis, ankylosing spondylitis |
| Radiation pneumonitis | Obesity |
| Hypersensitivity pneumonitis | Neuromuscular: MG, GBS, ALS, phrenic nerve palsy |
| Pneumonectomy/lobectomy | Pleural effusion, mesothelioma |
DLCO:
- Parenchymal ILD → ↓ DLCO (thickened alveolar membrane)
- Chest wall/neuromuscular → Normal DLCO (intrinsic gas exchange intact)
C. Mixed Obstructive-Restrictive Defect
Diagnosis: FEV₁/FVC < LLN AND TLC < LLN
Findings: Features of both obstruction and restriction coexist. Requires TLC measurement to diagnose.
Causes: Sarcoidosis with airway involvement, cystic fibrosis (late), combined ILD + emphysema
D. Nonspecific Ventilatory Pattern
Diagnosis: FEV₁/FVC normal + FVC ↓ (or FEV₁ ↓) + TLC normal
Significance: Does not fit classic obstructive or restrictive definition. May represent:
- Early restriction (TLC at lower end of normal)
- Mixed obstructive disease with air trapping masking reduced FVC
- Small airway disease
6. DIFFUSING CAPACITY (DLCO / TLCO / Transfer Factor)
Principle
- Patient exhales to RV → rapidly inhales a mixture of CO + inert tracer gas (He or CH₄) to TLC → breath-hold for 10 seconds → exhale
- CO is measured before and after; the inert gas measures alveolar volume (VA)
- DLCO = rate of CO uptake / driving pressure
Transfer coefficient: Kco = DLCO / VA (corrects for lung volume)
Normal DLCO
- ≥ 75% predicted (LLN: typically ~70% predicted)
- Corrected for hemoglobin (anemia → falsely low; polycythemia → falsely high)
- Corrected for COHb (smokers)
- Altitude: lower PIO₂ → DLCO appears increased
Interpretation of DLCO Changes
| DLCO | Pattern | Causes |
|---|---|---|
| ↓↓ DLCO | Obstructive pattern | Emphysema (destruction of alveolar surface area) |
| ↓ DLCO | Restrictive + parenchymal | ILD, sarcoidosis, asbestosis, pulmonary edema |
| Normal DLCO | Restrictive, extrapulmonary | Chest wall disease, neuromuscular disease, obesity |
| Normal DLCO | Obstructive | Asthma, chronic bronchitis (no parenchymal loss) |
| ↑ DLCO | — | Pulmonary hemorrhage (Hb in alveoli binds CO), polycythemia, left-to-right shunts, exercise |
| ↓ DLCO isolated | Normal spirometry + normal TLC | Pulmonary vascular disease (PE, pulmonary HTN), mild parenchymal disease |
7. FLOW-VOLUME LOOP PATTERNS IN SPECIFIC CONDITIONS
Upper Airway Obstruction (UAO)
| Type | Location | Effect | Pattern on Loop |
|---|---|---|---|
| Fixed obstruction (tracheal stenosis, goiter) | Above or below thoracic inlet | Equal limitation in both phases | Plateau in both inspiratory AND expiratory limbs |
| Variable extrathoracic (vocal cord paralysis, tracheomalacia above inlet) | Above thoracic inlet | Worsens on inspiration (negative pressure collapses airway) | Plateau in inspiratory limb only |
| Variable intrathoracic (tracheomalacia below inlet) | Below thoracic inlet | Worsens on exhalation (positive pleural pressure compresses airway) | Plateau in expiratory limb only |
Emphysema
- Scooped-out expiratory limb
- "Negative effort dependence" — tidal flow may exceed forced expiratory flow (highly collapsible airways collapse more during forced effort)
- Increased RV, FRC, TLC
8. BRONCHODILATOR RESPONSE TESTING
Protocol
- Administer SABA (salbutamol 400 mcg via MDI + spacer, or 2.5 mg nebulized); reassess after 15–20 minutes
- OR LABA (salmeterol, formoterol); reassess after 30–60 minutes
Positive (Significant) Bronchodilator Response (ATS/ERS 2022):
- ≥ 10% increase in FEV₁ or FVC relative to predicted AND absolute increase ≥ 200 mL
- (Older criteria: ≥ 12% AND ≥ 200 mL increase from baseline — still widely used for MD exams)
Clinical interpretation
- Complete reversibility (FEV₁/FVC normalizes): suggests asthma
- Partial/incomplete reversibility: COPD or incompletely controlled asthma
- No reversibility: established COPD
- Significant response does NOT exclude COPD; absence does NOT exclude asthma
9. BRONCHIAL CHALLENGE TESTING
Used when spirometry is normal but asthma is suspected (e.g., chronic cough, exercise-induced symptoms).
Methacholine Challenge
- Principle: Inhalation of progressive concentrations of methacholine (muscarinic agonist)
- Endpoint: PC₂₀ — concentration causing 20% fall in FEV₁
- Interpretation:
- PC₂₀ < 1 mg/mL: moderate–severe hyperresponsiveness (asthma very likely)
- PC₂₀ 1–4 mg/mL: borderline
- PC₂₀ 4–16 mg/mL: mild hyperresponsiveness (possible asthma)
- PC₂₀ > 16 mg/mL: normal (asthma unlikely)
Other Stimuli
- Exercise challenge (EIB diagnosis): ≥ 10–15% fall in FEV₁ after exercise = positive
- Mannitol challenge: dry powder osmotic stimulus; high specificity for asthma
- Eucapnic voluntary hyperpnoea (EVH): used in athletes
10. RESPIRATORY MUSCLE STRENGTH
| Test | Measurement | Normal | Interpretation |
|---|---|---|---|
| MIP (PImax) | Maximal inspiratory pressure at RV | > −80 cmH₂O (men); > −70 cmH₂O (women) | ↓ = diaphragm/inspiratory muscle weakness |
| MEP (PEmax) | Maximal expiratory pressure at TLC | > +80 cmH₂O | ↓ = expiratory muscle weakness (↓ cough efficacy) |
| Sniff nasal inspiratory pressure (SNIP) | Diaphragm strength | — | Sensitive test; reduced in phrenic nerve palsy |
Indications: Neuromuscular diseases (MG, GBS, ALS, Duchenne MD), unexplained dyspnea or hypercapnia with low spirometry but normal TLC
PFT pattern in neuromuscular disease:
- Reduction in FVC (often supine FVC drops > 20% vs. erect → indicates diaphragm weakness)
- Normal FEV₁/FVC
- Normal DLCO
- ↓ MIP and MEP
11. FACTORS AFFECTING PFT RESULTS
Patient factors
| Factor | Effect |
|---|---|
| Height | ↑ height → ↑ all lung volumes |
| Age | TLC minimally changed; FVC and FEV₁ decrease (−21 to −33 mL/yr in men); RV increases |
| Sex | Men > women for most volumes |
| Ethnicity/Race | African-Americans and Asian subjects have ~10–15% lower lung volumes than White subjects at same height (controversial; ATS 2022 moving toward race-neutral equations) |
| Obesity | ↓ FRC and ERV; restrictive-like pattern possible |
| Smoking | Accelerated decline in FEV₁ (~45 mL/yr vs. ~25 mL/yr in non-smokers) |
| Posture | Supine → ↓ FRC (especially in obesity/neuromuscular disease) |
Technical/analytical factors
- Poor effort → falsely low FVC and FEV₁
- Air leaks, calibration errors
- Medication effects (bronchodilators must be withheld: SABA 4–6 hrs, LABA 12–24 hrs before testing if reversibility is being assessed)
12. SEVERITY CLASSIFICATION
GOLD Staging (Obstructive — post-bronchodilator):
| GOLD Stage | FEV₁ % predicted |
|---|---|
| 1 (Mild) | ≥ 80% |
| 2 (Moderate) | 50–79% |
| 3 (Severe) | 30–49% |
| 4 (Very Severe) | < 30% |
Restrictive Disease Severity (ATS/ERS):
| Severity | TLC or FVC % predicted |
|---|---|
| Mild | 70–80% |
| Moderate | 60–69% |
| Moderately severe | 51–59% |
| Severe | 41–50% |
| Very severe | ≤ 40% |
13. SPECIAL APPLICATIONS OF PFT
| Clinical Scenario | PFT Role |
|---|---|
| Pre-operative assessment | FEV₁ < 40% predicted or ppoFEV₁ < 30% → ↑ post-op pulmonary complication risk; ppoFEV₁ < 40% → relative contraindication for pneumonectomy |
| Disability assessment | Objective functional impairment quantification |
| Asthma control monitoring | Serial FEV₁/PEF measurements |
| ILD monitoring | ≥ 10% relative decline in FVC over 6–12 months = significant progression (predicts mortality in IPF) |
| Lung transplant listing | FVC < 50% in ILD; FEV₁ < 20% + DLCO < 20% or homogeneous emphysema → transplant evaluation |
| Lung volume reduction surgery (LVRS) | FEV₁ 20–45%, TLC > 100%, RV > 150%, upper lobe predominant emphysema |
| Monitoring after COVID-19 | ~70% of moderate-severe survivors have DLCO abnormalities at 6 weeks; ~25% obstructive, ~20% restrictive |
14. SUMMARY TABLE — CLASSIC EXAM PATTERNS
| Pattern | FEV₁/FVC | FEV₁ | FVC | TLC | RV | DLCO |
|---|---|---|---|---|---|---|
| Normal | ≥ 0.70 | ≥ 80% | ≥ 80% | N | N | N |
| Obstructive (airway) | ↓ | ↓ | N or ↓ | N or ↑ | ↑ | N |
| Emphysema | ↓ | ↓↓ | ↓ | ↑ | ↑↑ | ↓↓ |
| Restrictive (ILD) | N or ↑ | ↓ | ↓↓ | ↓ | ↓ | ↓ |
| Restrictive (chest wall/NMD) | N or ↑ | ↓ | ↓↓ | ↓ | N or ↓ | N |
| Mixed | ↓ | ↓↓ | ↓↓ | ↓ | variable | ↓ |
| Pulmonary HTN / vascular | N | N | N | N | N | ↓↓ |
| Pulmonary hemorrhage | N | N | N | N | N | ↑↑ |
| Neuromuscular | N or ↑ | ↓ | ↓ | ↓ | N or ↑ | N |
15. KEY EXAM POINTS (HIGH-YIELD)
- FEV₁/FVC < 0.70 (or < LLN) = obstructive; requires TLC to distinguish "obstruction with air trapping" from "mixed"
- TLC < LLN is mandatory to confirm restriction — spirometry alone cannot diagnose restriction
- DLCO ↑ = pulmonary hemorrhage, polycythemia, left-to-right shunt
- DLCO ↓ in isolation (normal spirometry + normal TLC) = pulmonary vascular disease
- Emphysema: FEV₁/FVC ↓ + RV ↑↑ + TLC ↑ + DLCO ↓↓
- Asthma: FEV₁/FVC ↓ + significant reversibility (≥ 12% and ≥ 200 mL) + normal DLCO
- Neuromuscular disease: reduced FVC and TLC, normal FEV₁/FVC, normal DLCO, ↓ MIP/MEP; supine FVC falls > 20% = diaphragm weakness
- Fixed upper airway obstruction: plateau on BOTH inspiratory and expiratory limbs
- FEF₂₅₋₇₅%: small airway marker; high variability — use with caution in isolation
- Helium dilution underestimates TLC in emphysema (bullae don't communicate); body plethysmography is the gold standard
Sources: Murray & Nadel's Textbook of Respiratory Medicine; Goldman-Cecil Medicine; Fishman's Pulmonary Diseases & Disorders; Bailey & Love's Surgery; ATS/ERS Technical Standard on Lung Function Interpretation (PMID 40084848, 38999220)
This is a shared conversation. Sign in to Orris to start your own chat.