Tuberculosis, clinical features, etiopathology, mode of transmission, types, lab diagnosis, systemic or local effects, treatment, MDR TB, xdr TB, prophylaxis, prevention
Tuberculosis - Comprehensive Review
1. Etiology and Organism
- Slow-growing (generation time ~15-20 hours); grows on Lowenstein-Jensen (LJ) medium in 3-6 weeks
- Cell wall contains cord factor (trehalose dimycolate) - inhibits phagosome-lysosome fusion, key virulence factor
- Sulfolipids in the cell envelope promote coughing - enhancing transmission
- Related pathogens: M. bovis (cattle, rare), M. africanum, and M. microti comprise the M. tuberculosis complex (MTBC)
2. Epidemiology
| Indicator | India (2019) |
|---|---|
| Estimated incidence | 2.64 million (193 per 100,000) |
| HIV-TB co-infection | 71,000 |
| MDR/RR-TB incidence | 124,000 |
| Mortality (HIV-negative TB) | 436,000 |
- Park's Textbook of Preventive and Social Medicine
3. Mode of Transmission
- 60-71% of aerosolized MTB survive for 3 hours indoors; 28-32% for 9 hours under standard conditions
- Close (household) contacts: ~50% become infected; ~15 per 1,000 develop active TB
- Non-close contacts: ~15% infected; ~3 per 1,000 develop active TB
- Patients with cavitary lesions (10^7-10^9 bacilli per cavity) are the most infectious; smear-negative patients can still transmit
- Environmental factors promoting transmission: poor ventilation, recirculating air systems, overcrowding, darkness (UV light kills bacilli)
- UV light irradiation is used in hospital waiting rooms and clinics to reduce transmission
- Murray & Nadel's Textbook of Respiratory Medicine; Goldman-Cecil Medicine
4. Etiopathogenesis
Step 1: Initial Infection and Innate Response
- Blocking phagosome-lysosome fusion (cord factor, lipoarabinomannan)
- Inhibiting autophagy
- Inducing the Warburg effect
- Activating ESX-1 secretion system to escape the phagosome
Step 2: Adaptive Immunity and Granuloma Formation
- Dendritic cells carry antigen to regional lymph nodes and present to T cells
- CD4+ T cells (Th1) produce IFN-γ, activating macrophages to kill intracellular bacilli
- CD8+ T cells have cytotoxic activity
- IL-12 from macrophages drives Th1 differentiation - patients with IL-12 receptor deficiency have severe mycobacterial infections
- A granuloma forms: a structured collection of activated macrophages (epithelioid cells), Langhans giant cells, lymphocytes, and fibroblasts walling off the bacilli
- Central caseous necrosis (cheese-like, acidic, hypoxic, nutrient-poor) develops, creating a hostile environment that limits bacterial replication but does not eliminate all bacilli
Step 3: Primary TB Complex (Ghon Complex)
- The initial lung parenchymal lesion = Ghon focus (subpleural, typically mid-lung zone)
- Ghon focus + caseating hilar/regional lymph nodes = Ghon (Primary) Complex
- In ~95% of immunocompetent individuals: granulomas calcify, infection is controlled, bacilli remain dormant (latent TB)
- In <5%: primary disease progresses without control
Step 4: Latent TB Infection (LTBI)
- ~1.7 billion people worldwide have LTBI
- Bacilli remain dormant within granulomas, held in check by immune surveillance
- Lifetime risk of reactivation: ~5-10% (without HIV); ~10% per year (with HIV)
- Reactivation triggers: HIV infection, immunosuppressive drugs (TNF-alpha inhibitors, corticosteroids), diabetes mellitus, malnutrition, silicosis, end-stage renal disease, head/neck cancer, lymphoma, advanced age, gastrectomy
Step 5: Post-Primary (Secondary/Reactivation) TB
-
Bacilli reactivate, typically in the apices of upper lobes (high O₂ tension favors aerobic MTB growth)
-
Rapid tissue destruction due to Type IV (delayed-type) hypersensitivity - the sensitized immune system mounts a vigorous but tissue-destructive response
-
Cavitation occurs readily; cavities may erode into airways, releasing infectious bacilli into sputum
-
Robbins, Cotran & Kumar Pathologic Basis of Disease; Goldman-Cecil Medicine; Murray & Nadel's
5. Types / Classification of Tuberculosis
A. By Site
- Involves the lung parenchyma
- Miliary TB is classified as PTB (lesions present in lungs)
- Most common form; source of community transmission
- Lymph nodes (most common EPTB site globally): cervical lymphadenopathy ("scrofula"), non-tender, matted
- Pleura: Pleural effusion (exudative, lymphocyte-predominant, high ADA)
- CNS: Tuberculous meningitis (TBM), tuberculoma - mortality 18-40%
- Spine (Pott's disease): Vertebral body destruction, paravertebral abscess, gibbus deformity, cord compression
- Genitourinary: "Sterile pyuria," ureteric strictures, renal calcification ("putty kidney")
- Peritoneum: Ascites, abdominal pain, peritoneal thickening
- Pericardium: Constrictive pericarditis
- Miliary TB: Hematogenous dissemination producing 1-2 mm millet-seed-like granulomas in multiple organs; can affect lungs, liver, spleen, bone marrow, meninges
B. By Treatment History (WHO Classification)
- New: Never treated or treated <1 month
- Relapse: Previously cured/completed, now recurrent
- Treatment after failure: Treatment failed at end of last course
- Treatment after loss to follow-up: (previously "treatment after default")
- Other previously treated: Unknown/undocumented outcome
C. By Drug Resistance
-
Monoresistance: Resistance to one first-line drug
-
Polydrug resistance: Resistance to >1 first-line drug (but not both INH and RIF)
-
MDR-TB: Resistance to at least isoniazid (INH) and rifampicin (RIF)
-
XDR-TB (new 2021 WHO definition): MDR/RR-TB + resistance to any fluoroquinolone AND at least one of bedaquiline or linezolid
-
Pre-XDR-TB: MDR/RR-TB + resistance to a fluoroquinolone
-
RR-TB: Rifampicin-resistant TB (any resistance to rifampicin)
-
Park's Textbook of Preventive and Social Medicine; Murray & Nadel's Respiratory Medicine
6. Clinical Features
Primary TB
- Usually asymptomatic or subclinical
- May present with: low-grade fever, malaise, nonproductive cough, shortness of breath
- Rare: erythema nodosum (immune-mediated), phlyctenular conjunctivitis
- CXR: mid-lung field patchy opacity (Ghon focus) + hilar lymphadenopathy
Post-Primary (Secondary/Reactivation) TB
- Low-grade fever (typically remittent, highest in the afternoon)
- Night sweats
- Anorexia and significant weight loss (cachexia)
- Fatigue, malaise
- Chronic productive cough (>2-3 weeks) - initially mucoid, then mucopurulent
- Hemoptysis - present in ~50% of pulmonary TB cases; ranges from blood-streaked sputum to massive hemorrhage (Rasmussen aneurysm erosion)
- Dyspnea (with extensive disease, pneumothorax, pleural effusion)
- Pleuritic chest pain (when infection extends to pleural surfaces)
- Rales/crepitations over the apices
Miliary TB
- Fever, weight loss, hepatosplenomegaly
- Diffuse miliary nodules on CXR (1-2 mm "millet seed" pattern)
- Can present with meningism if CNS involved
- May be missed early due to non-specific presentation; bone marrow biopsy may confirm
7. Systemic / Local Effects (Complications)
Pulmonary Complications
- Cavitation → secondary bacterial infection, aspergilloma (fungus ball in old cavity)
- Bronchiectasis
- Pneumothorax (from pleural disease or bronchopleural fistula)
- Massive hemoptysis
- Respiratory failure (extensive bilateral disease)
- Destroyed lung / fibrosis
Extrapulmonary Complications
| System | Complication |
|---|---|
| CNS | TBM (mortality 18-40%), hydrocephalus, tuberculoma, paraparesis |
| Spine | Pott's disease, gibbus deformity, paraplegia |
| Kidney | Renal TB, strictures, hydronephrosis, "putty kidney" |
| Adrenal | Addison's disease (bilateral adrenal destruction) |
| Pericardium | Constrictive pericarditis |
| Joints | TB arthritis, cold abscess |
| Bone marrow | Pancytopenia (miliary TB) |
| GI | Ileocaecal TB (commonest abdominal site), bowel obstruction, malabsorption |
Immune-mediated Effects
- Erythema nodosum
- Phlyctenular keratoconjunctivitis
- Reactive arthritis (Poncet's disease)
8. Laboratory Diagnosis
Bacteriological Tests (Gold Standard)
- ZN staining (standard) or Fluorescent staining (auramine-rhodamine, more sensitive)
- At least 2-3 sputum samples collected (early morning specimens preferred)
- Sensitivity ~40-60%; Specificity ~99% (smear cannot distinguish MTB from NTM)
- A positive smear means the patient is highly infectious (smear-positive TB)
- Solid media: Lowenstein-Jensen (LJ) medium - growth in 3-6 weeks
- Liquid media (automated): BACTEC MGIT 960, BacT/Alert, VersaTrek - results in 1-2 weeks
- Allows drug susceptibility testing (DST)
- Modified proportionate sensitivity testing (MGIT 960 system)
- Economic variant proportion method (1%) on LJ medium
- Essential for diagnosing drug resistance
- GeneXpert MTB/RIF (CBNAAT): PCR-based; simultaneously detects MTB AND rifampicin resistance; results in <2 hours; WHO-recommended first-line test; sensitivity ~89% overall, ~98% in smear-positive
- Truenat MTB: Point-of-care molecular test
- Line Probe Assay (LPA):
- First-line LPA (FL-LPA): Detects MTB complex + INH and RIF resistance (rpoB, katG, inhA mutations)
- Second-line LPA (SL-LPA): Detects fluoroquinolone and second-line injectable resistance
- Whole-genome sequencing (WGS): Predicts susceptibility to first-line drugs with >90% accuracy; not yet widely available
Immunological Tests
- Intradermal injection of 0.1 mL (2 TU) PPD (purified protein derivative) into the forearm
- Read at 48-72 hours; measure induration (not erythema) in mm
- Interpretation (induration thresholds):
- ≥5 mm: HIV positive, recent TB contact, immunosuppressed, old fibrotic lesion on CXR
- ≥10 mm: High-risk groups (healthcare workers, immigrants from endemic areas, prisoners, diabetics, silicosis, renal failure, children <5 years)
- ≥15 mm: General population with no risk factors
- False negatives: Active severe TB, HIV/immunosuppression, malnutrition, viral infections (measles, chickenpox), recent live-virus vaccination, incorrect injection, very old infection (waning immunity)
- False positives: BCG vaccination, NTM infection
- Two-step testing: Used for periodic retesting (e.g., healthcare workers) to detect boosting phenomenon
- Does NOT differentiate latent from active TB
- Blood tests: T-cells are stimulated with MTB-specific antigens (ESAT-6, CFP-10 - absent in BCG strains)
- Two commercial assays: QuantiFERON-TB Gold Plus (whole blood ELISA) and T-SPOT.TB (ELISPOT)
- Advantages over TST: Not affected by BCG vaccination, requires only one visit, more specific
- Also cannot differentiate active from latent TB; similar sensitivity to TST
- Preferred in BCG-vaccinated populations and healthcare workers
Radiological Diagnosis
- Primary TB: Mid-lung opacity + hilar lymphadenopathy (Ghon complex)
- Post-primary TB: Upper lobe infiltrates, cavitation, fibrosis, calcification, pleural effusion
- Miliary TB: Diffuse bilateral 1-2 mm nodules throughout both lung fields
- More sensitive than CXR; detects small cavities, tree-in-bud pattern (bronchogenic spread), miliary nodules
- MRI: Better for pleural involvement and characterizing caseous necrosis; preferred in pregnant women and children (no radiation)
- FDG-PET/CT: Useful for monitoring treatment response and differentiating active from inactive disease
Other Diagnostic Tests
-
ADA (Adenosine Deaminase): Elevated in pleural, pericardial, peritoneal, and CSF TB
-
Histopathology: Caseating granuloma with Langhans giant cells on biopsy (lymph node, pleura, bone)
-
CSF analysis (TBM): Lymphocytic pleocytosis, elevated protein, low glucose, low chloride; India ink (exclude cryptococcal meningitis)
-
Nucleic Acid Amplification Tests (NAAT): As sensitive as culture in smear-positive samples; less sensitive in smear-negative or pediatric TB
-
Murray & Nadel's Respiratory Medicine; Park's Preventive Medicine; Robbins & Cotran Pathology; Sherris & Ryan's Medical Microbiology
9. Treatment of TB
Principles of Anti-TB Therapy
- Kill rapidly dividing bacilli (bactericidal activity - early)
- Kill persisting bacilli in acidic/hypoxic environments (sterilizing activity)
- Prevent emergence of drug resistance
- Intensive phase: 3-4 drugs for 2 months - rapid kill, reducing bacterial load
- Continuation phase: 2 drugs for 4 months - sterilize residual "persisters," prevent relapse
First-Line Anti-TB Drugs (HRZE)
| Drug | Mechanism | Key Side Effects |
|---|---|---|
| Isoniazid (H/INH) | Inhibits mycolic acid synthesis (InhA) | Hepatotoxicity, peripheral neuropathy (B6 deficiency), lupus-like reaction |
| Rifampicin (R/RIF) | Inhibits RNA polymerase (rpoB) | Hepatotoxicity, orange discoloration of body fluids, drug interactions (CYP450 inducer), flu-like syndrome |
| Pyrazinamide (Z/PZA) | Active in acidic pH; mechanism uncertain | Hepatotoxicity (most hepatotoxic), hyperuricemia, arthralgia |
| Ethambutol (E/EMB) | Inhibits arabinosyl transferase (arabinogalactan synthesis) | Optic neuritis (color vision loss, reduced visual acuity) |
| Streptomycin (S) | Aminoglycoside; inhibits 30S ribosome | Ototoxicity (vestibular and cochlear), nephrotoxicity |
Standard Treatment Regimens
- 2HRZE / 4HR (2 months intensive phase HRZE + 4 months continuation phase HR)
- Daily regimen is preferred; intermittent (thrice-weekly) also used under DOTS supervision
- Drug susceptibility testing (DST) before starting treatment
- 2HRZES / 1HRZE / 5HRE (older regimen) OR individualized based on DST
- TB meningitis: 2HRZE / 7-10HR (total 9-12 months) + adjuvant dexamethasone
- Adults: dexamethasone 0.4 mg/kg/24hr with reducing course over 6 weeks
- Children: prednisolone 4 mg/kg/24hr for 4 weeks, then taper
- Bone/joint TB: 2HRZE / 4-7HR (6-9 months total)
- Spinal TB (Pott's disease): Medical management preferred; surgery for cord compression, poor response to treatment
-
3HP: 3 months of weekly isoniazid + rifapentine (preferred regimen; 12 doses)
-
1HP: 1 month of daily isoniazid + rifapentine
-
3HR: 3 months of daily isoniazid + rifampicin
-
4R: 4 months of daily rifampicin
-
6H: 6 months of daily isoniazid (alternative)
-
9H: 9 months of daily isoniazid (conditionally recommended)
-
Isoniazid 5 mg/kg/day (adults), 10-20 mg/kg/day (children), max 300 mg/day
-
Murray & Nadel's Respiratory Medicine; Park's Preventive Medicine
10. MDR-TB (Multidrug-Resistant Tuberculosis)
- ~3.3% of newly diagnosed patients worldwide
- ~20% of previously treated patients
- India: ~2.8% new cases, ~14% previously treated cases
- Inadequate/irregular treatment (poor adherence)
- Incorrect prescription (wrong drugs, doses, or duration)
- Poor drug quality or supply
- Incomplete treatment courses (patient defaulting)
- Drug malabsorption
- Transmission of already-resistant strains
WHO Grouping for MDR-TB Treatment (Longer Regimen)
| Group | Medicines |
|---|---|
| Group A (include all 3) | Levofloxacin (Lfx) OR Moxifloxacin (Mfx) + Bedaquiline (Bdq) + Linezolid (Lzd) |
| Group B (add 1 or both) | Clofazimine (Cfz) + Cycloserine (Cs) OR Terizidone (Trd) |
| Group C (complete when A+B insufficient) | Ethambutol (E), Delamanid (Dlm), Pyrazinamide (Z), Imipenem-cilastatin OR Meropenem, Amikacin (Am), Ethionamide (Eto), p-aminosalicylic acid (PAS) |
- Park's Preventive Medicine; Murray & Nadel's; Schwartz's Surgery
11. XDR-TB (Extensively Drug-Resistant Tuberculosis)
- Rifampicin (part of MDR/RR-TB definition) AND
- Any fluoroquinolone (levofloxacin, moxifloxacin) AND
- At least one of bedaquiline or linezolid
- Remaining susceptible second and third-line agents
- Newer drugs: bedaquiline, linezolid, delamanid, pretomanid
- BPaL/BPaLC regimen: Bedaquiline + Pretomanid + Linezolid ± Clofazimine (TB-PRACTECAL, ZeNix trials)
- Surgery in selected cases (resection of localized disease)
- Complete, adequate, and regular treatment is the most important preventive measure
- DOTS (Directly Observed Treatment, Short-course) - a key WHO strategy
- Rapid DST to guide treatment
- Infection control measures in health facilities
12. Prophylaxis
A. Chemoprophylaxis (Preventive Therapy for LTBI)
- HIV-positive individuals (regardless of TST/IGRA result in high-burden countries)
- Household contacts of sputum-positive TB (especially children <5 years, immunocompromised)
- Healthcare workers with LTBI
- Patients on anti-TNF therapy
- Patients with fibrotic lesions consistent with old TB (TST/IGRA positive)
B. BCG Vaccination (Primary Prevention)
- Vaccine: BCG (Bacille Calmette-Guérin) - live attenuated strain of M. bovis developed by Calmette and Guérin (1921)
- Efficacy: 70-80% protection against severe forms of childhood TB: tuberculous meningitis, miliary TB. Protection against pulmonary TB in adults is variable (0-80% in different trials)
- Dose: 0.1 mg in 0.1 mL (standard); newborns <4 weeks: 0.05 mL (thinner skin, risk of abscess with full dose)
- Route: Intradermal, into the deltoid (left arm, just above deltoid insertion); using tuberculin syringe with 26-gauge needle; produces a 5 mm wheal if correctly administered
- Age (India policy): At birth (institutional deliveries) or 6 weeks of age (simultaneously with DPT and polio)
- Site: Left deltoid (if injected too high/forward/backward, regional lymph nodes may become involved)
- 2-3 weeks: papule develops
- ~5 weeks: papule reaches 4-8 mm, then may ulcerate (shallow, usually crusted)
- 6-12 weeks: heals, leaves permanent scar (4-8 mm round scar = evidence of successful vaccination)
- 8-14 weeks: Mantoux test becomes positive
- Local ulceration and lymphadenitis: 1-10% of vaccinations
- Disseminated BCG infection: <1 per million vaccinations (associated with severe cellular immunodeficiency, e.g., SCID)
- Osteomyelitis (rare)
- Park's Preventive Medicine
13. Prevention and Control (RNTCP/NTP Strategies)
DOTS (Directly Observed Treatment, Short-Course)
- Government commitment to sustained TB control
- Case detection by bacteriological examination (sputum microscopy)
- Standardized short-course chemotherapy under direct observation
- Regular, uninterrupted supply of all essential anti-TB drugs
- Recording and reporting system for monitoring and evaluation
End TB Strategy (WHO)
- Integrated, patient-centered care and prevention
- Bold policies and supportive systems
- Intensified research and innovation
Key Prevention Measures
- BCG vaccination (primary prevention - especially for children)
- Early case detection and prompt treatment (breaking transmission chain)
- Contact tracing and LTBI treatment (especially household contacts)
- Infection control in healthcare facilities: N95 respirators, negative-pressure rooms, UV irradiation of room air, HEPA filtration, adequate ventilation
- Addressing risk factors: Control of HIV (antiretrovirals reduce TB risk), diabetes management, improved nutrition, reduced overcrowding and poverty
- Active screening of vulnerable groups: prisoners, homeless, healthcare workers, immunocompromised, TB contacts
- Notification: TB is a notifiable disease; mandatory reporting under national programs
- Prevention of drug resistance: Ensuring treatment completion, use of fixed-dose combinations (FDCs), DST-guided therapy
Notification and Recording
- All TB cases must be notified to the National Tuberculosis Elimination Programme (NTEP, formerly RNTCP) in India
- Treatment outcomes recorded: Cured, Treatment completed, Treatment failed, Died, Lost to follow-up, Not evaluated
Summary Table
| Feature | Detail |
|---|---|
| Causative agent | M. tuberculosis (acid-fast bacillus) |
| Transmission | Airborne droplet nuclei (1-5 µm) |
| Primary lesion | Ghon focus (subpleural mid-lung) |
| Hallmark pathology | Caseating granuloma with Langhans giant cells |
| Most common symptom | Chronic productive cough >2-3 weeks |
| Classic systemic features | Fever, night sweats, weight loss |
| Best screening test | TST (Mantoux) or IGRA |
| Fastest molecular test | GeneXpert MTB/RIF (results <2 hours) |
| Gold standard culture | LJ medium (3-6 weeks) or liquid MGIT (1-2 weeks) |
| Standard DS-TB treatment | 2HRZE / 4HR (6 months total) |
| MDR-TB definition | Resistance to INH + RIF |
| XDR-TB definition (2021) | MDR + fluoroquinolone + bedaquiline or linezolid resistance |
| MDR-TB treatment duration | 18-24 months (longer regimen) |
| Vaccine | BCG (live attenuated M. bovis) |
| BCG dose | 0.1 mg/0.1 mL intradermal; neonates 0.05 mL |
| BCG efficacy | 70-80% against severe childhood TB (TBM, miliary) |
Search for recent WHO guidelines on TB diagnosis and drug-resistant TB management
WHO guidelines tuberculosis diagnosis drug-resistant TB management 2024 2025
"tuberculosis" AND "WHO guidelines" AND ("drug-resistant" OR "diagnosis")
WHO 2024 2025 consolidated guidelines drug-resistant tuberculosis treatment update
https://www.who.int/news/item/11-08-2025-who-releases-an-upd…
"tuberculosis" AND ("BPaL" OR "bedaquiline pretomanid linezolid" OR "6-month regimen" OR "MDR-TB treatment")
PMID: 39813501
PMID: 40683298
PMID: 41128098
WHO Module 3 diagnosis TB 2025 updated IGRA rapid molecular tests tNGS recommendations
https://www.who.int/teams/global-programme-on-tuberculosis-a…
PMID: 40915311
Recent WHO Guidelines on TB Diagnosis and Drug-Resistant TB Management (2024-2026)
WHO Consolidated Guidelines - Module Structure (Updated 2025)
| Module | Topic | Latest Update |
|---|---|---|
| Module 1 | Prevention (TB preventive treatment) | 2024 (2nd edition) |
| Module 2 | Screening | 2021 |
| Module 3 | Diagnosis | 2025 |
| Module 4 | Treatment and care | 2025 |
| Module 5 | Children and adolescents | 2022 |
| Module 6 | Comorbidities (HIV, undernutrition) | October 2025 |
PART 1: Updated WHO Guidance on TB Diagnosis (Module 3, August 2025)
1. Rapid Molecular Tests - Now the First-Line Standard
- A 2023 UN High-Level Meeting target requires that 100% of people diagnosed with TB should initially be tested with a WHO-recommended rapid diagnostic test by 2027
- 2024 WHO benchmarks: 12 standards defined for universal access to rapid TB diagnostics
- Low-complexity automated NAATs (e.g., GeneXpert MTB/RIF Ultra, Cobas MTB)
- Manual NAATs (e.g., Truenat MTB, MTB Plus)
- Biomarker-based point-of-care tests (e.g., LF-LAM for HIV-positive patients)
2. Xpert MTB/RIF Ultra - Updated Evidence (Cochrane 2025)
| Sample Type | Sensitivity (children, MRS) | Specificity |
|---|---|---|
| Sputum | 75.3% (95% CI 68.9-80.8%) | 95.9% |
| Gastric aspirate | 69.6% (95% CI 60.3-77.6%) | 91.0% |
| Stool | 68.0% (95% CI 50.3-81.7%) | 98.2% |
3. New Near-Point-of-Care Tests (March 2026)
- Portable battery-powered molecular tests delivering results in <1 hour, at less than half the cost of existing molecular diagnostics
- Recommended for tongue swab samples - a new, easy-to-collect sample type for adults and adolescents who cannot produce sputum (previously untestable population)
- Sputum pooling strategy - combining samples from multiple individuals reduces commodity costs and machine time (recommended when resources are exceptionally constrained)
- These devices have potential future use for HIV, mpox, and HPV testing
4. Targeted Next-Generation Sequencing (tNGS)
- Updated tNGS solutions for detection of drug-resistant TB (resistance to more drug classes than GeneXpert)
- Revised pooled diagnostic accuracy estimates for NAATs
- New figure guiding use of DST results for treatment regimen selection
5. New and Updated IGRAs
- New policy statements on use of newer-generation IGRA platforms for detection of TB infection
- Updated diagnostic algorithms for:
- Adults and adolescents with HIV (concurrent respiratory + non-respiratory sample testing)
- Children with HIV
- Children without HIV or with unknown HIV status
6. Isoniazid-Resistant TB - New Emphasis
- WHO 2025 data: Isoniazid-resistant, rifampicin-susceptible TB is now the most prevalent form of drug resistance globally (aside from streptomycin resistance)
- ~7% of newly diagnosed cases
- ~8-11% of previously treated cases
- INH-resistant TB carries a higher risk of acquiring further resistance and evolving toward MDR-TB if treated with standard 2HRZE/4HR
- Dedicated guidance for this category: add levofloxacin to cover INH resistance
PART 2: Updated WHO Guidance on Drug-Resistant TB Treatment (Module 4, 2025)
Key Paradigm Shift: All-Oral Shorter Regimens
A. 6-Month BPaLM Regimen - New Standard for MDR/RR-TB
| Outcome | Result (NNT) |
|---|---|
| Unfavorable composite outcome (death/failure/loss/recurrence) | NNT = 7 (BPaLM better) |
| Early treatment discontinuation | NNT = 8 |
| Serious adverse events | NNT = 5 |
B. Pre-XDR-TB: New Trial Evidence - endTB-Q (Lancet Respir Med, September 2025)
- 6-month BDLC for limited disease, 9-month BDLC for extensive disease
- Favourable outcome at week 73: 87% (BDLC) vs. 89% (control) in mITT population
- Adjusted risk difference: +0.2% (95% CI -9.1 to +9.5; p-noninferiority = 0.0051) - non-inferiority demonstrated in mITT
- Per-protocol analysis did not show non-inferiority (borderline result)
- This trial provides important evidence supporting all-oral regimens even for fluoroquinolone-resistant TB
C. Bedaquiline + Linezolid - Meta-Analysis
D. STREAM Stage 2 - Long-Term Data (Lancet Respir Med, December 2024)
E. Indian RCT on BPaL Linezolid Dosing (Clin Infect Dis, December 2024)
F. QTc Monitoring - TB-PRACTECAL Data
PART 3: DS-TB - Shorter Regimen Research (Clo-Fast Trial, Lancet Infect Dis, January 2026)
- The trial was stopped early for lack of clinical efficacy - the 3-month clofazimine-containing regimen did not meet non-inferiority criteria
- Important negative result: this particular shortening strategy did not work
- However, ATS/CDC/ERS/IDSA 2025 updates conditionally recommend 4-month regimens (rifapentine + moxifloxacin-based) for selected DS-TB patients ≥12 years old
PART 4: TB and Undernutrition (WHO Module 6, October 2025)
- Nutritional assessment and counselling for ALL people with TB and household contacts - now a core TB strategy
- Addressing food insecurity is integrated into people-centered care under the End TB Strategy
- Undernutrition is one of the most significant drivers of the TB epidemic globally
Summary of What Changed vs. Prior Guidelines
| Aspect | Old Guidance | Updated WHO 2025 Guidance |
|---|---|---|
| First-line diagnostic test | Sputum smear microscopy | Rapid molecular test (WRD) - strongly preferred |
| New sample types | Sputum only | + Tongue swabs, sputum pooling now recommended |
| Children's diagnosis | Limited tools | Updated Xpert Ultra accuracy data; multi-sample approaches |
| IGRA | QuantiFERON, T-SPOT | Updated with newer-generation IGRA platforms |
| Drug resistance testing | LPA + phenotypic DST | tNGS added for broader resistance detection |
| MDR/RR-TB treatment | 18-24 months, injectable-containing | 6-month BPaLM (all-oral) - preferred first choice |
| Pre-XDR-TB treatment | Very limited options | BDLC (6-9 months) supported by endTB-Q trial |
| INH-resistant TB | Often under-addressed | Explicit emphasis; add levofloxacin |
| Nutrition | Not formally addressed | Nutritional assessment now mandatory for all TB patients |
| Monitoring DR-TB adverse events | Variable | Active, systematic monitoring in most countries by 2024 |
- WHO Global TB Report 2025 - Section 2.2 Diagnostic Testing (data as of July 30, 2025)
- WHO Operational Handbook Module 3: Diagnosis, updated August 2025
- WHO new near-POC diagnostic tools, March 24, 2026
- BPaLM systematic review: Silva et al., J Bras Pneumol 2025 (PMID 39813501)
- endTB-Q pre-XDR trial: Guglielmetti et al., Lancet Respir Med 2025 (PMID 40683298)
- Xpert Ultra in children (Cochrane 2025): Kay et al., Cochrane Database 2025 (PMID 41128098)
- WHO Module 6 - TB and undernutrition, October 2025
Hiv aids
WHO HIV clinical staging 2024 CD4 count criteria AIDS defining conditions
HIV / AIDS - Comprehensive Review
1. Introduction and Epidemiology
-
~39 million people living with HIV worldwide (2022)
-
~630,000 deaths annually
-
~67% of all cases in Sub-Saharan Africa
-
ART transformed HIV from a fatal disease to a manageable chronic illness (after 1995-96 in high-income countries)
-
UNAIDS 95-95-95 targets (by 2030): 95% know status, 95% on ART, 95% virally suppressed - already achieved by 5 countries (Botswana, Eswatini, Rwanda, Tanzania, Zimbabwe)
-
First-line ART now costs <$45/year in low- and middle-income countries (vs. >$10,000/year in 2000)
-
Harrison's Principles of Internal Medicine 22E (2025); Robbins & Kumar Basic Pathology
2. The Virus - Virology
- HIV-1: Responsible for the global pandemic; more virulent
- HIV-2: Predominantly West Africa; less transmissible, slower progression; NNRTIs, enfuvirtide, and fostemsavir are NOT active against HIV-2
- Enveloped RNA virus; genome is single-stranded positive-sense RNA (two copies)
- Outer envelope: gp120 (surface glycoprotein, binds CD4) + gp41 (transmembrane; mediates fusion)
- Capsid protein: p24 (marker of acute infection)
- Matrix protein: p17
- Enzymes within the virion: Reverse transcriptase (RNA → DNA), Integrase (integrates viral DNA into host genome), Protease (cleaves polyproteins into functional proteins)
- Structural: gag (core proteins), pol (enzymes), env (envelope proteins)
- Regulatory: tat (transactivator - key for viral replication), rev (RNA export), nef, vif, vpr, vpu
- T-tropic (X4) strains: Infect CD4+ T cells using CXCR4 as co-receptor (dominant in late disease)
- M-tropic (R5) strains: Infect macrophages/monocytes using CCR5 as co-receptor (dominant in early infection, sexually transmitted)
- Dual-tropic strains: Use both co-receptors
3. Mode of Transmission
A. Sexual Transmission (Most Common)
- Vaginal, anal (highest risk for receptive partner), or oral sex
- Risk factors: high viral load in source, lack of condom use, concurrent STIs (especially ulcerative: syphilis, herpes, chancroid), uncircumcised male
- USA: ~70% of new infections in MSM (men who have sex with men), ~20% heterosexual
- Africa/Asia: heterosexual transmission dominant, equal sex distribution; accounts for >80% of new infections worldwide
B. Parenteral Transmission
- Sharing of contaminated needles/syringes (IV drug users) - 6% of US cases
- Blood/blood product transfusion (largely eliminated by screening)
- Needlestick injuries in healthcare workers (risk ~0.3% per needlestick from HIV+ source)
- Occupational exposure: corneal/mucous membrane splash (risk ~0.09%)
C. Mother-to-Child Transmission (MTCT / Vertical)
- During delivery (birth canal) - most common
- Transplacental (in utero, less common)
- Breastfeeding
- Overall rate WITHOUT intervention: ~25-40%; WITH ART: <1% in US
- Major cause of pediatric AIDS
- Robbins & Kumar Basic Pathology; Sherris & Ryan's Medical Microbiology
4. Pathogenesis
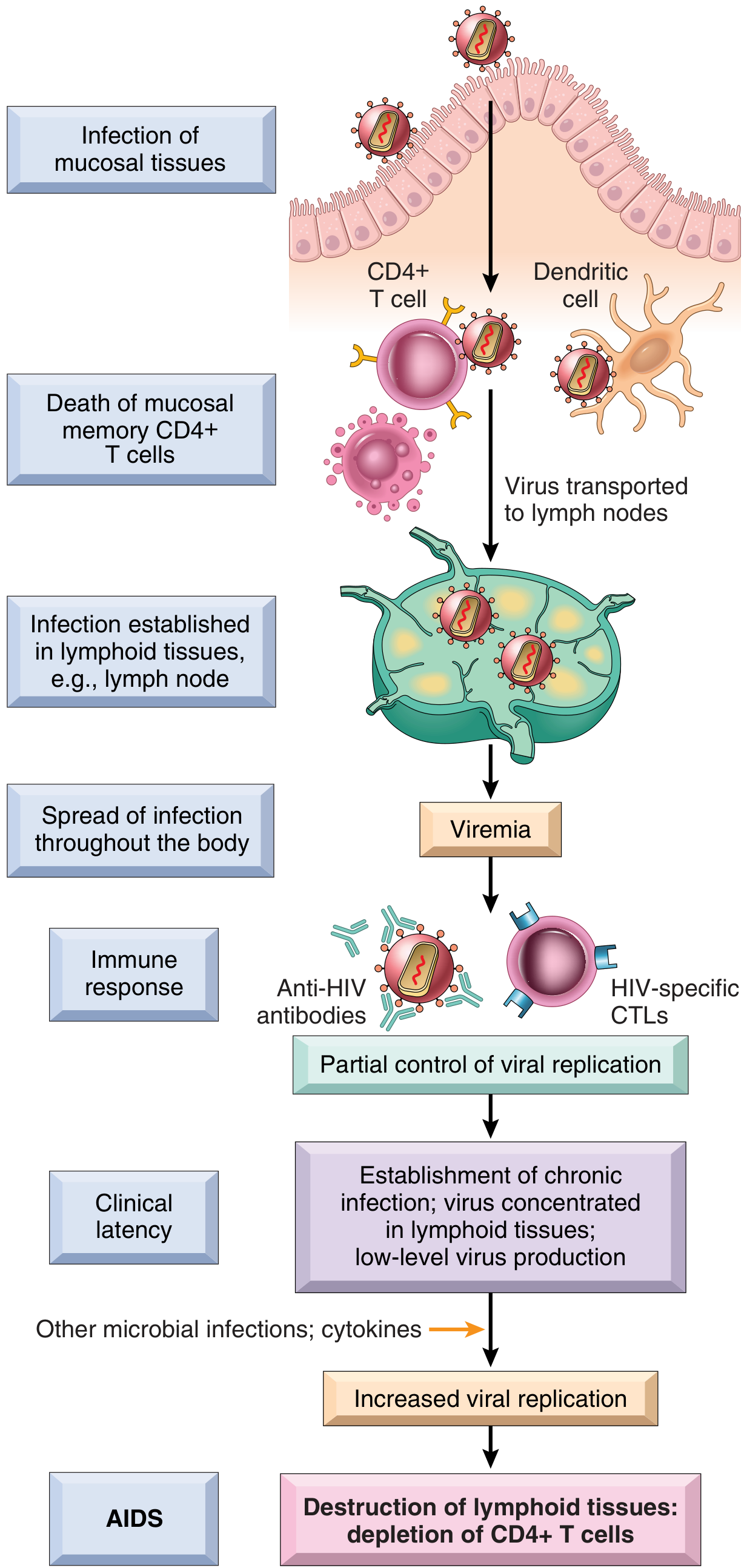
Step 1: Entry and Initial Infection
- gp120 binds CD4 on T helper cells and macrophages
- Co-receptor binding: CCR5 (early, M-tropic) or CXCR4 (later, T-tropic)
- gp41 mediates membrane fusion → viral core enters cytoplasm
- Memory CD4+ T cells in mucosal-associated lymphoid tissue (MALT/GALT) are the first major target - massive depletion occurs here early
- Dendritic cells in the epithelium capture virus and transport it to lymph nodes via direct cell-to-cell contact with CD4+ T cells
Step 2: Viremia and Dissemination
- Within days of exposure: viral replication in lymph nodes detectable
- High-level viremia: Virus disseminates throughout the body; infects CD4+ T cells, macrophages, and dendritic cells in peripheral lymphoid tissues
- Blood: >10^6 viral copies/mL during acute phase
Step 3: Immune Response and Acute HIV Syndrome
- 3-6 weeks post-infection: 40-90% of individuals develop acute HIV syndrome (acute retroviral syndrome / primary HIV infection)
- Host mounts humoral (anti-HIV antibodies) and cell-mediated (HIV-specific CD8+ cytotoxic T lymphocytes) responses
- Seroconversion occurs 3-7 weeks after exposure (window period)
- Viremia falls; patient enters clinical latency
Step 4: Chronic/Latent Phase
- Virus concentrates in lymphoid tissues; low-level ongoing replication continues
- CD4+ T cell count slowly declines (~50-100 cells/µL per year without ART)
- Lymph nodes: early reactive hyperplasia of B cell follicles → later follicular dissolution and lymphoid depletion (morphologic reflection of immunosuppression)
- Patient clinically asymptomatic; may have persistent generalized lymphadenopathy (PGL)
- Duration: typically 8-10 years without treatment (range 1-20 years)
Step 5: Progressive Immunodeficiency and AIDS
- HIV infects and kills CD4+ T cells through:
- Direct cytopathic effect (viral budding, pore formation)
- Immune-mediated killing of infected cells by CD8+ CTLs
- Syncytia formation (fusion of infected and uninfected cells)
- Chronic immune activation and bystander apoptosis
- Macrophages: infected but more resistant to cytopathic effects → serve as reservoirs
- CNS: HIV carried into brain by infected monocytes ("Trojan horse"); neurologic effects mostly indirect via viral products and cytokines from infected macrophages (neurons not directly infected)
HIV Reservoirs (Key barrier to cure)
- Cellular reservoirs: Resting CD4+ T cells (central memory TCM, transitional memory TTM, effector memory TEM) with integrated HIV provirus; CD34+ bone marrow stem cells
- Anatomical reservoirs: GALT (gut-associated lymphoid tissue), lymph nodes (low ART penetration); CNS
- Robbins & Kumar Basic Pathology; Sherris & Ryan's Medical Microbiology 8e
5. Clinical Stages / Natural History
Phase 1: Acute HIV Syndrome (Primary HIV Infection)
- Fever, myalgias, arthralgias
- Sore throat, pharyngitis
- Maculopapular rash (trunk and arms)
- Lymphadenopathy
- Headache, retroorbital pain
- Diarrhea, nausea, vomiting
- Oral ulcers (aphthous)
- Aseptic meningitis (in some)
Phase 2: Clinical Latency / Asymptomatic Phase
- Duration: ~8-10 years average without ART
- Patient asymptomatic or has only Persistent Generalized Lymphadenopathy (PGL): bilateral, non-tender, >1 cm, in ≥2 extrainguinal sites for >3 months
- Ongoing viral replication, gradual CD4+ decline
- Viral set point determines prognosis
Phase 3: Early Symptomatic HIV (WHO Stage 2-3)
- CD4 count ~200-500 cells/µL
- Recurrent bacterial infections, mucosal candidiasis, oral hairy leukoplakia, herpes zoster, seborrhoeic dermatitis, unexplained weight loss (<10%), chronic diarrhea, recurrent sinusitis, recurrent upper respiratory infections
Phase 4: AIDS (CDC Stage 3 / WHO Stage 3-4)
- CD4+ count <200 cells/µL, OR
- CD4+ percentage <14%, OR
- Presence of an AIDS-defining condition (regardless of CD4 count)
6. WHO Clinical Staging System
| Stage | Clinical Features | CD4 (approx.) |
|---|---|---|
| Stage 1 | Asymptomatic; PGL | >500 |
| Stage 2 | Weight loss <10%; minor mucocutaneous conditions (herpes zoster, seborrheic dermatitis, oral ulcerations, fungal nail infections, recurrent upper RTIs) | 350-500 |
| Stage 3 | Weight loss >10%; unexplained chronic diarrhea >1 month; unexplained prolonged fever; oral candidiasis; oral hairy leukoplakia; pulmonary TB; severe bacterial infections (pneumonia, meningitis, empyema); acute necrotizing ulcerative stomatitis | 200-350 |
| Stage 4 (AIDS) | All AIDS-defining illnesses (see below) | <200 |
7. AIDS-Defining Conditions (CDC/WHO Stage 4)
Opportunistic Infections
- Pneumocystis jirovecii pneumonia (PCP) - CD4 <200
- Cryptococcal meningitis - CD4 <100
- Disseminated histoplasmosis, coccidioidomycosis
- Esophageal candidiasis - CD4 <100
- Penicilliosis (Talaromyces marneffei) - Southeast Asia
- Disseminated Mycobacterium avium complex (MAC/MAI) - CD4 <50
- TB (both pulmonary and extrapulmonary) - any CD4 count
- Recurrent Salmonella septicemia
- Recurrent pneumonia (>2 episodes in 12 months)
- CMV retinitis/colitis/esophagitis - CD4 <50
- HSV chronic ulcers >1 month; bronchitis, pneumonitis, esophagitis
- Progressive multifocal leukoencephalopathy (PML) - JC virus - CD4 <50
- Disseminated toxoplasmosis (cerebral toxoplasmosis) - CD4 <100
- Cryptosporidiosis with diarrhea >1 month
- Microsporidiosis
- Isosporiasis
AIDS-Defining Malignancies
- Kaposi's sarcoma (HHV-8) - vascular skin lesions, violaceous plaques; visceral involvement
- Non-Hodgkin lymphoma (particularly Burkitt's and diffuse large B-cell)
- Primary CNS lymphoma (EBV-associated) - CD4 <50
- Invasive cervical carcinoma (HPV-related)
Neurologic AIDS-Defining Conditions
- HIV-associated neurocognitive disorder (HAND) / HIV encephalopathy - most common cause of dementia under 50 in pre-ART era
- Vacuolar myelopathy
- Progressive encephalopathy
8. Systemic Effects by Organ System
| System | Manifestations |
|---|---|
| Pulmonary | PCP (most common OI in developed world), TB, MAC, CMV pneumonitis, bacterial pneumonia, Kaposi's sarcoma |
| GI | Oral candidiasis, oral hairy leukoplakia, esophageal candidiasis, CMV colitis/esophagitis, cryptosporidiosis (watery diarrhea), MAC enteritis, KS of gut |
| CNS | HIV encephalopathy (dementia), toxoplasma abscess, PML, cryptococcal meningitis, CNS lymphoma, vacuolar myelopathy, peripheral neuropathy |
| Ophthalmic | CMV retinitis (most common cause of blindness in AIDS) |
| Dermatologic | Kaposi's sarcoma, seborrhoeic dermatitis, molluscum contagiosum, oral hairy leukoplakia, recurrent herpes, prurigo, drug rashes |
| Hematologic | Anemia, thrombocytopenia (immune ITP), leukopenia; lymphoma |
| Renal | HIV-associated nephropathy (HIVAN) - collapsing FSGS; most common in Black patients |
| Cardiovascular | Cardiomyopathy; in ART era: accelerated atherosclerosis, dyslipidemia |
| Endocrine | Adrenal insufficiency (CMV adrenalitis); thyroid dysfunction |
| Musculoskeletal | Myopathy (HIV or AZT-related), septic arthritis, avascular necrosis |
9. Laboratory Diagnosis
A. Tests for HIV Infection
- Gold standard for initial screening
- Detects: HIV-1/2 antibodies + p24 antigen simultaneously
- Positive from 18-45 days post-infection (shorter window period than 3rd-generation Ab-only tests)
- If reactive: confirm with HIV-1/HIV-2 antibody differentiation immunoassay
- If confirmatory test negative/indeterminate: order HIV RNA NAAT (to detect acute infection)
- Detects HIV antibodies; sensitivity ~99.5%, specificity ~99.5%
- Reactive ELISA must be confirmed with Western blot or differentiation assay
- Window period: 3-12 weeks (average 6 weeks) for 3rd-generation; shorter for 4th-generation
- Detects antibodies to specific HIV proteins
- Positive: Bands to p24, gp41, gp120/160
- Indeterminate: Insufficient bands - repeat in 1 month or do RNA test
- Being replaced by HIV-1/HIV-2 differentiation immunoassay in many settings
- Detects viral RNA as early as 10-14 days post-infection
- Used for: diagnosing acute HIV (seronegative window period), confirming diagnosis in indeterminate serology, pediatric diagnosis in infants born to HIV+ mothers
- Essential for viral load monitoring (see below)
- Point-of-care; results in 20-30 minutes; detect HIV antibodies
- Used for urgent situations, resource-limited settings
- All reactive rapid tests require confirmatory testing
- Detects viral core protein; positive from ~2 weeks post-infection
- Now usually part of 4th-generation combination test
B. Monitoring Tests (for HIV+ Patients)
- Absolute number (cells/µL) and percentage
- Normal: 500-1500 cells/µL
- Indicates degree of immunosuppression and risk of OIs:
| CD4 Count | Risk |
|---|---|
| >500 | Near normal immune function |
| 200-500 | Increased susceptibility to bacterial infections, TB, herpes zoster |
| 100-200 | PCP, toxoplasmosis, cryptosporidiosis, candidiasis |
| 50-100 | CMV retinitis, MAC, cryptococcal meningitis |
| <50 | MAC, PML, CNS lymphoma, CMV; most severe OIs |
- Measured in copies/mL; ideally expressed as log10
- Goals of ART: achieve viral suppression <50 copies/mL (undetectable)
- "Undetectable = Untransmittable" (U=U): virally suppressed patients do not sexually transmit HIV
- Monitored: baseline, 2-4 weeks after starting/changing ART, then every 3-6 months
- Virologic failure: Detectable viral load (>200 copies/mL) after 6 months of ART
- Performed at: HIV diagnosis (before starting ART), virologic failure, any change due to failure
- Identifies resistance mutations in reverse transcriptase, protease, and integrase genes
- Guides selection of active ART drugs
-
Cryptococcal antigen (serum, CSF)
-
CMV PCR (serum, vitreous)
-
Toxoplasma serology (IgG)
-
TB testing (IGRA, sputum AFB)
-
Hepatitis B and C serology
-
Sherris & Ryan's Medical Microbiology; Robbins & Kumar Basic Pathology; Harrison's Principles 22E
10. Antiretroviral Therapy (ART)
When to Start
Classes of Antiretroviral Drugs
| Class | Examples | Mechanism |
|---|---|---|
| NRTIs (Nucleoside/Nucleotide Reverse Transcriptase Inhibitors) | Tenofovir DF (TDF), Tenofovir AF (TAF), Emtricitabine (FTC), Lamivudine (3TC), Abacavir (ABC), Zidovudine (AZT) | Competitive inhibition + chain termination of reverse transcriptase |
| NNRTIs (Non-Nucleoside RTIs) | Efavirenz (EFV), Rilpivirine (RPV), Doravirine (DOR), Nevirapine (NVP), Etravirine (ETR) | Non-competitive binding to reverse transcriptase; not active against HIV-2 |
| PIs (Protease Inhibitors) | Darunavir (DRV), Atazanavir (ATV); always boosted with ritonavir (RTV) or cobicistat | Inhibit viral protease, prevent cleavage of polyproteins |
| INSTIs (Integrase Strand Transfer Inhibitors) | Dolutegravir (DTG), Bictegravir (BIC), Raltegravir (RAL), Elvitegravir (EVG), Cabotegravir (CAB) | Block viral integrase; prevent integration of viral DNA into host genome; now preferred class |
| Entry Inhibitors | Maraviroc (MVC) - CCR5 antagonist; Enfuvirtide (T-20) - fusion inhibitor; Fostemsavir (FTR) - CD4 attachment inhibitor; Ibalizumab (TMB-355) - anti-CD4 monoclonal antibody | Block viral entry at different steps |
| Pharmacokinetic Enhancers (Boosters) | Ritonavir (RTV), Cobicistat | Inhibit CYP3A4 → increase levels of co-administered PIs/INSTIs |
Preferred First-Line Regimens (Current US DHHS Guidelines)
- Biktarvy (Bictegravir/TAF/FTC) - single pill, once daily; most commonly prescribed
- Dolutegravir + TAF or TDF + FTC/3TC
- Dolutegravir + ABC + 3TC (Triumeq) - if HLA-B*5701 negative
- Dolutegravir + 3TC (Dovato) - for hepatitis B-negative patients with baseline viral load <500,000 copies/mL
- Cabotegravir (CAB) + Rilpivirine (RPV) long-acting - given as IM injections every 1 or 2 months; improves adherence; equivalent efficacy to daily oral ART
- Represents a major shift in how ART is delivered
Principles of ART Use
- Never use monotherapy - rapid resistance develops
- Minimum of 3 active agents from ≥2 classes (or 2-drug INSTI-based regimens in selected patients)
- Goal: HIV RNA <50 copies/mL (undetectable) on all monitoring tests
- Adherence is critical - even brief gaps lead to resistance
- Drug resistance testing before starting therapy and at virologic failure
- Fixed-dose combinations (FDCs) greatly improve adherence
Key Side Effects of ART
| Drug | Notable Toxicity |
|---|---|
| TDF | Renal tubular dysfunction, bone density loss |
| TAF | Better renal/bone profile than TDF; some weight gain |
| ABC | Hypersensitivity reaction (HLA-B*5701 associated) - potentially fatal if re-exposed |
| AZT | Anemia, bone marrow suppression, myopathy, lipoatrophy |
| Efavirenz | CNS effects (vivid dreams, dizziness), teratogenic (avoid in pregnancy) |
| PIs | GI intolerance, lipodystrophy, hyperlipidemia, insulin resistance |
| INSTIs | Generally well tolerated; weight gain (especially DTG/CAB in women); neuropsychiatric (raltegravir) |
| Ritonavir (booster dose) | Multiple CYP450 drug interactions |
Immune Reconstitution Inflammatory Syndrome (IRIS)
- Paradoxical worsening of a pre-existing OI after starting ART, despite rising CD4 and falling viral load
- Due to restored immune response attacking residual antigens
- Common with: TB, cryptococcal meningitis, MAC, CMV, Kaposi's sarcoma
- Management: Continue ART; NSAIDs or corticosteroids for severe cases
- Prevention: Delay ART for 2-4 weeks after starting TB or cryptococcal treatment
11. Prophylaxis for Opportunistic Infections
| OI | CD4 Threshold | Primary Prophylaxis | Drug |
|---|---|---|---|
| PCP | <200 cells/µL | Yes | TMP-SMX (cotrimoxazole) DS one tablet daily (also covers toxoplasmosis) |
| Toxoplasmosis | <100 cells/µL | Yes (if IgG+) | TMP-SMX (same regimen covers PCP) |
| MAC (disseminated) | <50 cells/µL | Yes | Azithromycin 1200 mg weekly OR clarithromycin 500 mg twice daily |
| Cryptococcal meningitis | <100 cells/µL (high burden) | Fluconazole 200 mg daily (in high-burden settings) | Fluconazole |
| TB (LTBI) | All HIV+ individuals | Yes (regardless of CD4 in high-burden settings) | 3HP, 6H, or other WHO-approved LTBI regimen |
| CMV retinitis | <50 cells/µL (if CMV IgG+) | Consider oral ganciclovir | Valganciclovir |
12. Prevention of HIV
A. Pre-Exposure Prophylaxis (PrEP)
- MSM or bisexual men not using condoms
- Transgender individuals
- Multiple sexual partners
- History of STIs
- Individuals from high-prevalence areas (≥3%)
- Injection drug users sharing equipment
- Sex workers
- Daily oral TDF/FTC (Truvada) - highly effective (~99% when adherent)
- On-demand/pericoital TDF/FTC (2-1-1 regimen) - for planned sex in MSM
- Long-acting injectable Cabotegravir (CAB-LA) - every 2 months IM injection; now recommended as first-line PrEP for all sexual risk populations; superior to oral TDF/FTC in trials (HPTN 083, HPTN 084)
B. Post-Exposure Prophylaxis (PEP)
- TDF 300 mg + FTC 200 mg (once daily) + Dolutegravir 50 mg (once daily) OR Raltegravir 400 mg twice daily
- Darunavir/ritonavir is an alternative third drug
C. Prevention of Mother-to-Child Transmission (PMTCT)
- ART for all HIV+ pregnant women (regardless of CD4) - reduces MTCT from ~25-40% to <1%
- Elective cesarean section in women with detectable viral load near delivery
- Infant prophylaxis: Zidovudine or nevirapine syrup for 4-6 weeks after birth
- Avoidance of breastfeeding in resource-rich settings (where safe alternatives available)
D. Behavioral and Structural Prevention
- Condom use - consistent and correct use reduces transmission by ~70-80%
- Male circumcision - reduces risk in heterosexual men by ~60%
- Harm reduction for IDU: Needle/syringe exchange programs, opioid substitution therapy
- HIV testing and counseling - CDC recommends routine testing for all ages 13-64 at least once
- Treatment as Prevention (TasP): Undetectable = Untransmittable (U=U) - virally suppressed HIV+ individuals cannot transmit HIV sexually
- Education and behavior modification - cornerstone of any strategy
- Blood safety: Mandatory screening of blood donations; donor deferral criteria
- Healthcare worker precautions: Universal precautions; avoid recapping needles; immediate wound wash after exposure; prompt PEP initiation; HBV vaccination (important because HBV is 50x more transmissible than HIV from needlestick)
E. Vaccine Development
- Harrison's Principles of Internal Medicine 22E (2025); Goldman-Cecil Medicine; Robbins & Kumar Basic Pathology; Sherris & Ryan's Medical Microbiology 8e
Summary Table
| Feature | Key Points |
|---|---|
| Causative agent | HIV-1 (global) / HIV-2 (West Africa) - Retrovirus, Lentivirus |
| Genome | ssRNA, diploid; reverse transcriptase, integrase, protease |
| Main receptor | CD4 + co-receptor (CCR5 or CXCR4) |
| Primary target cell | CD4+ T helper lymphocytes |
| Main route transmission | Sexual (worldwide); MSM (USA) |
| Window period (4th gen test) | 18-45 days |
| AIDS definition (CD4) | <200 cells/µL or AIDS-defining condition |
| Most common OI (USA/Europe) | PCP (Pneumocystis jirovecii) |
| Most common OI (globally) | TB |
| Most common CNS complication | HIV encephalopathy (HAND) |
| AIDS-defining malignancy | Kaposi's sarcoma (HHV-8), Primary CNS lymphoma, Invasive cervical cancer |
| First-line ART | INSTI-based (Bictegravir/TAF/FTC preferred) |
| Goal of ART | HIV RNA <50 copies/mL (undetectable) |
| PrEP | TDF/FTC daily oral or Long-acting Cabotegravir IM |
| PEP duration | 28 days; start within 72 hours |
| PMTCT efficacy with ART | Reduces MTCT to <1% |
| Key barrier to cure | HIV reservoirs (resting CD4+ T cells, GALT) |
Rabies
Rabies - Comprehensive Review
1. Introduction
- ~55,000-59,000 deaths per year globally (WHO estimate)
- Nearly 100% mortality once clinical symptoms develop
- >95% of human deaths occur in Asia and Africa; dog bites cause >90% of deaths in developing countries
- First successful post-exposure prophylaxis: Louis Pasteur, July 1885 (9-year-old Joseph Meister after a dog bite)
2. Etiology / The Virus
- Family: Rhabdoviridae
- Genus: Lyssavirus (currently 14 species in 3 phylogroups)
- Type: Negative-sense, single-stranded RNA virus
- Bullet-shaped (unique - diagnostic shape), enveloped
- 70 nm × 180 nm
- Helical nucleocapsid (N protein) wrapped around the RNA genome
- Surface: knob-like glycoprotein (G) spikes embedded in the lipid envelope
- Matrix protein (M) lies between the nucleocapsid and envelope
- The glycoprotein (G) elicits virus-neutralizing and hemagglutination-inhibiting antibodies - the basis for vaccine immunity
- G protein binds to host cell receptors (nicotinic acetylcholine receptors at neuromuscular junctions, neural cell adhesion molecules, p75 neurotrophin receptor)
- Strains from different animals (bats, dogs, skunks, foxes, raccoons) show antigenic heterogeneity - this may explain occasional vaccine failures
- An RNA-dependent RNA polymerase is enclosed within the nucleocapsid
-
Worldwide: Dogs (primary reservoir, cause >90% human deaths globally)
-
North America: Bats (primary source of human rabies in USA), raccoons (eastern USA), skunks (central USA), foxes, coyotes
-
Europe: Foxes, bats
-
Small rodents (squirrels, rats, mice, hamsters) and lagomorphs (rabbits): rabies is rare in these animals
-
Hawaii: Rabies-free
-
Sherris & Ryan's Medical Microbiology 8e; Red Book 2021
3. Epidemiology and Transmission
Transmission Routes
- Animal bite - virus transmitted via infected saliva
- Scratch with contaminated saliva on broken skin
- Lick on broken skin or mucous membranes
- Aerosol transmission - documented in bat-inhabited caves (Frio cave, Texas) and laboratory accidents
- Organ/corneal transplantation from donors dying of unrecognized rabies (documented clusters - 2004: 4 recipients died; corneal transplants)
- No documented person-to-person bite transmission in the USA
- Small rodents (squirrels, rats, mice, hamsters, gerbils, chipmunks), rabbits, hares - rabies is extremely rare in these species
- Animals with intact vaccination status that remain healthy for 10 days after bite
Animal observation rule:
- A dog, cat, or ferret that remains healthy for 10 days of confinement after biting a person has NOT transmitted rabies - no PEP needed
- Unimmunized biting animals should be euthanized and brain tested
4. Pathogenesis
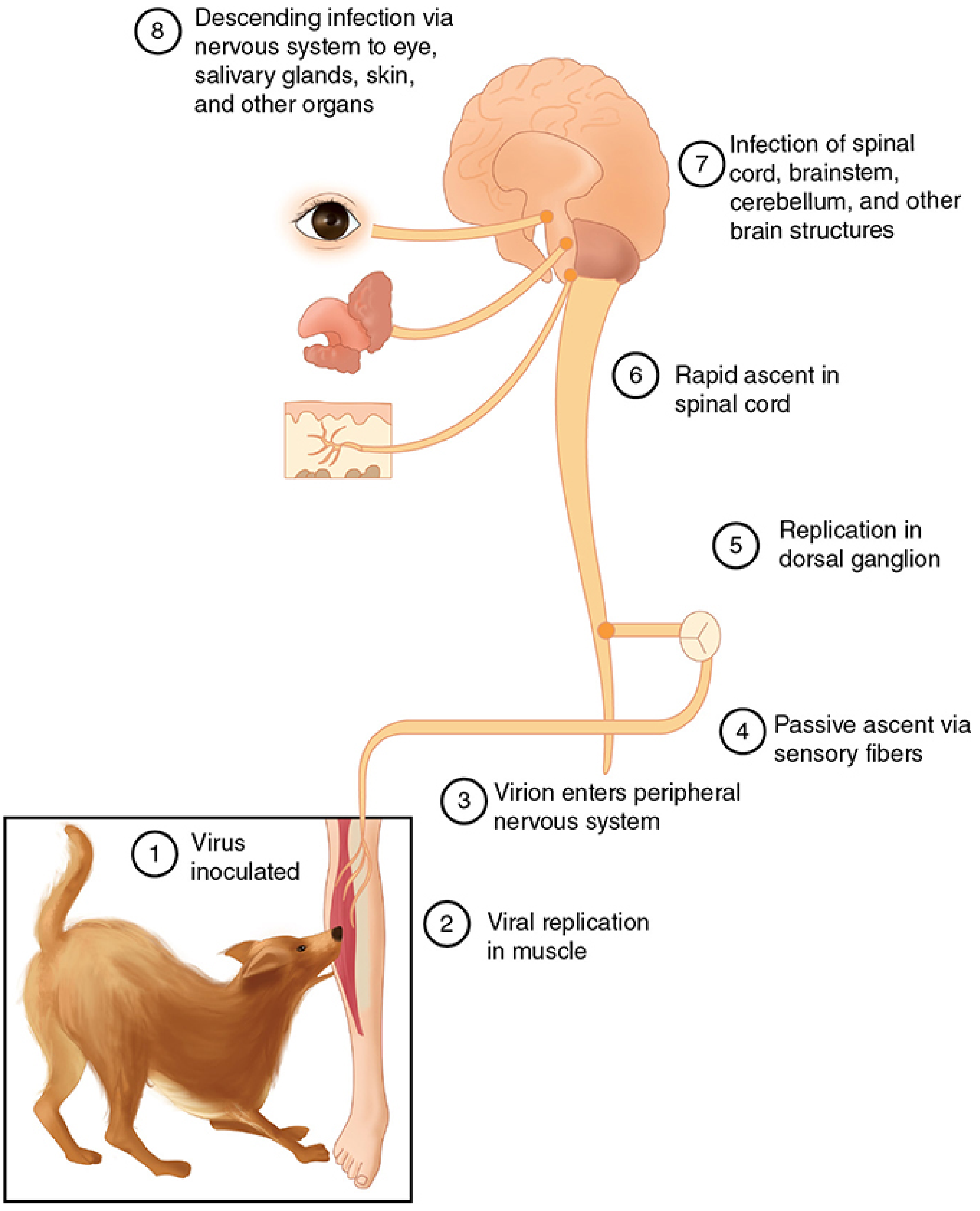
Step 1: Inoculation
- Virus inoculated through epidermis (animal bite)
- Also possible via inhalation of heavily contaminated aerosol
Step 2: Replication in Muscle
- Virus first replicates in striated muscle tissue at the site of inoculation
- This "peripheral replication phase" provides the window of opportunity for vaccination to prevent neural invasion
- Immunization given during this phase can prevent migration into neural tissues
Step 3: Entry into Peripheral Nervous System
- Virus binds to receptors at neuromuscular junctions and enters peripheral nerve endings
- Travels centrally by retrograde axonal transport (not via bloodstream)
- Rate of spread: ~3 mm/hour along axons
Steps 4-5: Passive Ascent via Sensory Fibers, Replication in Dorsal Ganglion
- Travels up sensory fibers to dorsal root ganglia
- Replicates in dorsal ganglion (explains paresthesias at bite site as an early symptom)
Step 6-7: Rapid Ascent to CNS
- Rapid ascent in the spinal cord → brainstem, cerebellum, cerebral cortex
- Replicates exclusively within the gray matter of the CNS
- Neuropathology: lymphocytic infiltration, neuronal destruction, most severe in brainstem, limbic system, hippocampus
Step 8: Centrifugal Spread (Descending)
- After CNS infection established, virus spreads centrifugally along autonomic nerves to:
- Salivary glands → facilitates transmission to next host
- Adrenal medulla
- Kidneys
- Lungs
- Eyes, skin (corneal epithelium - explains diagnostic utility of nuchal skin biopsy)
Key Neuropathological Feature: Negri Bodies
- Negri bodies = eosinophilic, oval or round intracytoplasmic inclusions in neurons
- Pathognomonic for rabies
- Located in: hippocampus (Ammon's horn - most common site), cerebral cortex, cerebellum (Purkinje cells), dorsal spinal ganglia
- Represent accumulations of viral nucleocapsid proteins
- Found in 75-90% of rabies cases in dogs by microscopy
- Size: 2-10 µm; may contain a central darkly staining granule
Why rabies has a variable incubation period:
-
Incubation depends on distance from bite to CNS (leg bite longer than face/neck bite), viral inoculum, and site-specific nerve density
-
Face/neck bites → short incubation; lower limb bites → longer incubation
-
Sherris & Ryan's Medical Microbiology 8e; Bradley and Daroff's Neurology; Park's Preventive Medicine
5. Incubation Period
- Usual: 1-3 months (average 20-90 days)
- Range: 10 days to several years (documented up to 6+ years)
- Factors determining incubation:
- Shorter: Head/neck/face bites, multiple deep wounds, high viral inoculum, bites near nerve-rich areas
- Longer: Lower extremity bites, distal wounds, low inoculum
- Incubation in dogs: 3-8 weeks (range: 10 days to >1 year)
6. Clinical Features
Phase 1: Prodromal Phase (2-10 days)
- Fever, malaise, headache, fatigue
- Anorexia, nausea, vomiting
- Paresthesias, pain, or pruritus at the bite site - highly characteristic (reflects viral replication in dorsal root ganglia)
- Anxiety, agitation, depression
- Sore throat, cough
Phase 2: Acute Neurological Phase
A. Furious (Encephalitic) Rabies (~80% of cases)
- Hydrophobia (fear of water) - present in up to 80% of patients
- Severe, painful spasms of pharyngeal and nuchal muscles on swallowing or seeing water
- Triggered by: swallowing attempts, tactile, auditory, visual, olfactory stimuli
- Spasms last 1-5 minutes
- Mechanism: exaggerated respiratory tract protective reflex
- Aerophobia - spasms triggered by air blown on the face
- Hyperactivity, agitation, confusion, hallucinations
- Autonomic hyperactivity: hypersalivation ("foaming at the mouth"), excessive sweating, piloerection, hyperthermia (up to 105-107°F), tachycardia, hypertension
- Seizures
- Cranial nerve palsies
- Bat-acquired rabies more commonly shows: tremor, myoclonus, local sensory symptoms at the exposure site, abnormal cranial nerve and motor examinations
B. Paralytic (Dumb) Rabies (~20% of cases)
- Characterized by ascending flaccid paralysis resembling Guillain-Barré syndrome
- Paresthesias and weakness in the bitten extremity → progressive quadriplegia
- Hydrophobia less prominent or absent
- More commonly seen with bat-acquired rabies
- Consciousness preserved longer than in furious form
- Often misdiagnosed as GBS - rabies should be in the differential of any unexplained ascending paralysis
Phase 3: Coma and Death
- Both forms progress to coma
- Death from: respiratory paralysis (major cause), cardiac arrhythmias, autonomic failure
- Survival after symptom onset: typically 2-7 days (furious); slightly longer in paralytic form
- Outcome: nearly universally fatal - only a handful of documented survivors (most following some pre-exposure vaccination history)
Clinical features in animals:
- Furious rabies in dogs: Change in behavior (cardinal sign), aggression, biting without provocation, running amuck, hoarse voice/inability to bark, excessive salivation and foaming, then paralysis
- Dumb rabies in dogs: Predominantly paralytic; withdrawal, sleepiness, death in ~3 days
- Infected animals rarely survive more than a week after symptom onset
7. Differential Diagnosis
- Tetanus (shorter incubation <2 weeks; trismus; normal CSF; no hydrophobia)
- Viral encephalitis (herpes, arboviral, EV-71)
- Guillain-Barré syndrome (for paralytic rabies)
- Intoxications (strychnine, atropine)
- Psychiatric illness, hysteria, rabies phobia (hysterical response to animal bite)
- Postvaccinal encephalitis (rare, with older nerve-tissue vaccines)
8. Laboratory Diagnosis
In Humans (Antemortem)
| Test | Specimen | Notes |
|---|---|---|
| Direct Fluorescent Antibody (DFA) / Immunofluorescence | Nuchal (posterior neck) skin biopsy - hair-bearing skin | Most rapid antemortem test; detects viral antigen around nerve endings in hair follicles; highest sensitivity |
| RT-PCR | Saliva, CSF, skin biopsy, brain tissue | Rapidly detects viral RNA sequences; saliva has best sensitivity; CSF sensitivity is low |
| Virus isolation | Saliva, brain tissue | Suckling mice or tissue culture; slow |
| Serology (neutralizing antibodies) | Serum and CSF | Diagnostic if unvaccinated patient has detectable antibodies; appear late (1-2 weeks into illness); high titers >1:5000 in active disease; useful in previously immunized patients |
| Corneal smear | Corneal epithelium | Rarely used due to low sensitivity |
In Animals (Postmortem)
| Test | Description |
|---|---|
| DFA (Direct Fluorescent Antibody) | Gold standard; brain tissue; highly specific; results within hours; equals virus isolation in accuracy |
| Microscopy for Negri bodies | Brain tissue (hippocampus); identifies 75-90% of rabid dogs; rapid but less sensitive than DFA |
| Mouse intracerebral inoculation | 10% brain emulsion injected intracerebrally into suckling mice; gold standard for isolation; watch for signs of rabies in mice over 28 days |
| Tissue culture | Virus isolation |
CSF findings:
- Mononuclear pleocytosis (present in >50% in first week, >87% beyond first week)
- Slightly elevated protein
MRI findings (when available):
-
T2/FLAIR signal abnormalities in gray matter: basal ganglia, thalamus, midbrain, pontine nuclei, brainstem, cortex
-
Park's Preventive Medicine; Bradley and Daroff's Neurology; Red Book 2021; Sherris & Ryan's Medical Microbiology
9. WHO Wound Category Classification and Post-Exposure Prophylaxis (PEP)
WHO Categories of Exposure
| Category | Type of Contact | PEP Required |
|---|---|---|
| Category I | Touching or feeding animals; licks on intact skin | None |
| Category II | Nibbling of uncovered skin; minor scratches or abrasions without bleeding | Immediate vaccination + local wound treatment |
| Category III | Single or multiple transdermal bites or scratches; licks on broken skin; contamination of mucous membranes with saliva; any bat contact | Immediate vaccination + Rabies Immunoglobulin (RIG) + local wound treatment |
- Biting animal is a known reservoir/vector species (bats, foxes, raccoons, skunks, dogs in endemic areas)
- Animal appears sick or behaves abnormally
- Wound or mucous membrane contaminated with saliva
- Bite was unprovoked
- Animal is unvaccinated or vaccination status unknown
- Biting animal cannot be traced
10. Post-Exposure Prophylaxis (PEP) - Detailed Steps
Step 1: Immediate Local Wound Treatment (Most Important First Step)
- Flush and wash wound thoroughly with plenty of soap and water, preferably under running tap, for at least 15 minutes
- If no soap available: flush with large volumes of water alone
- For puncture wounds: use catheters/syringes to irrigate deeply
- Should not be neglected even if hours or days have elapsed
- After cleansing, apply virucidal agent: 70% alcohol, tincture of iodine, or 0.01% aqueous povidone-iodine
- Inactivates residual virus
- Do NOT immediately suture bite wounds - avoids spreading virus into deeper tissues
- If suturing is necessary: delay 24-48 hours, apply minimum stitches, under cover of RIG locally
- Give antibiotics if wound infection risk
- Anti-tetanus prophylaxis as indicated
Step 2: Rabies Immunoglobulin (RIG) - Passive Immunization (Category III only)
- Human Rabies Immunoglobulin (HRIG): 20 IU/kg body weight
- Equine Rabies Immunoglobulin (ERIG) / F(ab')₂ products: 40 IU/kg body weight (purified equine products now safe and effective)
- Administer once only, preferably at the time of first vaccine dose (can be given up to day 7 after first vaccine dose; after day 7, active antibody response is presumed to have occurred, so RIG is NOT indicated)
- As much as anatomically feasible should be infiltrated directly into and around the wound(s)
- Remaining volume: inject intramuscularly at a site distant from vaccine injection site
- Do NOT exceed the recommended dose - may partially suppress active antibody production
- RIG can be diluted to sufficient volume to infiltrate all wounds without causing compartment syndrome
Step 3: Active Immunization - Rabies Vaccines
- HDCV - Human Diploid Cell Vaccine (gold standard; embryonic fibroblast cells)
- PCECV - Purified Chick Embryo Cell Vaccine
- PVRV - Purified Vero Cell Rabies Vaccine (Vero cells - African green monkey kidney)
- PDEV - Purified Duck Embryo Vaccine
- Primary hamster kidney cell vaccine
| Route | Schedule | Doses |
|---|---|---|
| IM (Intramuscular) | Days 0, 3, 7, 14 (Essen regimen) | 4 doses, 1.0 mL deltoid each |
| IM (Zagreb/2-1-1 regimen) | Day 0 (2 sites), Day 7 (1 site), Day 21 (1 site) | Accelerated schedule |
| ID (Intradermal) - 2-site regimen | Days 0, 3, 7, 28 at 2 sites (0.1 mL per site) | 0.1 mL/site; uses 1/5 of IM dose - economical |
- No RIG required (already have protective antibodies)
- Vaccine only: Days 0 and 3 (2 doses IM or ID) OR single-visit 4-site ID regimen
- Condition: documented complete prior PrEP or PEP with CCEEV OR neutralizing antibody titre ≥0.5 IU/mL
- 5 full IM doses required
- Comprehensive wound management + RIG infiltration
- Check neutralizing antibody titre 2-4 weeks after vaccination
Important notes on vaccine administration:
- Inject in the deltoid (adults) or anterolateral thigh (young children) - never in the gluteal area (poor absorption)
- Vaccine and RIG must be given at separate anatomical sites
- People taking chloroquine (malaria prophylaxis/treatment) should receive rabies vaccine IM, not ID (reduced response with intradermal route)
11. Pre-Exposure Prophylaxis (PrEP)
- Veterinarians, animal handlers, wildlife workers
- Laboratory workers handling rabies virus
- Travelers to endemic areas with limited healthcare access (especially long-term travelers >1 month)
- Cave explorers (spelunkers - bat exposure risk)
- Children in endemic areas (due to higher risk of unrecognized bites)
- 3 doses IM or ID: Days 0, 7, 21 or 28
- Still require post-exposure wound treatment + 2 booster doses (days 0 and 3)
- No RIG required in previously vaccinated individuals
- Healthcare workers and lab personnel: every 2 years (or based on serological monitoring; maintain titre ≥0.5 IU/mL)
12. Treatment of Clinical Rabies
- Sedation (benzodiazepines, barbiturates) for agitation, seizures, spasms
- Analgesia for pain
- Airway management, mechanical ventilation
- Management of autonomic instability
- Isolation precautions (universal precautions; staff vaccination)
13. Prevention and Control
Primary Prevention (Avoiding Infection)
- Animal vaccination campaigns - mass vaccination of dogs is the most cost-effective intervention; WHO target: vaccinate ≥70% of dog population in endemic areas
- Wildlife rabies control - oral rabies vaccine (ORV) baits distributed in wildlife habitats (especially effective in Europe for fox rabies elimination)
- Elimination of stray dogs in endemic areas
- Public education - avoid contact with wild/unknown animals; do not feed stray animals; teach children to report all animal bites
Secondary Prevention (After Exposure)
Healthcare Worker/Laboratory Protection
- Universal precautions for all contacts with suspected rabies patients
- Rabies virus isolated from saliva of infected patients - saliva should be treated as infectious
- All healthcare workers caring for rabies patients should be vaccinated
- Notify public health authorities after any potential exposure
Key facts for control:
- Over 90% of human deaths in developing countries are caused by dog bites
- Eliminating dog rabies would prevent the vast majority of human rabies deaths
- Hawaii is the only US state that is rabies-free (due to strict quarantine measures)
- Rabies is a notifiable disease in most countries
Summary Table
| Feature | Detail |
|---|---|
| Causative agent | Rabies virus - Rhabdoviridae, Lyssavirus genus |
| Genome | Negative-sense ssRNA |
| Shape | Bullet-shaped (70 × 180 nm) |
| Major reservoir globally | Dogs (>90% of human deaths) |
| Major reservoir USA | Bats |
| Incubation period | 10 days to years (average 1-3 months) |
| Incubation shorter with | Head/face/neck bites (close to CNS) |
| Pathognomonic finding | Negri bodies (eosinophilic intracytoplasmic inclusions) |
| Best site for Negri bodies | Hippocampus (Ammon's horn) |
| Two clinical forms | Furious (80%) and Paralytic/Dumb (20%) |
| Cardinal feature - furious | Hydrophobia and aerophobia |
| Fastest antemortem test | Nuchal skin biopsy + immunofluorescence (DFA) |
| Best animal diagnosis | DFA on brain tissue |
| Category I exposure | No PEP |
| Category II exposure | Vaccine + wound care; NO RIG |
| Category III exposure | Vaccine + RIG + wound care |
| HRIG dose | 20 IU/kg (infiltrate into wound) |
| ERIG dose | 40 IU/kg |
| RIG given beyond day 7 | NOT indicated |
| Vaccine schedule (unvaccinated) | Days 0, 3, 7, 14 (IM) |
| Vaccine route NOT recommended | Gluteal/buttock injection |
| Mortality after symptoms | Nearly 100% |
| Only proven prevention | PEP (prompt wound care + RIG + vaccine) |
Hepatitis
Hepatitis - Comprehensive Review
Overview Comparison Table
| Feature | Hep A (HAV) | Hep B (HBV) | Hep C (HCV) | Hep D (HDV) | Hep E (HEV) |
|---|---|---|---|---|---|
| Virus family | Picornaviridae | Hepadnaviridae | Flaviviridae | Deltaviridae | Hepeviridae |
| Genome | +ss RNA | Partially ds DNA | +ss RNA | -ss RNA (circular) | +ss RNA |
| Size | 27 nm | 42 nm (Dane) | 50-60 nm | 36 nm | 32-34 nm |
| Transmission | Fecal-oral | Parenteral/sexual/vertical | Parenteral | Parenteral (needs HBV) | Fecal-oral |
| Incubation | 15-50 days | 45-180 days | 14-180 days | Same as HBV | 15-60 days |
| Chronicity | Never | 5-10% adults; 90% neonates | 70-85% | 90-100% (superinfection) | Never (except in immunocompromised) |
| Fulminant hepatitis | Rare | Yes | Rare | Yes (esp. coinfection) | High in pregnancy (~20%) |
| Cirrhosis risk | No | Yes | Yes | Very high | No (usually) |
| HCC risk | No | Yes | Yes | Yes (highest combined) | No |
| Vaccine available | Yes | Yes | No | Prevented by HBV vaccine | Available in China; not globally licensed |
1. Hepatitis A (HAV)
Virology
- 27 nm RNA picornavirus (non-enveloped)
- 4 capsid proteins (VP1-4); single serotype worldwide
- NOT cytopathic to hepatocytes - liver injury is immune-mediated (both cellular and humoral)
- Stable in environment; resistant to drying, heating to 60°C
Epidemiology and Transmission
- Fecal-oral route - primarily via contaminated food or water
- Ingestion of raw shellfish from contaminated waters (classic)
- Person-to-person spread in households, day-care centers
- High-risk groups: people who inject drugs, MSM, travelers to endemic areas, persons exposed to sewage, raw seafood consumers
- Historically accounts for ~1/4 to 1/3 of acute hepatitis cases in USA
- Epidemics linked to waterborne and foodborne contamination
- Most virulent in middle-aged and older people; children often have subclinical infection
Clinical Features
- Incubation period: 15-50 days (average ~28 days)
- Acute illness: fever, malaise, anorexia, nausea, vomiting, right upper quadrant discomfort
- Jaundice develops in 50-70% of infected adults (but rarely in children)
- Most recover fully within 2-4 weeks
- No chronic form - always self-limiting
- Special situations:
- Cholestatic hepatitis A: Weeks of jaundice + pruritus in some adults
- Relapsing hepatitis A: In up to 5% of patients, 1-3 months after initial illness; associated with viremia but recovery always ensues
- Mortality ~2% in those over 60 years
- Can precipitate severe hepatitis or liver failure in patients with pre-existing chronic HBV or HCV
Diagnosis
| Test | Significance |
|---|---|
| IgM anti-HAV | Acute HAV infection; present at diagnosis; persists 3-6 months; use ONLY in clinical acute hepatitis setting (risk of false positives) |
| Total anti-HAV (IgG + IgM) | Past infection or vaccination; protective; persists lifelong |
| HAV RNA (research only) | Not used clinically |
Treatment
- Supportive only: Rest, adequate nutrition, avoid alcohol and hepatotoxic drugs
- No specific antiviral therapy
Prevention
- Vaccine: Three types: monovalent HAV, combined HAV+HBV (Twinrix), combined HAV+typhoid
- Schedule: 2 doses (day 0 and booster at 12 months) → immunity up to 20 years
- All children should be immunized; adults at high risk; international travelers
- Passive immunization: Normal immune globulin (IG) can be given for post-exposure prophylaxis within 2 weeks of exposure in unvaccinated individuals
2. Hepatitis B (HBV)
Virology
- 42 nm DNA virus = Dane particle (complete, infectious virion)
- Family: Hepadnaviridae
- Genome: Partially double-stranded circular DNA, ~3200 nucleotides
- Overlapping reading frames (one of the most compact genomes)
- Uses reverse transcriptase activity (like retroviruses) - error-prone, high mutation rate
| Protein | Encoded by | Significance |
|---|---|---|
| HBsAg (Surface antigen) | S gene (small form) | Coat of virion + excess subviral particles; marker of infection; basis of vaccine and detection |
| HBcAg (Core antigen) | C gene | Intracellular; part of infectious core; NOT detected in serum by routine tests |
| HBeAg (e antigen) | Pre-C/basal core promoter | Secreted protein; marker of active viral replication and high infectivity |
| HBV DNA polymerase | P gene | Reverse transcriptase + RNase H activity; target of NUC drugs |
| HBx protein | X gene | Transactivating factor; involved in viral replication and possibly HCC development |
| S1 protein (large surface) | Pre-S1 + S gene | Forms surface coat of circulating Dane particles |
- Genotype A: North America, Northern Europe
- Genotype C: Asia (higher risk of cirrhosis, HCC, poor IFN response)
- Genotypes A, B: Better response to interferon
- Clinical importance: predictor of natural course and treatment response
Epidemiology and Transmission
- Most common chronic viral infection worldwide: ~350 million chronically infected
- Highest prevalence: Southeast Asia, sub-Saharan Africa (>8% population)
- Routes:
- Parenteral: Blood/blood products, sharing needles (IDU), needlestick injuries in HCW
- Sexual transmission: Especially MSM, heterosexual with multiple partners
- Vertical (mother-to-child): Most important route in endemic areas; occurs mainly perinatally (during delivery); transplacental rare (~2%)
- Without intervention: 90% of perinatally infected infants develop chronic HBV
- In adults: 5-10% develop chronic HBV after acute infection
Pathogenesis
- HBV is NOT directly cytopathic - liver damage is immune-mediated
- Hepatocytes express HBcAg + HLA class I proteins on surface → primed CD8+ T lymphocytes attack infected hepatocytes
- Chronic hepatitis results from incomplete immune clearance
- Many chronic HBV patients have deficient interferon response → cannot express adequate HLA antigens for lymphocyte targeting
| Phase | HBsAg | HBeAg | Anti-HBe | HBV DNA | ALT | Histology |
|---|---|---|---|---|---|---|
| Immune-tolerant | + | + | - | Very high (>10^8 IU/mL) | Normal | Minimal |
| Immune-reactive (HBeAg+) | + | + | - | High (>2000 IU/mL) | Elevated | Active hepatitis |
| Inactive carrier | + | - | + | Low/undetectable | Normal | Minimal |
| HBeAg-negative CHB | + | - | + | Variable (>2000 IU/mL) | Elevated | Active hepatitis |
| HBsAg clearance (resolved) | - | - | + | Very low/undetectable | Normal | Minimal fibrosis |
Clinical Features
- Incubation: 45-180 days (average 60-90 days)
- Prodrome: malaise, anorexia, nausea, RUQ discomfort, arthralgias, fever
- Icteric phase: jaundice, dark urine (bilirubinuria), pale stools, hepatomegaly, splenomegaly
- Serum sickness-like syndrome: urticaria, arthralgias (immune complex-mediated) - characteristic of HBV
- Resolution: most immunocompetent adults recover within 3-6 months
- Fulminant hepatitis: ~1% of cases; acute liver failure, encephalopathy, coagulopathy
- Most patients asymptomatic initially; detected by abnormal LFTs or screening
- Symptoms: fatigue, right upper quadrant discomfort
- Progressive: cirrhosis → portal hypertension → hepatocellular carcinoma (HCC)
- Extrahepatic manifestations (1-10% of patients, immune complex-mediated):
- Polyarteritis nodosa (most classic association)
- Glomerulonephritis (membranous)
- Cryoglobulinemia
- Polymyalgia rheumatica
- Myocarditis, Guillain-Barré syndrome
HBV Serology - Interpretation
| HBsAg | Anti-HBs | Anti-HBc IgM | Anti-HBc Total | HBeAg | Interpretation |
|---|---|---|---|---|---|
| + | - | + | + | + | Acute HBV (early) |
| + | - | - | + | +/- | Chronic HBV (replicating) |
| - | + | - | - | - | Vaccinated (immune via vaccine) |
| - | + | - | + | - | Past infection, immune (natural infection, resolved) |
| - | - | - | + | - | Resolved infection (anti-HBs not yet detectable = "core window") OR occult HBV |
| - | - | - | - | - | Never infected, not immune (susceptible) |
- HBsAg: First marker to appear in infection; active infection marker; persists >6 months = chronic
- Anti-HBs (≥10 IU/mL): Protective immunity; vaccine response or past resolved infection
- Anti-HBc IgM: Acute/recent infection (high titer); also positive in flares of chronic HBV (lower titer)
- Anti-HBc Total (IgG): Past or present infection; NOT induced by vaccine; marker of prior exposure
- HBeAg: Active viral replication, high infectivity
- Anti-HBe: Seroconversion = viral control, declining infectivity (but check HBV DNA - some precore mutants remain replicative)
- HBV DNA: Quantifies viral load; monitors treatment; definitive marker of active replication
- HBsAg quantification: Predicts treatment response; declining levels = treatment response
Laboratory Tests (LFTs)
- ALT > AST (in uncomplicated viral hepatitis)
- AST/ALT ratio >1 suggests alcohol-related liver disease or cirrhosis
- Elevated bilirubin, alkaline phosphatase, GGT
- Prolonged prothrombin time (PT) in severe/fulminant disease
HBV Treatment
- Finite duration (48 weeks); no resistance; stimulates host immune response
- Higher rate of HBeAg seroconversion and durable off-treatment response
- Side effects: flu-like symptoms, depression, cytopenia, autoimmune thyroiditis, teratogenic
- Contraindicated: decompensated cirrhosis, psychiatric disease, cytopenias, autoimmune disease, pregnancy
- Better response: Genotypes A and B; high ALT; low HBV DNA; low HBsAg
| Drug | Class | Advantages | Key Toxicity |
|---|---|---|---|
| Entecavir (ETV) | Nucleoside | Potent; high barrier to resistance; first-line | Lactic acidosis (rare) |
| Tenofovir disoproxil fumarate (TDF) | Nucleotide | Potent; high barrier to resistance; active against HBV+HIV; first-line | Nephrotoxicity, bone loss |
| Tenofovir alafenamide (TAF) | Nucleotide | Similar potency to TDF; better renal/bone safety; first-line | Less renal/bone toxicity |
| Lamivudine (3TC) | Nucleoside | Available but high resistance rate (~70% at 5 years) - no longer preferred | YMDD mutant resistance |
| Adefovir | Nucleotide | Older; low potency; renal toxicity | Nephrotoxicity |
| Telbivudine | Nucleoside | Moderate potency; resistance issues | Myopathy, neuropathy |
HBV Vaccination
- Recombinant HBsAg vaccine (Engerix-B, Recombivax HB)
- 3-dose schedule: 0, 1, 6 months (IM deltoid)
- Protective antibody level: anti-HBs ≥10 IU/mL
-
90% seroconversion in healthy adults; >95% in children
- Universal infant vaccination is global standard
- Perinatal prophylaxis for infants of HBsAg+ mothers:
- HBIG (0.06 mL/kg IM) + first dose HBV vaccine within 24 hours of birth
-
95% effective in preventing perinatal transmission
3. Hepatitis C (HCV)
Virology
- 50-60 nm enveloped flavivirus (+ss RNA)
- Family: Flaviviridae
- Genome encodes a single polyprotein cleaved into structural (Core, E1, E2) and non-structural proteins (NS2, NS3, NS4A, NS4B, NS5A, NS5B)
- NS5B = RNA-dependent RNA polymerase (target of sofosbuvir)
- NS5A = regulatory protein (target of ledipasvir, velpatasvir, pibrentasvir)
- NS3/4A = protease (target of glecaprevir, grazoprevir, voxilaprevir)
- 6 major genotypes (1-6) with subtypes; global distribution varies
- High mutation rate → quasispecies → major obstacle to vaccine development
Epidemiology and Transmission
- ~58-71 million people chronically infected worldwide
- Primarily parenteral transmission:
- IDU (sharing needles) - most common in developed countries
- Blood transfusions (before 1992 screening)
- Needlestick injuries in HCW
- Tattooing, piercing with contaminated equipment
- Sexual transmission: Low risk (0.07% per sexual encounter); higher in HIV+ MSM
- Vertical (mother-to-child): Low risk (~3-5%)
- Not transmitted by casual contact, sharing food, hugging
Clinical Features
- Incubation: 14-180 days (average 6-8 weeks)
- Mostly asymptomatic (70-80%) - "silent epidemic"
- 10-30% develop jaundice when clinical disease occurs
- ALT elevation typically ~6-8 weeks after infection
- HCV RNA detectable 1-2 weeks after exposure
- 15-25% clear infection spontaneously (especially younger women with IL28B CC genotype)
- 75-85% develop chronic infection (much higher than HBV in adults)
- Often asymptomatic for 20-30 years
- Fatigue is the most common symptom
- Progressive fibrosis → cirrhosis (20-30% of patients over 20-30 years)
- Cirrhosis → HCC (~1-4% per year)
- HCV is the leading indication for liver transplantation in many countries
- Mixed cryoglobulinemia (most characteristic) - purpura, arthralgia, neuropathy, glomerulonephritis
- Membranoproliferative glomerulonephritis (MPGN)
- Porphyria cutanea tarda (PCT)
- Lichen planus
- Non-Hodgkin lymphoma (B-cell)
- Insulin resistance/type 2 diabetes
- Sicca syndrome (Sjögren-like)
- Thyroid disorders
HCV Diagnosis
- 3rd generation ELISA: sensitivity >99%
- Window period: 2-3 weeks after infection (3rd gen); positive in ~50% at time of clinical acute presentation
- Positive anti-HCV requires confirmation with HCV RNA (as anti-HCV persists lifelong even after clearance)
- Does NOT distinguish active from past resolved infection
- Detectable 1-2 weeks after exposure (before antibodies)
- Gold standard for active infection
- Qualitative: confirms infection; detects acute infection when antibody negative
- Quantitative (viral load): monitors treatment response
- Determines duration and regimen selection
- Reference method: direct sequencing
- Rapid Virologic Response (RVR): Undetectable HCV RNA at week 4
- Early Virologic Response (EVR): ≥2 log10 decline by week 12
- Sustained Virologic Response (SVR): Undetectable HCV RNA 12-24 weeks after treatment completion = functional cure
HCV Treatment - Direct-Acting Antivirals (DAAs)
| Class | Target | Examples |
|---|---|---|
| NS5B nucleotide inhibitors | RNA polymerase (chain termination) | Sofosbuvir (SOF) - pangenotypic |
| NS5A inhibitors | Replication complex | Ledipasvir, Velpatasvir, Pibrentasvir, Daclatasvir |
| NS3/4A protease inhibitors | Viral protease | Glecaprevir, Grazoprevir, Voxilaprevir |
| Regimen | Brand | Genotypes | Duration |
|---|---|---|---|
| Sofosbuvir/Velpatasvir (SOF/VEL) | Epclusa | 1-6 (pangenotypic) | 12 weeks |
| Glecaprevir/Pibrentasvir (GLE/PIB) | Mavyret | 1-6 (pangenotypic) | 8-12 weeks |
| SOF/VEL + Voxilaprevir | Vosevi | 1-6; retreatment after DAA failure | 12 weeks |
| Ledipasvir/Sofosbuvir (LDV/SOF) | Harvoni | GT 1, 4, 5, 6 | 8-12 weeks |
- Treatment goal: SVR12 (undetectable HCV RNA ≥12 weeks post-treatment) = cure
- SVR reduces risk of HCC, liver failure, all-cause mortality
- Even cirrhotic patients can be treated (adjust regimen if decompensated)
- Ledipasvir/sofosbuvir: 99% SVR in treatment-naïve GT1 patients
- Drug interaction alert: Avoid rifampin (P-glycoprotein inducer) and St. John's wort with SOF-based regimens; avoid amiodarone with sofosbuvir (risk of fatal bradycardia)
- No vaccine available; prevention relies on harm reduction (needle exchange, safe sex)
4. Hepatitis D (HDV) - Delta Hepatitis
Virology
- 36 nm incomplete RNA virus (obligate satellite virus)
- Family: Deltaviridae
- Genome: Single-stranded, circular, antisense (negative-sense) RNA - the smallest mammalian viral genome
- Cannot replicate independently - requires HBsAg as its envelope protein
- Encodes only one protein: Delta antigen (HDAg)
Key Clinical Features
- Worldwide prevalence: ~4.5% among HBsAg-positive individuals
- High-risk regions: China, Russia, Eastern Europe, Africa, South America
- Risk factors: IDU, HCV/HIV coinfection, travel to endemic areas
- Extremely infectious; strongly associated with IV drug use
- ~10 million infected worldwide (declining with reduced HBV incidence)
- Typically self-limiting acute hepatitis
- Only 2-8% progress to chronic (same as HBV alone)
- Higher risk of fulminant hepatitis than HBV alone
- Higher mortality
- HDV superimposed on existing chronic HBV infection
- ~90-100% develop chronic HDV infection
- ~80% progress to cirrhosis within 5-10 years
- Estimated: cirrhosis 4%/year; HCC 3%/year
- Dramatic worsening of liver disease
HDV Diagnosis
| Test | Significance |
|---|---|
| Anti-HDV IgM | Acute HDV infection |
| Anti-HDV IgG (Total anti-HDV) | Chronic infection (persists) vs. resolved (disappears by ~32 weeks) |
| HDV RNA | Gold standard for active replication; used for monitoring |
| HDAg (Delta antigen) | Early acute infection; brief window |
Treatment
- Pegylated interferon-alpha was the only available therapy for decades (high relapse rates)
- Bulevirtide (Hepcludex): New entry inhibitor; prevents HDV entry by blocking sodium taurocholate cotransporting polypeptide (NTCP receptor); conditionally approved in Europe (2020)
- Prevention: HBV vaccination prevents HDV (cannot have HDV without HBV)
5. Hepatitis E (HEV)
Virology
- 32-34 nm non-enveloped RNA virus (+ss RNA)
- Family: Hepeviridae
- 4 major genotypes (GT1 and GT2: humans only; GT3 and GT4: zoonotic - pigs, deer, wild boar)
Epidemiology and Transmission
- Fecal-oral transmission (like HAV)
- GT1/2: Epidemic form in developing countries (South Asia, Central Asia, Africa, Mexico); contaminated water supplies; large outbreaks
- GT3/4: Sporadic zoonotic infection in developed countries (via undercooked pork, deer, game)
- High mortality in pregnant women: 15-25% mortality in third trimester (unique feature)
- Usually self-limiting; no chronic form in immunocompetent individuals
- Chronic hepatitis E occurs in immunocompromised patients (transplant recipients, HIV+, hematologic malignancy patients) with GT3/4
Clinical Features
- Incubation: 15-60 days (average ~40 days)
- Similar to HAV: fever, jaundice, nausea, RUQ pain
- Cholestasis often prominent
- Self-limiting; no chronic form in immunocompetent
- Extrahepatic: Neurological manifestations (Guillain-Barré, neuralgic amyotrophy) associated with GT3
- Pregnancy: Disproportionate severity, risk of fulminant hepatic failure, preterm labor, fetal loss; 15-25% mortality in third trimester
Diagnosis
| Test | Notes |
|---|---|
| Anti-HEV IgM | Acute HEV infection; present at time of jaundice |
| Anti-HEV IgG | Past infection or immunity |
| HEV RNA (PCR) | Detects viremia; needed in immunocompromised (serology may be negative); used to confirm chronic HEV |
Treatment
- Immunocompetent: Supportive only (self-limiting)
- Chronic HEV (immunocompromised):
- Reduce immunosuppression (first step)
- Ribavirin for 3-6 months (off-label; first choice)
- Pegylated interferon (second line; cannot use in transplant recipients)
Prevention
- Vaccine: HEV 239 (Hecolin) - licensed and available in China since 2012; not globally licensed
- Boil drinking water in endemic areas; avoid uncooked pork/game in developed countries
- Safe water supply and good sanitation
6. Hepatitis G (HGV/GBV-C)
- Flavivirus; bloodborne; co-infects with HIV
- Not clearly pathogenic - does not cause clinically significant hepatitis
- May actually be beneficial in HIV-infected individuals (slower HIV progression)
- No treatment indicated
7. General Clinical Features of Acute Viral Hepatitis
Phases
- Flu-like: fever, malaise, fatigue, headache, myalgia
- GI: nausea, vomiting, anorexia, RUQ discomfort
- Aversion to cigarettes and alcohol (characteristic)
- Arthralgia, urticaria (especially HBV - serum sickness-like)
- Pale/clay-colored stools; dark urine (bilirubinuria) appears before jaundice
- Jaundice (icteric sclera first), dark urine, pale stools
- Hepatomegaly, splenomegaly
- Tenderness in right hypochondrium
- Pruritus (especially if cholestatic)
- Systemic symptoms often improve when jaundice appears (unlike in fever-related jaundice)
- Jaundice resolves, appetite returns, fatigue improves
Complications
- Fulminant hepatic failure: Acute liver failure, encephalopathy, coagulopathy; highest risk with HBV+HDV coinfection, HEV in pregnancy
- Cholestatic hepatitis (prolonged jaundice, mainly HAV)
- Relapse (HAV - 5% of cases)
- Chronic hepatitis → cirrhosis → HCC (HBV, HCV, HDV)
8. Laboratory Investigations
Liver Function Tests (LFTs)
| Test | Finding | Interpretation |
|---|---|---|
| ALT (SGPT) | Elevated; ALT > AST in viral hepatitis | Most specific for hepatocyte injury |
| AST (SGOT) | Elevated | AST/ALT >2 suggests alcoholic hepatitis |
| AST/ALT ratio >1 | Cirrhosis or alcohol-related disease | |
| Bilirubin | Elevated (conjugated + unconjugated) | Jaundice when >3 mg/dL |
| Alkaline phosphatase | Mildly elevated | More elevated in cholestatic disease |
| GGT | Elevated | Sensitive for alcohol/drug-induced; tracks with ALP |
| Albumin | Decreased in chronic disease | Marker of synthetic function |
| PT/INR | Prolonged in severe disease | Most sensitive marker of acute hepatic failure |
| Platelet count | Decreased in cirrhosis (hypersplenism) |
Causes of Chronic Hepatitis (Diagnostic workup)
| Cause | Key Test |
|---|---|
| Hepatitis B | HBsAg, anti-HBs, anti-HBc, HBV DNA |
| Hepatitis C | Anti-HCV, HCV RNA PCR |
| Autoimmune type 1 | ANA, anti-smooth muscle antibody (ASMA) |
| Autoimmune type 2 | Anti-LKM1, anti-SLA |
| Wilson disease | Serum ceruloplasmin, 24h urine copper, slit-lamp |
| Drug-induced | History |
| Alpha-1 antitrypsin deficiency | AAT phenotype (Pi typing) |
| NAFLD/NASH | Metabolic syndrome, ultrasound, biopsy |
9. Histopathology of Viral Hepatitis
- Hepatocyte swelling (ballooning degeneration)
- Acidophil (Councilman) bodies - apoptotic hepatocytes
- Lobular disarray
- Mononuclear portal and lobular inflammatory infiltrate
- Cholestasis
- Interface hepatitis (periportal hepatocyte necrosis - "piecemeal necrosis")
- Portal inflammatory infiltrate
- Bridging necrosis (connecting portal tracts or central veins) = severe disease
- Fibrosis (staging: F0-F4)
- Grading (activity): degree of inflammation
- Staging (fibrosis): F0=none → F4=cirrhosis
10. Prevention Summary
| Virus | Vaccine | Post-exposure Prophylaxis |
|---|---|---|
| HAV | Yes - inactivated (2 doses) | Immune globulin + vaccine within 2 weeks |
| HBV | Yes - recombinant (3 doses) | HBIG + vaccine within 24 hours of birth; PEP within 24h of exposure |
| HCV | No | None (no vaccine, no IG); harm reduction only |
| HDV | Prevented by HBV vaccine | HBV vaccination prevents HDV |
| HEV | Yes (China only - Hecolin) | Avoid contaminated water; safe food handling |