Musculocutaneous nerve
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
I now have comprehensive information from multiple authoritative textbooks. Let me compile the full answer.
Musculocutaneous Nerve
Origin and Roots
The musculocutaneous nerve arises from the lateral cord of the brachial plexus, carrying fibers from C5, C6, and C7 (primarily C5-C6 for motor, with C7 contributing in some sources). It is the most proximal of the major nerves to emerge from the brachial plexus.
- Gray's Anatomy for Students, p. 879
- Imaging Anatomy Vol. 3, p. 191
Course
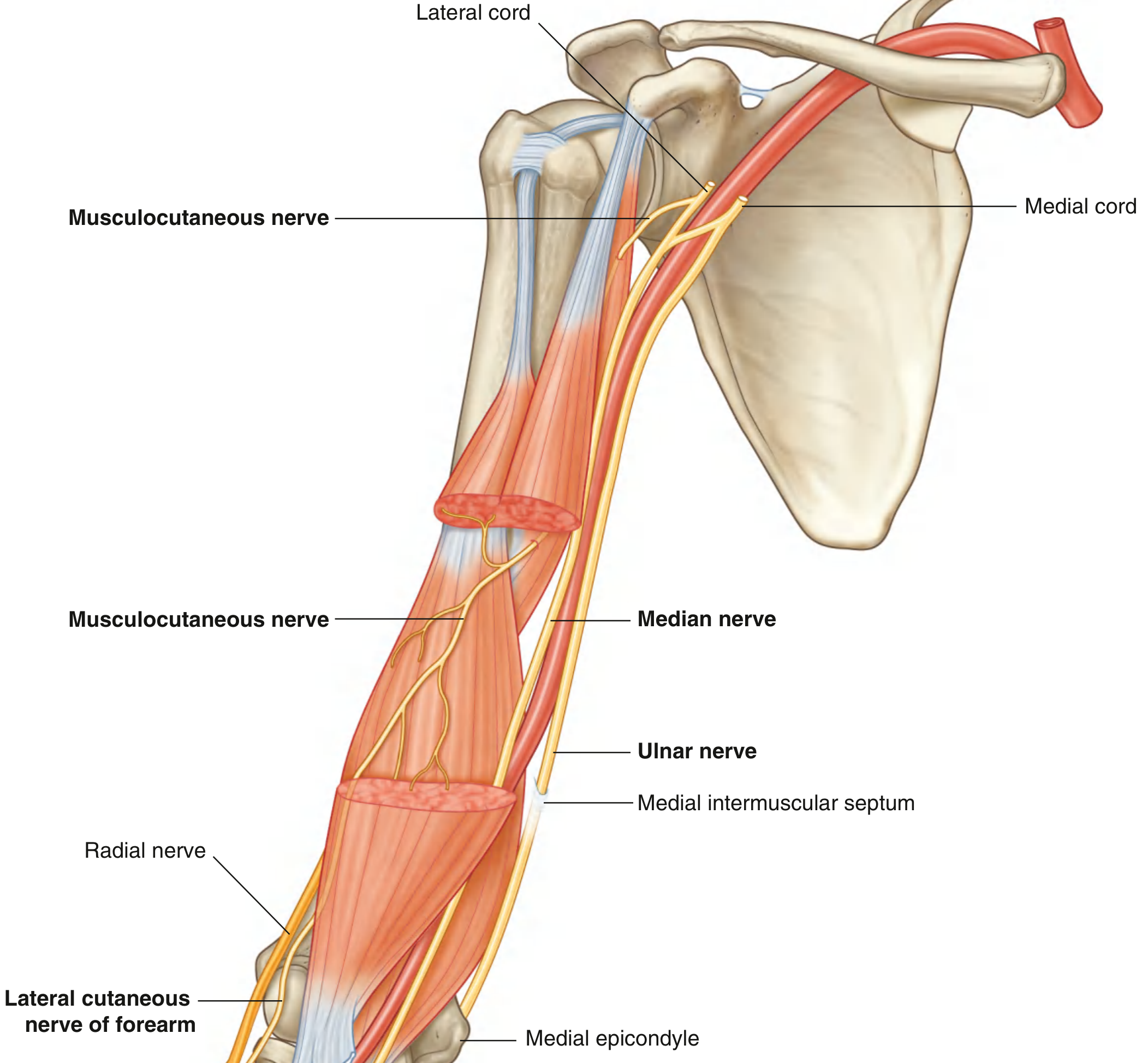
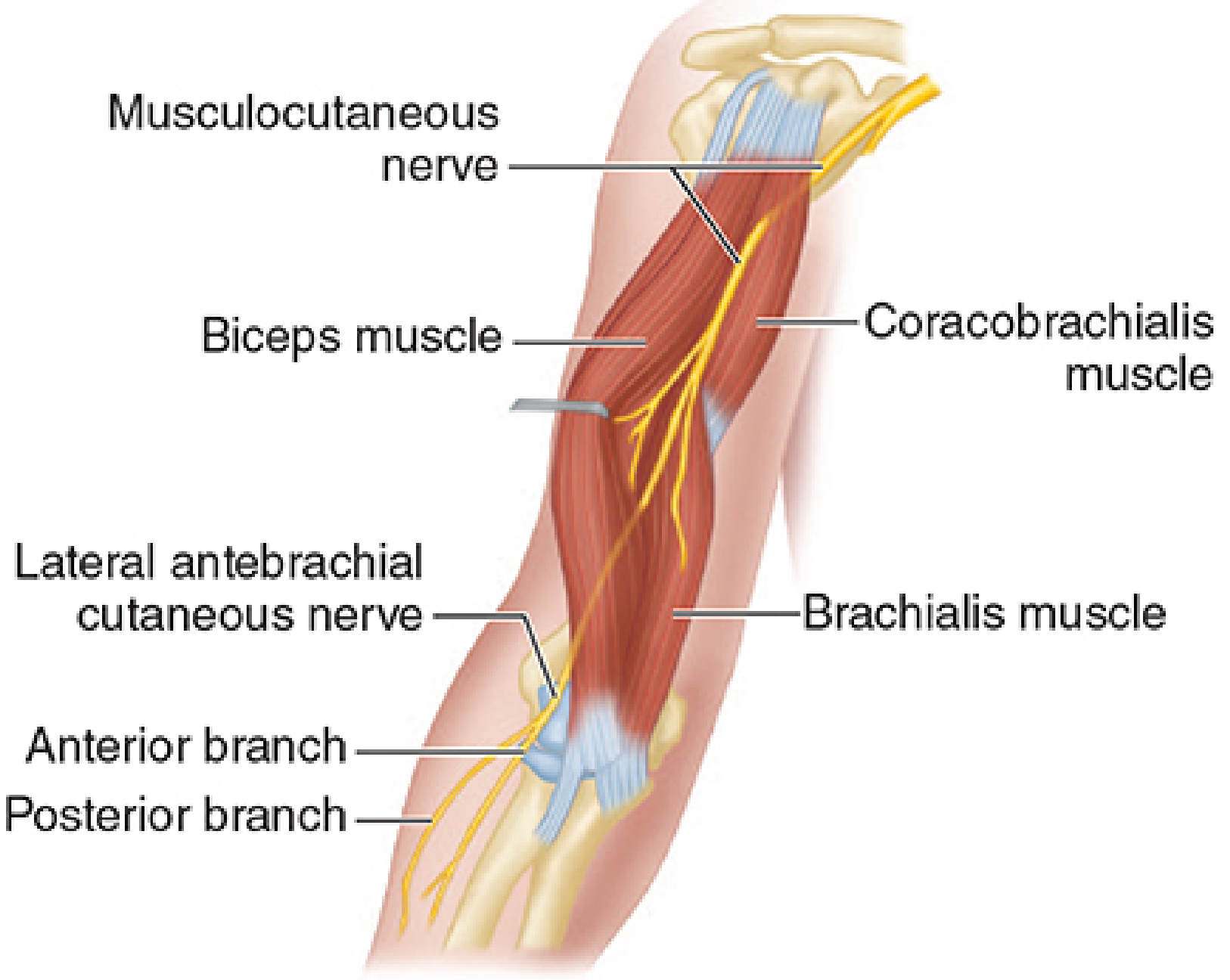
- Leaves the axilla and immediately pierces the coracobrachialis muscle at a mean distance of 5.6 cm inferior to the coracoid process (within 5 cm of the coracoid tip in 75% of cases).
- Passes diagonally down the arm in the fascial plane between the biceps brachii (anteriorly) and the brachialis (posteriorly), giving motor branches to each.
- At the elbow, it emerges laterally to the biceps tendon, penetrates the deep fascia, and continues as the lateral cutaneous nerve of the forearm (lateral antebrachial cutaneous nerve).
Branches and Innervation
Motor (all muscles of the anterior compartment of the arm)
| Muscle | Action |
|---|---|
| Coracobrachialis | Arm flexion and adduction at shoulder |
| Biceps brachii | Elbow flexion (especially with supination), forearm supination |
| Brachialis | Elbow flexion (main workhorse) |
Note: The branch to the coracobrachialis arises most proximally, at 3-7 cm distal to the coracoid tip.
Sensory
- Lateral cutaneous nerve of the forearm (terminal branch): supplies the lateral surface of the forearm, from the elbow to the wrist, via anterior and posterior divisions running in the subcutaneous tissue of the anterolateral and posterolateral forearm, respectively.
Clinical Relevance
Causes of Injury
| Cause | Mechanism |
|---|---|
| Shoulder dislocation | Stretch/tear |
| Proximal humeral fracture | Direct compression or displacement |
| General anesthesia / positioning | Compression during prolonged procedures |
| Strenuous exercise (weight lifting, rowing, throwing) | Entrapment/stretch at coracobrachialis |
| Carpet carrier's palsy | Repeated nerve compression by carrying rolled objects on the shoulder |
| Surgical retraction | Excessive medial retraction of the conjoined tendon during shoulder surgery |
| Neuralgic amyotrophy (Parsonage-Turner syndrome) | Inflammatory involvement |
| Venipuncture / IV cutdown in cubital fossa | Injures the lateral antebrachial cutaneous branch (lies under the median cubital vein) |
Clinical Features of Musculocutaneous Mononeuropathy
- Weakness of elbow flexion (especially with supination) and brachialis
- Atrophy of the ventral upper arm (biceps + brachialis wasting)
- Loss of biceps reflex (C5-C6)
- Sensory loss over the lateral forearm (autonomous zone: a narrow band along the radial forearm)
- Coracobrachialis weakness is present but hard to detect clinically
Electrodiagnostic Findings (NCS/EMG)
- NCS: Reduced or absent musculocutaneous CMAP amplitude (recorded over biceps); low-amplitude or absent lateral antebrachial cutaneous sensory nerve action potential
- EMG: Denervation in biceps brachii and brachialis; coracobrachialis is often spared (its branch arises proximal to where most injuries occur)
Differential Diagnosis
- C5 or C6 radiculopathy
- Upper trunk brachial plexopathy
- Lateral cord plexopathy
- Biceps tendon rupture (causes similar motor picture)
Prognosis and Treatment
- Spontaneous recovery is the rule for most injuries
- Local corticosteroid injection for pain relief
- Surgical decompression if no improvement over time
Surgical Importance
- The nerve is at risk during the deltopectoral approach (shoulder surgery) when the conjoined tendon (short head of biceps + coracobrachialis) is retracted medially - excessive medial retraction can stretch or avulse the nerve.
- The nerve is also endangered when extracting an anteriorly dislocated humeral head from beneath the conjoined tendon.
- In nerve transfer surgery, intercostal nerve transfers to the musculocutaneous nerve are used to restore elbow flexion after brachial plexus avulsion injuries.
Nerve Block (Anesthesia)
Blocking the musculocutaneous nerve is required to complete forearm and wrist anesthesia when performing an axillary brachial plexus block, because the nerve exits the plexus proximal to the axilla and is frequently missed by standard axillary injection. Under ultrasound guidance, the needle is redirected laterally to target the nerve lying between the heads of the coracobrachialis or between the coracobrachialis and biceps brachii, and 4-8 mL of local anesthetic is injected around the nerve.
Sources: Gray's Anatomy for Students, p. 879 | Bradley and Daroff's Neurology in Clinical Practice | Imaging Anatomy Vol. 3, p. 191 | Localization in Clinical Neurology, 8e, p. 90-91 | Morgan and Mikhail's Clinical Anesthesiology, 7e | Rockwood and Green's Fractures in Adults, 10th ed. | Campbell's Operative Orthopaedics, 15th ed.
Exam oriented answer and how to remember the course Make it more visualised and easily understandable
Loading Image
Loading Image
Here is a fully exam-oriented, memory-friendly breakdown:
🧠 Musculocutaneous Nerve - Exam Master Sheet
🔑 THE ONE-LINE MEMORY TRICK FOR THE COURSE
"Lateral cord → Pierces Cora → Rides between Bi & Bra → Pops out at elbow → Becomes LACN"
Think of it as a snake that:
- Hatches from the lateral cord
- Bites through coracobrachialis (pierces it)
- Slides between biceps and brachialis (sandwiched)
- Pops out laterally at elbow
- Becomes sensory - lateral antebrachial cutaneous nerve (LACN)
📍 STEP-BY-STEP COURSE (Visual Map)
LATERAL CORD (C5, C6, C7)
↓
[AXILLA] - Leaves axilla
↓
●PIERCES coracobrachialis ← (gives branch HERE)
↓
Between BICEPS (front) & BRACHIALIS (behind)
← gives branch to BICEPS
← gives branch to BRACHIALIS
↓
Emerges LATERAL to biceps tendon at elbow
↓
Pierces DEEP FASCIA
↓
= LATERAL ANTEBRACHIAL CUTANEOUS NERVE
├── Anterior branch → anterolateral forearm skin
└── Posterior branch → posterolateral forearm skin
⚡ QUICK FACTS TABLE (High-Yield)
| Feature | Value |
|---|---|
| Origin | Lateral cord of brachial plexus |
| Roots | C5, C6 (± C7) |
| Unique feature | Only nerve that pierces a muscle (coracobrachialis) |
| Runs between | Biceps brachii & brachialis |
| Terminal branch | Lateral antebrachial cutaneous nerve (LACN) |
| Sensory area | Lateral forearm (radial side, elbow to wrist) |
| Reflex tested | Biceps reflex (C5-C6) |
💪 MUSCLES INNERVATED
Mnemonic: "C - B - B" (CoracoBrachialis - Biceps - Brachialis)
Or remember: "Cord Boys Bicep Brachialis" from proximal to distal
| Muscle | Action | Exam clue |
|---|---|---|
| Coracobrachialis | Flexion + Adduction at shoulder | Hard to test clinically |
| Biceps brachii | Elbow flexion + Supination | Weak in supinated position |
| Brachialis | Elbow flexion (main flexor) | "True flexor" of elbow |
Exam pearl: The musculocutaneous nerve is the sole nerve of the anterior arm - it innervates ALL 3 muscles of the anterior compartment.
🩺 INJURY - WHAT TO EXPECT IN EXAM VIGNETTE
Scenario trigger: "Shoulder dislocation / weight lifter / carpet carrier / surgery with medial retraction"
Signs:
Motor loss:
✗ Weak elbow FLEXION (especially when forearm is SUPINATED)
✗ Weak SUPINATION (biceps role lost)
✗ Biceps + brachialis WASTING (ventral arm hollowing)
Reflex:
✗ BICEPS REFLEX LOST ← most testable sign
Sensory loss:
✗ Lateral forearm (radial side) from elbow → wrist
✓ Elbow flexion still POSSIBLE (brachioradialis, C6, radial nerve - compensates)
Key distinction (exam favorite):
| Feature | Musculocutaneous lesion | C5-C6 radiculopathy |
|---|---|---|
| Biceps weakness | ✓ | ✓ |
| Deltoid weakness | ✗ | ✓ (axillary n.) |
| Supraspinatus/infraspinatus weakness | ✗ | ✓ |
| Sensory loss | Lateral forearm only | Lateral arm + forearm |
| EMG | Biceps + brachialis only | Multiple muscles |
🔍 NCS/EMG FINDINGS (for PG/specialty exams)
| Test | Finding |
|---|---|
| Motor NCS (biceps) | Reduced CMAP amplitude |
| Sensory NCS (LACN) | Low/absent SNAP |
| EMG | Denervation in biceps + brachialis |
| EMG coracobrachialis | Often SPARED (branch arises most proximally) |
Exam pearl: Coracobrachialis sparing on EMG means the injury is distal to its branch - most common scenario.
⚠️ CAUSES TO MEMORIZE (Common Exam Scenarios)
| Cause | Why it happens |
|---|---|
| Shoulder dislocation | Stretch of nerve |
| Proximal humerus fracture | Direct injury |
| Weight lifting / rowing | Entrapment in coracobrachialis |
| Carpet carrier's palsy | Repeated compression on shoulder |
| Axillary brachial plexus block | Nerve exits proximal → often missed → must block separately |
| Surgical medial retraction | Deltopectoral approach risk |
| Venipuncture at cubital fossa | Injures LACN (lies under median cubital vein) |
🎯 UNIQUE / FAVOURITE EXAM FACTS
- Only nerve in the brachial plexus that pierces a muscle (coracobrachialis) - MCQ magnet
- Terminal branch is PURELY sensory (LACN) - despite starting as mixed
- Missed in axillary block - exits plexus proximal to axilla, needs separate injection
- LACN lies directly under median cubital vein - injured by cubital fossa venipuncture → pure sensory loss
- Spontaneous recovery is the rule - even after complete injury
🧩 SUMMARY FLOWCHART FOR REVISION
LATERAL CORD
↓ C5, C6 (±C7)
MUSCULOCUTANEOUS NERVE
/ | \
Coracobrachialis Biceps Brachialis
(shoulder flex) (flex+sup) (flex)
↓
At elbow → pierces fascia
↓
LATERAL ANTEBRACHIAL CUTANEOUS NERVE
↙ ↘
Anterior branch Posterior branch
(anterolateral (posterolateral
forearm skin) forearm skin)
Memory hook to lock it in: Think of the musculocutaneous nerve as "the arm's own personal trainer" - it goes through the coracobrachialis, coaches biceps and brachialis to flex and supinate, then retires as a sensory nerve covering the lateral forearm. One nerve, one compartment, one job: flex and feel the lateral forearm.
This is a shared conversation. Sign in to Orris to start your own chat.