pharmaceutical dosage forms
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Finding Sources
Now I have comprehensive content from the textbooks. Let me compile the full answer.
Pharmaceutical Dosage Forms
A dosage form is the physical formulation in which a drug is manufactured and administered to the patient. The choice of dosage form is determined by the drug's physicochemical properties (solubility, stability, ionization), the desired route of administration, the speed of onset required, and patient-related factors (age, ability to swallow, clinical status).
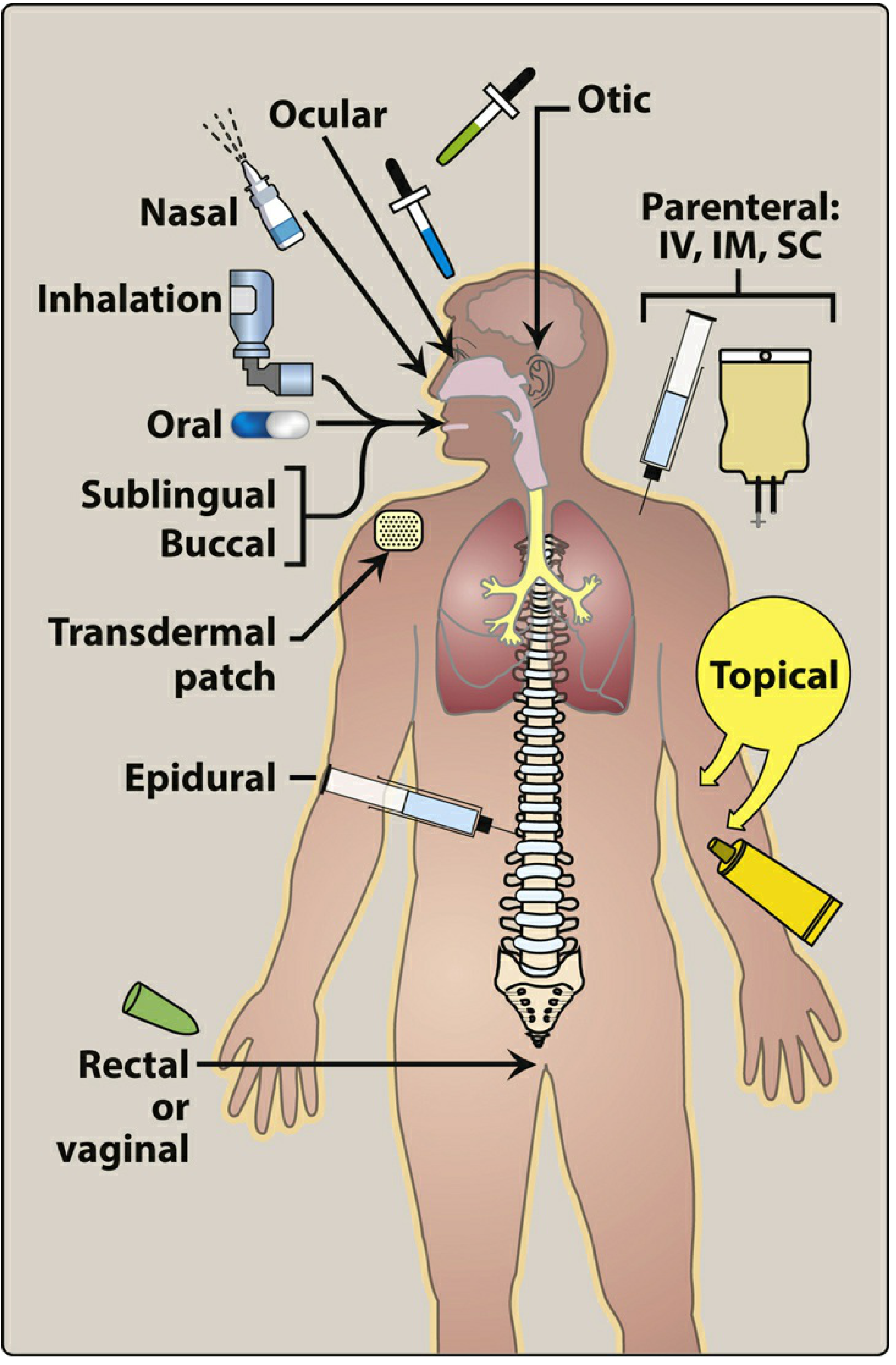
Figure: Commonly used routes of drug administration (Lippincott Illustrated Reviews: Pharmacology)
Classification of Dosage Forms by Route
1. Enteral (GI Tract) Dosage Forms
Enteral administration is the most common, convenient, and economical method. The drug may be swallowed (oral), placed under the tongue (sublingual), or placed between the gums and cheek (buccal).
A. Oral Solid Dosage Forms
| Form | Description |
|---|---|
| Uncoated tablets | Compressed solid, simplest form |
| Film-coated tablets | Thin polymer coating for taste masking and protection |
| Sugar-coated tablets | Outer sugar layer for palatability |
| Enteric-coated tablets | Chemical envelope resists stomach acid; dissolves in the intestine. Used for acid-labile drugs (e.g., omeprazole) or GI-irritating drugs (e.g., aspirin) |
| Chewable tablets | Designed to be chewed; useful in children and elderly |
| Dispersible tablets | Dissolve in water before administration; useful for paediatric/geriatric patients |
| Crushable tablets | Can be crushed for nasogastric tube administration |
| Hard gelatin capsules | Drug powder or granules enclosed in a gelatin shell |
| Soft gelatin capsules | Liquid or semi-solid drug enclosed in a one-piece gelatin shell |
| Sachets | Unit-dose powder packets dissolved in liquid before use |
B. Extended-Release (ER) Oral Preparations
Abbreviated as ER, XR, XL, SR, CR - these use special coatings or matrix systems to slow drug release and prolong the duration of action. Key advantages:
- Less frequent dosing (improves adherence)
- More stable plasma concentrations within the therapeutic range (fewer peaks and troughs)
- Particularly beneficial for drugs with short half-lives - e.g., oral morphine (t½ 2-4 h) needs 6 doses/day as immediate-release vs. only 2 doses/day as extended-release
"ER formulations may maintain concentrations within the therapeutic range over a longer duration, as opposed to immediate-release dosage forms, which may result in larger peaks and troughs in plasma concentration." - Lippincott Illustrated Reviews: Pharmacology
C. Oral Liquid Dosage Forms
- Syrups - aqueous solutions containing sugar; preferred in children
- Suspensions - drug particles dispersed (not dissolved) in a liquid vehicle; must be shaken before use
- Elixirs - clear, sweetened hydroalcoholic solutions
D. Sublingual and Buccal Forms
- Sublingual tablets - placed under the tongue; drug absorbed directly into systemic veins, bypassing first-pass hepatic metabolism (e.g., nitroglycerin, buprenorphine)
- Buccal tablets/films - placed between cheek and gum
Both routes offer: rapid absorption, bypass of the harsh GI environment, and avoidance of first-pass metabolism.
E. Rectal Forms
- Suppositories - solid forms that melt or dissolve at rectal temperature
- Enemas (e.g., hydrocortisone enemas for ulcerative colitis)
- Partially avoid first-pass effect (lower rectal veins drain into the inferior vena cava, not the portal vein)
2. Parenteral Dosage Forms
Parenteral administration introduces drugs directly into the systemic circulation. Used when:
- Drug is poorly absorbed or unstable in the GI tract (e.g., heparin, insulin)
- Patient is unconscious or unable to take oral drugs
- Rapid onset is needed
Disadvantage: Irreversible, may cause pain, local tissue damage, or infection.
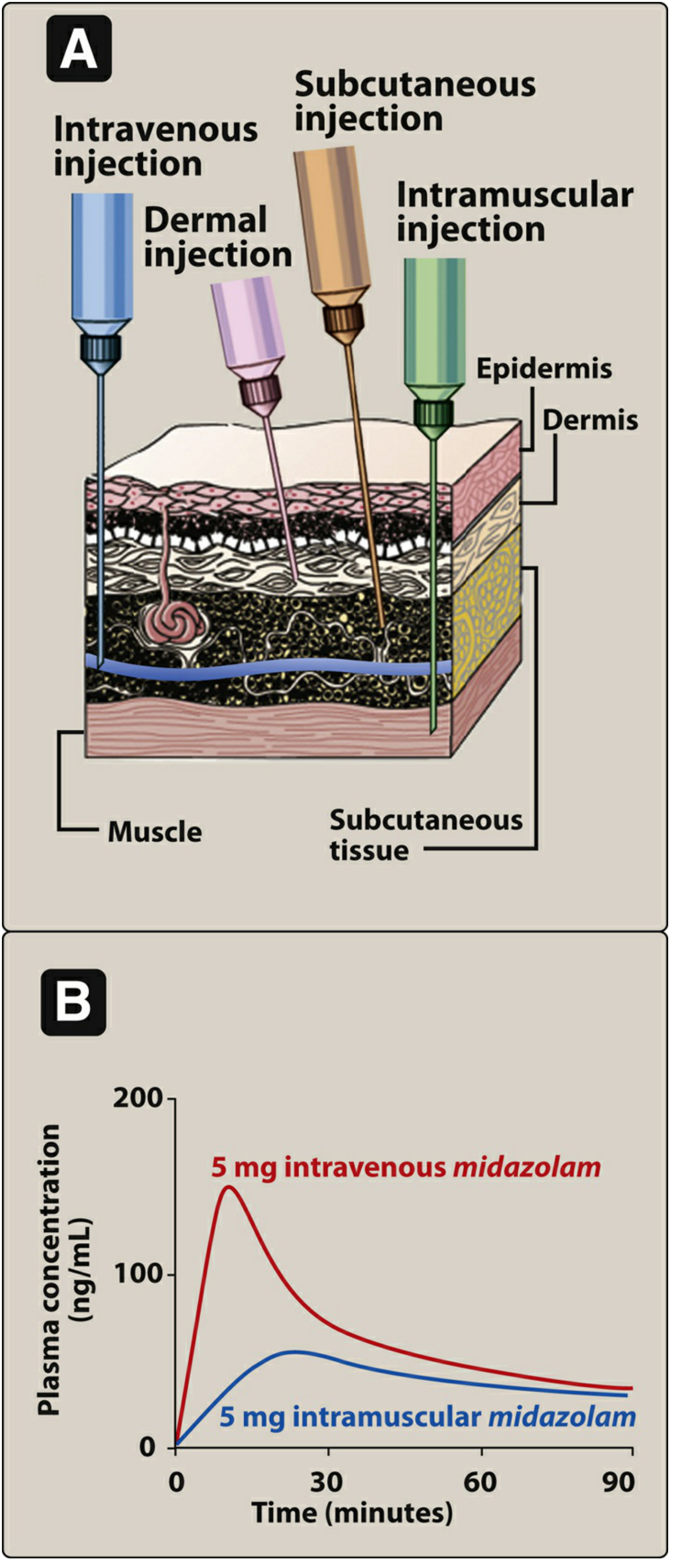
Figure: Schematic of injection routes and comparative plasma concentrations after IV vs IM midazolam (Lippincott Illustrated Reviews: Pharmacology)
| Route | Characteristics |
|---|---|
| Intravenous (IV) | Most common parenteral route. Bolus = immediate peak; infusion = lower, sustained levels. Maximum control over delivered dose. No absorption step - 100% bioavailability |
| Intramuscular (IM) | Aqueous solutions absorbed rapidly; depot preparations (in oil or polyethylene glycol) absorbed slowly over days-weeks (e.g., depot antipsychotics) |
| Subcutaneous (SC) | Slower than IV; constant, sustained absorption via simple diffusion. Avoid with irritant drugs |
| Intradermal (ID) | Into the dermis; used for allergy testing, desensitization, tuberculin test, vaccines |
| Intra-articular | Directly into joint space; e.g., corticosteroid injections for joint disease |
| Intrathecal / Intraventricular | Into CSF; used to bypass the blood-brain barrier for CNS-directed therapy |
| Epidural | Into the epidural space; used for regional anaesthesia and analgesia |
Depot preparations (IM): Consist of drug suspended in a non-aqueous vehicle (oil or polyethylene glycol). The vehicle diffuses out of muscle, drug precipitates at the injection site, then dissolves slowly - providing sustained dosing over weeks to months.
3. Inhalation and Nasal Dosage Forms
Drugs delivered via the respiratory tract reach a large mucosal surface area, producing rapid absorption nearly as fast as IV bolus. Drug effects are almost immediate.
- Metered-dose inhalers (MDIs)
- Dry powder inhalers (DPIs) - breath-activated; do NOT use with a spacer
- Nebulizers - convert liquid drug to aerosol mist
- Nasal sprays - topical delivery for local effect (e.g., intranasal corticosteroids for allergic rhinitis)
- Gas inhalation - e.g., anaesthetic agents (halothane, isoflurane, nitrous oxide, sevoflurane), oxygen
Advantages of inhaled route:
- Drug delivered directly to the site of action (lungs)
- Lower doses needed compared to oral or parenteral
- Fewer systemic side effects
4. Topical and Transdermal Dosage Forms
| Form | Description |
|---|---|
| Ointments | Semi-solid, oil-based; good skin penetration; occlusive |
| Creams | Oil-in-water or water-in-oil emulsions; less occlusive than ointments |
| Lotions | Liquid preparations; for large or hairy areas |
| Gels | Clear, semi-solid; absorb quickly |
| Drops | Ophthalmic (eye) or otic (ear) drops |
| Transdermal patches | Systemic delivery through skin; rate of absorption varies with skin characteristics and lipid solubility of the drug. Avoids first-pass metabolism. Examples: nitroglycerin, fentanyl, nicotine, estrogen patches |
"The transdermal route offers the same [first-pass bypassing] advantage [as sublingual]. There are several reasons for different routes: for convenience (oral), to maximize concentration at site of action (topical), to prolong absorption (transdermal), or to avoid first-pass effect (sublingual or rectal)." - Katzung's Basic and Clinical Pharmacology, 16th ed.
5. Other / Specialized Dosage Forms
| Form | Details |
|---|---|
| Ocular (ophthalmic) | Drops, ointments, gels applied directly to the eye |
| Otic | Drops instilled into the ear canal |
| Vaginal | Tablets, creams, rings, suppositories |
| Liposomal / Lipid complex preparations | Drug encapsulated in lipid vesicles; modified biodistribution and reduced toxicity (e.g., liposomal amphotericin B) |
| Powder for injection | Reconstituted with solvent before administration (e.g., thiopentone powder) |
Summary Table: Key Considerations for Dosage Form Selection
| Factor | Preferred Form |
|---|---|
| First-pass avoidance | Sublingual, transdermal, IV, rectal |
| Rapid onset needed | IV, sublingual, inhalation |
| Prolonged action | Extended-release oral, depot IM, transdermal |
| GI-irritating drug | Enteric-coated tablet |
| Acid-labile drug | Enteric-coated or IV |
| Patient cannot swallow | Parenteral, rectal, transdermal, sublingual |
| Local action in lung | Inhalation |
| Paediatric / elderly | Liquid, chewable, dispersible tablets |
Sources:
- Lippincott Illustrated Reviews: Pharmacology - Routes of Drug Administration, pp. 22-28
- Katzung's Basic and Clinical Pharmacology, 16th ed. - Alternative Routes of Administration & the First-Pass Effect, p. 82-83; Special Dosage Forms
- Park's Textbook of Preventive and Social Medicine - Dosage Forms/Formulations of a Medicine, p. 547
This is a shared conversation. Sign in to Orris to start your own chat.