Prostthetic heart valves in detail
Reading File
Finding Sources
Searching PubMed
"prosthetic heart valve"[MeSH Terms] AND "review"[pt]
Finding Sources
Searching PubMed
"heart valve prosthesis"[MeSH Terms] AND "anticoagulation"
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive material from multiple authoritative textbooks. Let me compile the full detailed answer.
Prosthetic Heart Valves - A Comprehensive Overview
1. Introduction
A prosthetic heart valve (PHV) is a device surgically or percutaneously implanted to replace a diseased native cardiac valve that cannot be repaired. The most commonly replaced valves are the aortic and mitral valves. The two fundamental categories are mechanical heart valves (MHV) and biological (bioprosthetic) heart valves (BHV). The primary trade-off between them is: MHVs are highly durable but require lifelong anticoagulation, while BHVs avoid long-term anticoagulation but undergo structural valve deterioration (SVD) over time.
2. Classification and Design
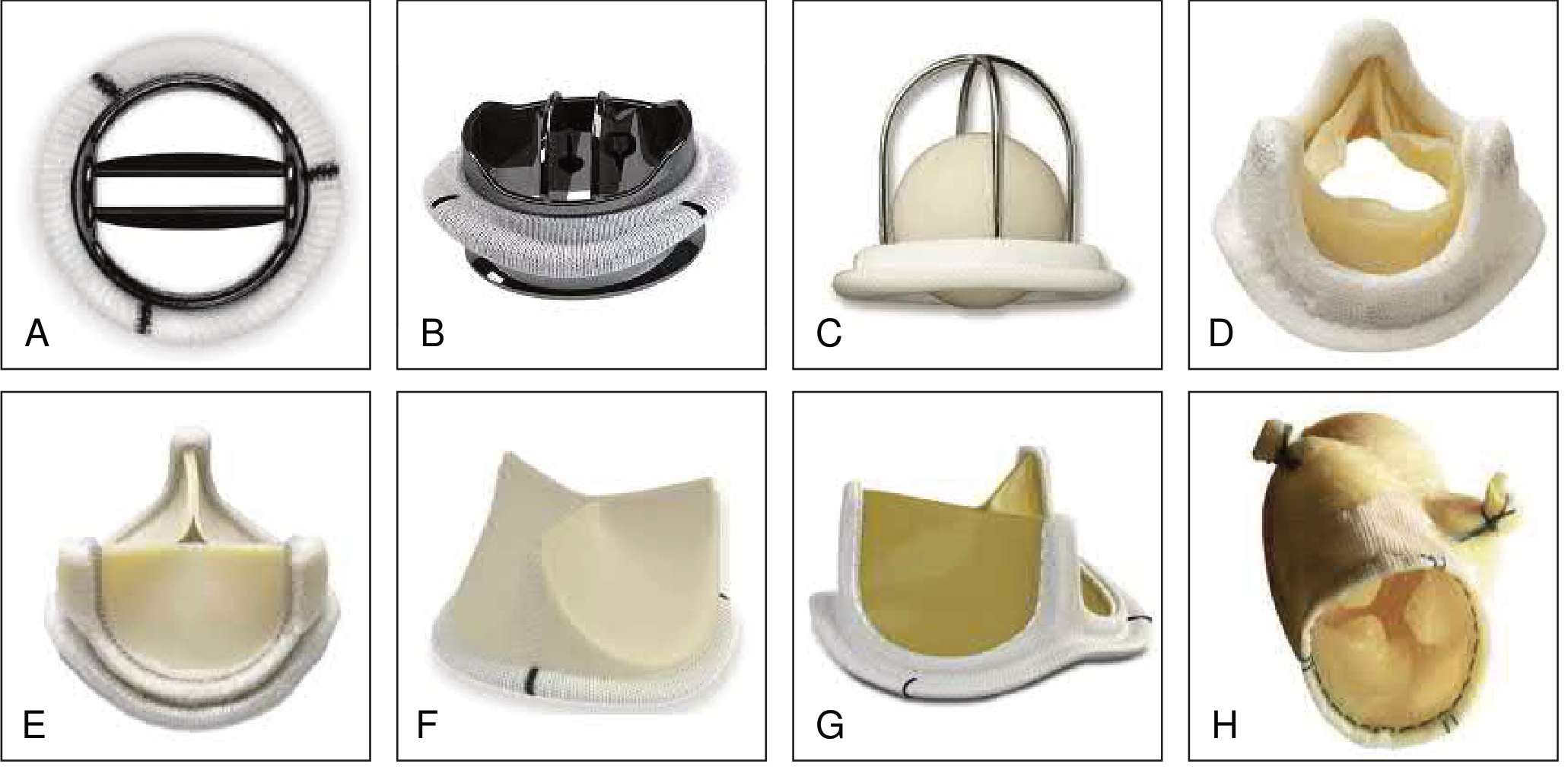
Figure: Different types and models of prosthetic valves (Braunwald's Heart Disease)
A. Mechanical Heart Valves (MHVs)
| Type | Design | Notes |
|---|---|---|
| Bileaflet | Two semicircular pyrolytic carbon leaflets pivot on hinges | Most widely used today (e.g., St. Jude Medical, Carbomedics, Oni-X) |
| Tilting disc (monoleaflet) | Single circular disc rotates on lateral/central metal struts; opens 60-80 degrees | Creates two unequal orifices (e.g., Bjork-Shiley, Medtronic Hall, Omnicarbon) |
| Ball-and-cage (Starr-Edwards) | Silastic ball moves within a metal cage | Oldest type (first used 1965); no longer implanted; most thrombogenic |
Key features of MHVs:
- Made from pyrolytic carbon - highly durable (>35-45 years freedom from SVD)
- Bileaflet valves have small "washing jets" (normal regurgitation from hinge points) that reduce thrombus formation
- 10-year freedom from valve-related death >90% for St. Jude and Carbomedics bileaflet valves
- All require lifelong anticoagulation with VKA
B. Biological (Bioprosthetic) Heart Valves (BHVs)
1. Stented Bioprostheses
- Three biologic leaflets (porcine aortic valve or bovine pericardium) treated with glutaraldehyde to reduce antigenicity, mounted on a metal/polymer stented ring
- Open to a circular orifice in systole, resembling native aortic valve anatomy
- Most treated with anti-calcifying agents
- Examples: Medtronic Mosaic (porcine), Edwards Magna / Carpentier-Edwards Perimount (bovine pericardial)
- The Edwards Inspiris Resilia incorporates newer anti-calcification technology and an expandable sewing ring designed for future valve-in-valve implantation
2. Stentless Bioprostheses
- No rigid support frame; leaflets mounted directly
- Better hemodynamics (larger effective orifice area), potentially slower SVD
- Example: Medtronic Freestyle (porcine)
- Technically more demanding to implant
3. Homografts (Allografts)
- Cadaveric human aortic or pulmonary valves
- Excellent hemodynamics and resistance to endocarditis
- Rarely used due to limited supply; most commonly used for pulmonary valve replacement
- No anticoagulation needed
4. Autografts (Ross Procedure)
- Patient's own pulmonary valve translocated to aortic position; pulmonary valve replaced with homograft
- Excellent durability and hemodynamics; grows with patient (ideal for children/young adults)
- Two valves at risk; technically demanding; risk of neoaortic dilation
5. Transcatheter Heart Valves (TAVR)
- Balloon-expandable (e.g., Edwards SAPIEN 3, SAPIEN 3 Ultra)
- Self-expanding (e.g., Medtronic CoreValve Evolut R, Evolut PRO)
- Used for patients at intermediate-to-high surgical risk with aortic stenosis; increasingly used in lower-risk patients
- Sutureless valves (e.g., Sorin Perceval) reduce operative times for surgical implantation
3. Advantages and Disadvantages
| Feature | Mechanical Valve | Bioprosthetic Valve |
|---|---|---|
| Durability | Excellent (>35 yrs) | Limited (10-20 yrs; accelerated in young patients) |
| Anticoagulation | Lifelong VKA required | Not needed (low thromboembolism risk) |
| Thromboembolism risk | Higher (requires anticoagulation) | Low (~0.04-0.34%/year without anticoagulation) |
| Catastrophic failure | Possible (disc embolism - rare now) | Rarely catastrophic; gradual SVD |
| Hemolysis | Possible | Rare |
| Endocarditis | Possible (similar rates) | Possible (some data suggest higher for bioprosthetic AVR) |
| Valve sounds | Audible mechanical clicks | Silent |
| Pregnancy | Anticoagulation management complex | Preferred in women planning pregnancy |
4. Choosing a Prosthetic Valve
The decision is made by the heart valve team through shared decision-making, incorporating patient preferences and lifestyle. Both AHA/ACC and ESC guidelines emphasize this approach.
Factors favoring MHV:
- No contraindication to long-term anticoagulation (low bleeding risk, good compliance)
- Increased risk of accelerated SVD (age <40, hyperparathyroidism)
- Existing indication for anticoagulation (existing mechanical prosthesis elsewhere, high thromboembolism risk, AF)
- Reasonable life expectancy beyond bioprosthesis durability
- High reoperation risk (porcelain aorta, prior radiation)
Factors favoring BHV:
- Contraindication to anticoagulation (high bleeding risk, poor compliance)
- Reoperation for mechanical valve thrombosis despite adequate anticoagulation
- Low reoperation risk
- Young women contemplating pregnancy
- Patient preference/lifestyle (e.g., contact sports, occupations with injury risk)
- Life expectancy less than presumed bioprosthesis durability
Age cutoffs (guideline differences):
- ACC/AHA: MHV preferred at age <50 years
- ESC: MHV preferred at age <60 years (aortic), <65 years (mitral)
- The trend toward bioprostheses in younger patients has accelerated due to improved new-generation durability and the availability of transcatheter valve-in-valve procedures for degenerated BHVs
(Fuster and Hurst's The Heart, 15th Edition)
5. Antithrombotic Therapy
Mechanical Heart Valves
- VKA (warfarin) is mandatory lifelong - prevents valve thrombosis and embolic events
- NOACs are contraindicated in patients with MHV (RE-ALIGN trial showed worse outcomes with dabigatran)
- INR monitoring: 2-3x/week when initiating, then at least monthly when stable
- Dedicated anticoagulation clinics improve outcomes vs. standard monitoring
INR targets:
- Mechanical AVR with no risk factors: INR 2.5
- Mechanical AVR with risk factors (AF, prior thromboembolism, LV dysfunction, hypercoagulable state) or older-generation valve: INR 3.0
- Mechanical MVR: INR 3.0
- Aspirin is no longer routinely added to VKA in the absence of other indications
Perioperative bridging:
- Minor procedures (dental): continue VKA with therapeutic INR
- Bileaflet mechanical AVR with no thrombosis risk factors: temporary interruption WITHOUT bridging is acceptable
- Bridging anticoagulation (LMWH or UFH) is reasonable for mechanical AVR with thromboembolic risk factors undergoing invasive procedures
- Bridging with UFH is recommended for mechanical MVR undergoing invasive procedures
Biological Heart Valves
- No routine anticoagulation required long-term
- Aspirin 75-100 mg/day is reasonable for all patients with a bioprosthetic aortic or mitral valve (Class IIa)
- Short-term anticoagulation (first 3 months after implantation) with VKA is reasonable in some guidelines for surgical bioprostheses
Transcatheter Heart Valves
- Managed per individual risk-benefit assessment; antiplatelet therapy commonly used
(Washington Manual of Medical Therapeutics; Fuster and Hurst's The Heart)
6. Complications
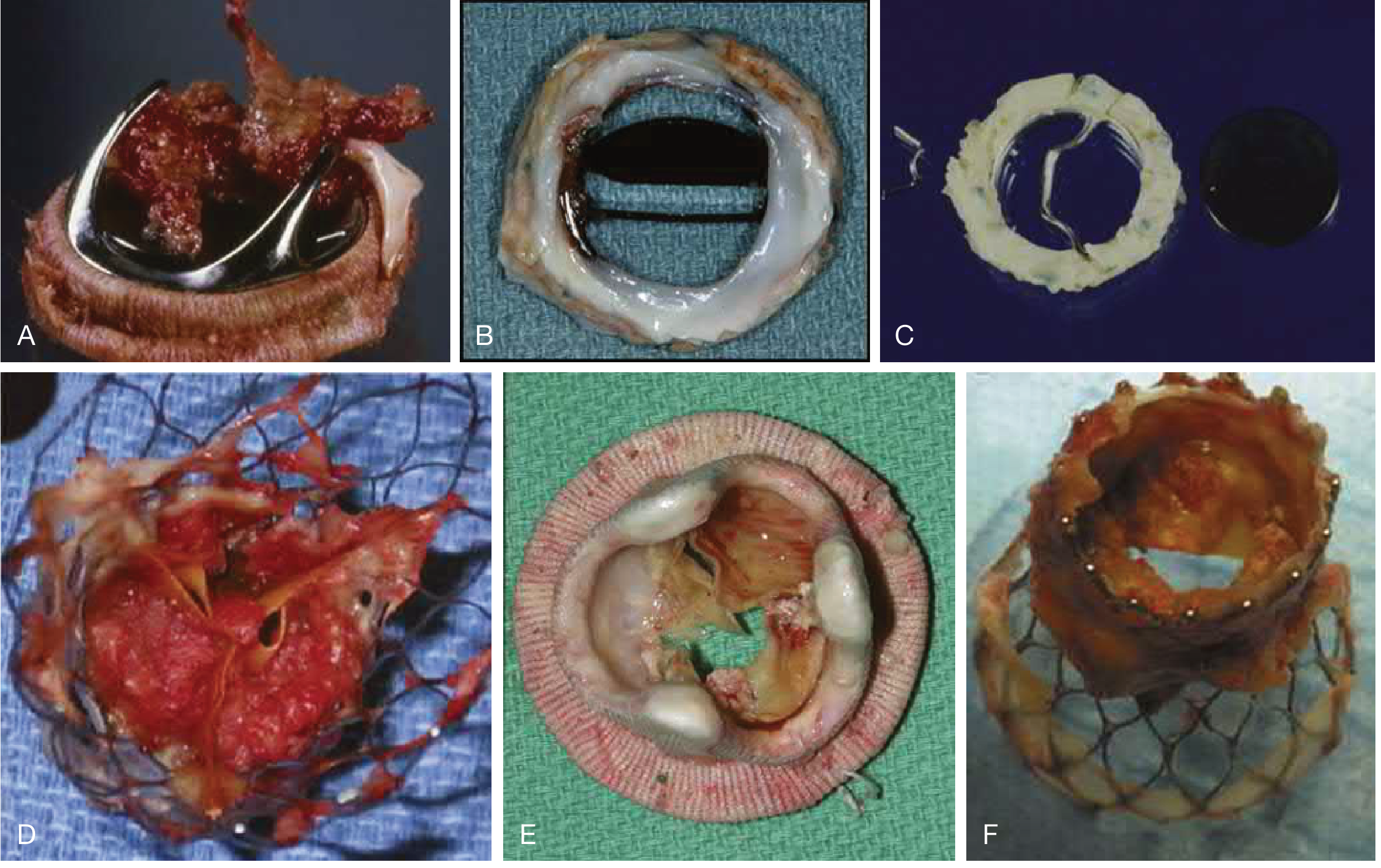
Figure: Prosthetic valve complications (Braunwald's Heart Disease)
6a. Structural Valve Deterioration (SVD)
- MHVs: SVD is extremely rare with modern valves
- BHVs: Major mode of failure. Caused by leaflet calcification, fibrosis, tears, and perforations (lipid infiltration, inflammation, immune rejection, active mineralization)
- SVD begins within 5-7 years for earlier generations, varies by position and age at implant
- Mitral bioprostheses fail earlier than aortic ones (higher LV closing pressures)
- Process accelerated in: younger patients, disordered calcium metabolism, end-stage renal disease
- Treatment: valve-in-valve TAVR (increasingly preferred over redo surgery in high-risk patients)
6b. Prosthetic Valve Thrombosis (PVT)
- More common with MHVs (subtherapeutic anticoagulation is the main cause)
- Can also occur with transcatheter valves (subclinical leaflet thrombosis detected by CT)
- Diagnosis: echocardiography (TEE preferred), cinefluoroscopy
- Treatment: fibrinolytic therapy (for non-obstructive or high-risk surgery), emergency surgery (for obstructive thrombosis in hemodynamically compromised patients)
6c. Prosthetic Valve Endocarditis (PVE)
- Incidence: 1-6% of patients with valve prostheses
- Associated with poor prognosis
- Similar rates in MHV vs. BHV overall; some data suggest higher early (<1 year) infection with MHV, and higher rates of both early and late PVE with bioprosthetic AVR
- Organisms: Staphylococci (early PVE), Streptococci, Enterococci (late PVE)
- Diagnosis requires careful integration of echocardiography, blood cultures, clinical data (Duke Criteria)
- Management: prolonged IV antibiotics; surgery often needed for complicated cases
6d. Paravalvular Leak (PVL)
- Incomplete seating of the sewing ring leads to regurgitation outside the prosthesis
- Can cause hemolysis and heart failure
- More common after TAVR than surgical valve replacement
- Treatment: redo surgery, catheter-based closure, or medical palliation
6e. Patient-Prosthesis Mismatch (PPM)
- Occurs when the implanted valve is too small for the patient's body size (cardiac output requirements), resulting in abnormally high postoperative gradients
- Defined by indexed Effective Orifice Area (EOAI):
- Aortic: PPM = EOAI <0.85 cm²/m²; Severe = <0.65 cm²/m²
- Mitral: PPM = EOAI <1.2 cm²/m²; Severe = <0.5 cm²/m²
- In obese patients (BMI ≥30): lower cutoffs (severe aortic PPM = <0.55 cm²/m²; severe mitral PPM = <0.75 cm²/m²)
- Prevalence: 20-70% after SAVR and >50% after MVR (moderate PPM); severe PPM 2-20%
- TAVR has lower PPM risk than SAVR, especially with self-expanding supra-annular designs
- Consequences: worse functional class, reduced LV hypertrophy regression, increased heart failure, pulmonary hypertension, and mortality
- Prevention: aortic root enlargement to allow larger prosthesis; use the projected EOAI before surgery
- Treatment options are limited; reintervention only if severe symptoms unresponsive to medical therapy
6f. Hemolysis
- Microangiopathic hemolytic anemia from turbulent blood flow across the prosthesis
- More common with perivalvular leaks; can also occur with normally functioning MHVs
- Markers: elevated LDH, low haptoglobin, schistocytes on blood smear
6g. Pannus Ingrowth
- Fibrous tissue overgrowth from the sewing ring into the orifice of MHVs
- Causes reduced leaflet opening and prosthetic valve obstruction
- Differentiated from thrombus by imaging (CT, TEE) and clinical context
7. Echocardiographic Assessment
Echocardiography (TTE/TEE) is the primary modality for evaluating prosthetic valve function.
Aortic prosthetic valve - obstruction thresholds:
| Parameter | Possible Obstruction | Significant Obstruction |
|---|---|---|
| Vmax | 3-3.9 m/s | ≥4 m/s |
| Mean pressure gradient (MPG) | 20-34 mmHg | ≥35 mmHg |
| Effective orifice area (EOA) | 0.8-1.1 cm² | <0.8 cm² |
| Doppler Velocity Index (DVI) | 0.25-0.34 | <0.25 |
Mitral prosthetic valve - obstruction thresholds:
| Parameter | Possible Obstruction | Significant Obstruction |
|---|---|---|
| Vmax | 1.9-2.5 m/s | >2.5 m/s |
| MPG | 6-10 mmHg | >10 mmHg |
| EOA | 1-2 cm² | <1 cm² |
| Pressure half-time (PHT) | 130-200 ms | >200 ms |
- Bileaflet MHVs have normal small "washing jets" - two converging jets at hinge points
- TEE is superior to TTE for evaluating prosthetic valves, particularly mitral prostheses (acoustic shadowing)
- Cinefluoroscopy assesses leaflet motion in MHVs
- CT is increasingly used for subclinical leaflet thrombosis (especially in TAVR) and pre-procedural planning
(Textbook of Clinical Echocardiography; Fuster and Hurst's The Heart)
8. Follow-Up Protocol
- Baseline TTE within 30 days of implantation (establishes reference values)
- Annual clinical evaluation
- Echo when there is a change in symptoms, new murmur, or concerning clinical finding
- For TAVR patients: CT at 1-3 months to screen for subclinical leaflet thrombosis
- Long-term monitoring for SVD, PVL, endocarditis, PPM
9. Special Considerations
Pregnancy
- MHVs pose anticoagulation management challenges during pregnancy
- Warfarin crosses the placenta (teratogenic in 1st trimester, fetal hemorrhage risk)
- LMWH can be used as an alternative but carries higher valve thrombosis risk
- BHV preferred in women of childbearing age; SVD may be accelerated by pregnancy
Infective Endocarditis Prophylaxis
- All prosthetic valve patients require IE prophylaxis (dental, invasive oropharyngeal procedures)
Recent Evidence (PubMed, 2024-2025)
- A 2025 meta-analysis (PMID: 40997282) in Neurology examined the timing of anticoagulation reinitiation after intracranial hemorrhage in patients with mechanical valves - a high-stakes clinical scenario where delaying VKA carries thromboembolism risk but early resumption increases rebleeding risk.
- A 2025 JACC comparative study (PMID: 40139884) compared bioprosthetic vs. mechanical AVR in patients aged 40-75 years, reflecting ongoing refinement of the age cutoffs in guidelines.
Key References:
- Braunwald's Heart Disease, 2-Vol Set, A Textbook of Cardiovascular Medicine - Chapter 79: Prosthetic Heart Valves
- Fuster and Hurst's The Heart, 15th Edition - Chapter 29
- Textbook of Clinical Echocardiography - Chapter 13
- Washington Manual of Medical Therapeutics
This is a shared conversation. Sign in to Orris to start your own chat.