Cleft palate and lip causes
Reading File
Finding Sources
Searching PubMed
"cleft lip" OR "cleft palate" etiology causes
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a comprehensive breakdown of the causes of cleft lip and cleft palate, drawn from embryology, genetics, and surgical textbooks.
Cleft Lip and Cleft Palate - Causes
Epidemiology at a Glance
- Cleft lip ± palate: ~1 in 1,000 births; more common in males (60-80% of cases)
- Isolated cleft palate: ~1 in 2,500 births; more common in females
- Overall distribution: cleft lip alone 15%, cleft lip + palate 45%, isolated cleft palate 40%
- Geographic variation: higher rates in South East Asian and Native American populations

Embryological Basis (the "how")
Understanding the cause requires knowing what goes wrong developmentally:
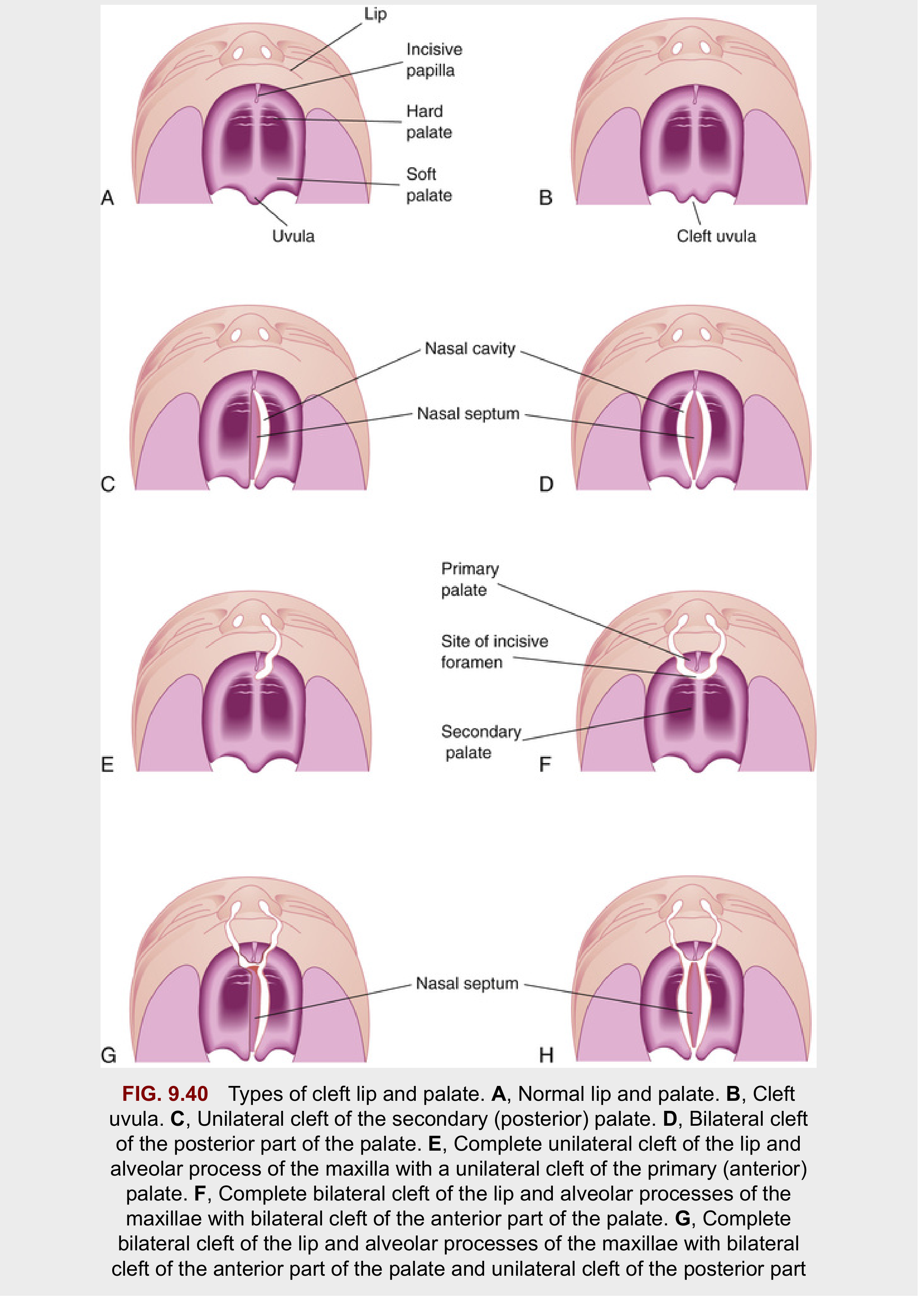
Cleft lip results from failure of the maxillary prominence on the affected side to fuse with the merged medial nasal prominences during weeks 5-7 of embryonic development. The mesenchymal masses fail to merge and proliferate under the overlying epithelium, leaving a persistent labial groove. The groove deepens, epithelium breaks down, and the lip divides into medial and lateral parts.
- Unilateral cleft lip: one-sided failure of this fusion
- Bilateral cleft lip: bilateral failure; median palatal process hangs free and projects anteriorly, with loss of continuity of the orbicularis oris muscle
- Median cleft lip (rare): results from mesenchymal deficiency causing failure of medial nasal prominences to merge - a feature of Mohr syndrome (autosomal recessive)
Cleft palate results from:
- Anterior (primary) palate clefts: failure of mesenchymal masses in the lateral palatal processes to meet and fuse with the mesenchyme in the primary palate
- Posterior (secondary) palate clefts: failure of the lateral palatine processes (palatal shelves) to meet, fuse with each other, and fuse with the nasal septum
- Contributing factors include abnormal width of the stomodeum, reduced mobility of the lateral palatine processes, and altered focal degeneration at palatal epithelial fusion sites
Causes
1. Multifactorial Inheritance (most common)
The majority of clefts arise from multifactorial inheritance - a combination of multiple small genetic and environmental factors, each causing a minor developmental disturbance. No single gene explains most cases. - The Developing Human: Clinically Oriented Embryology
2. Genetic Factors
Specific genes:
- IRF6 (Interferon Regulatory Factor 6): Strongly implicated in isolated cleft formation; one of the best-established genetic associations
- FGFR genes and growth factor signalling pathways are also implicated
- A cleft lip + alveolar process extending through the palate is often transmitted via a male sex-linked gene
Inheritance risk:
- When neither parent is affected, recurrence risk in siblings is ~4%
- First-degree relative affected significantly raises risk in the family
- A sibling of a child with cleft palate has elevated risk of cleft palate, but NOT increased risk of cleft lip (the two forms have different genetic underpinnings)
- Twin studies confirm genetics are more important in cleft lip ± palate than in isolated cleft palate
3. Chromosomal Abnormalities
- Trisomy 13 (Patau syndrome): Classically associated with midline cleft lip and palate
- Other chromosomal deletions and duplications can present with orofacial clefts
4. Syndromic Associations (>150 syndromes)
Isolated cleft palate is more commonly part of a syndrome than cleft lip + palate. Key syndromes include:
| Syndrome | Key Features |
|---|---|
| Stickler syndrome | Ophthalmic + musculoskeletal abnormalities |
| DiGeorge syndrome (22q11.2 deletion) | Cardiac defects, thymic aplasia, hypocalcaemia |
| Down syndrome (Trisomy 21) | Characteristic facies, intellectual disability |
| Apert syndrome | Craniosynostosis, syndactyly |
| Treacher Collins syndrome | Mandibulofacial dysostosis |
| Mohr syndrome | Median cleft lip, autosomal recessive |
| Pierre Robin sequence | Cleft palate, micrognathia, glossoptosis |
Over 300 recognized syndromes can include cleft lip/palate as a feature. - Bailey and Love's Short Practice of Surgery
5. Teratogenic Agents (Environmental)
Several drugs and exposures during the first trimester (particularly weeks 5-12 when lip and palate form) are established causes:
| Agent | Notes |
|---|---|
| Anticonvulsants | Phenytoin, valproate, phenobarbitone - among the best-documented teratogens |
| Corticosteroids | Particularly in first trimester |
| Alcohol | Fetal alcohol syndrome; cleft palate is a recognized feature |
| Retinoic acid (Vitamin A derivatives) | Isotretinoin (acne treatment) is a potent teratogen |
| Methotrexate | Folate antagonist; associated with orofacial clefts |
| Cigarette smoking | Well-established environmental risk factor |
| Maternal diabetes | Poorly controlled diabetes increases risk |
6. Folate Deficiency
Inadequate folic acid intake periconceptionally is a recognized risk factor. Folate supplementation has a protective effect - analogous to its role in neural tube defects.
7. Other Environmental/Maternal Factors
- Maternal hyperthermia (fever) in early pregnancy
- Maternal obesity
- Altitude/hypoxia in some studies
- Radiation exposure
Key Points to Remember
- Non-syndromic cleft lip/palate (the majority) is multifactorial - genetics + environment together
- Syndromic cleft palate (single-gene or chromosomal) is more likely when there are other anomalies
- Cleft lip ± palate and isolated cleft palate are embryologically and genetically distinct entities and should not be conflated
- All children born with a cleft are screened for other congenital abnormalities; genetic counselling is offered when a syndrome is suspected
A recent 2023 review of orofacial cleft genetics (PMID 37628654) has reinforced the role of IRF6 and other transcription factor mutations, and a 2025 review in Clinical Plastic Surgery (PMID 39986880) provides updated management context.
Sources: The Developing Human: Clinically Oriented Embryology; Bailey and Love's Short Practice of Surgery 28e; Creasy & Resnik's Maternal-Fetal Medicine
This is a shared conversation. Sign in to Orris to start your own chat.