Dengue management with current guide lines
Reading File
Finding Sources
Searching PubMed
"dengue" AND "management" AND "guidelines"
Searching the Web
WHO dengue management guidelines 2024 2025
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading Web Page
https://www.who.int/news/item/10-07-2025-new-who-guidelines-…
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive data from multiple authoritative sources. Let me compile the full, detailed response.
Dengue Management - Current Guidelines (2025-2026)
Guideline Update: WHO published its new arboviral disease guidelines on July 10, 2025 - the first global guidelines covering dengue, chikungunya, Zika, and yellow fever together. These are now the most current authoritative recommendations.
1. Overview and Epidemiology
Dengue is caused by four serotypes (DENV-1 to DENV-4) of the Flavivirus family, transmitted by Aedes aegypti (primary) and Aedes albopictus (secondary). Over 390 million infections occur annually; in 2024, WHO recorded over 14.4 million cases - unprecedented levels. As of early 2025, over 4 million cases and 3,000+ deaths were reported from 97 countries. About 40-80% of infections are asymptomatic; 1-5% of symptomatic cases progress to severe dengue.
Pathogenesis key point: Secondary infection with a different serotype dramatically increases the risk of severe dengue via antibody-dependent enhancement (ADE) - pre-existing non-neutralizing antibodies potentiate viral entry. - Goldman-Cecil Medicine, p. 3657
2. Clinical Classification (WHO 2009 - Still Standard)
Three-tier Classification
| Category | Criteria |
|---|---|
| Dengue without warning signs | Fever + 2 of: nausea/vomiting, rash, aches/pains, leukopenia, positive tourniquet test |
| Dengue WITH warning signs | Above + any of: abdominal pain/tenderness, persistent vomiting, clinical fluid accumulation (ascites/pleural effusion), mucosal bleeding, lethargy/restlessness, liver enlargement >2 cm, rapid decline in platelets |
| Severe dengue | Severe plasma leakage → shock or respiratory distress; severe bleeding; severe organ involvement (AST/ALT ≥1000 IU/L, impaired consciousness, cardiac/organ failure) |
Classic DHF Grading (WHO)
| Grade | Features | Labs |
|---|---|---|
| I (DHF) | DF criteria + haemorrhagic manifestation + positive tourniquet test | Platelets <100,000; Hct rise ≥20% |
| II (DHF) | Grade I + spontaneous bleeding (skin, GI, epistaxis) | Platelets <100,000; Hct rise ≥20% |
| III (DSS) | Grade II + circulatory failure (weak rapid pulse, pulse pressure ≤20 mmHg, hypotension, cold clammy skin, restlessness) | Platelets <100,000; Hct rise >20% |
| IV (DSS) | Grade III + profound shock with undetectable BP/pulse | Platelets <100,000; Hct rise >20% |
- Park's Textbook of Preventive & Social Medicine, p. 295
Disease Phases
- Febrile phase (days 1-3): High fever, headache, retro-orbital pain, myalgia/arthralgia, facial erythema, maculopapular rash, leukopenia, petechiae
- Critical phase (days 3-7, around defervescence): Plasma leakage lasting 24-48 hours - risk of pleural effusion, ascites, hypovolemic shock, hemorrhage. Rising hematocrit = warning
- Recovery/Convalescent phase: Reabsorption of extravascular fluid, watch for fluid overload (hematocrit falls due to dilution)
3. Diagnosis
Diagnostic Tests - Time-Based Selection
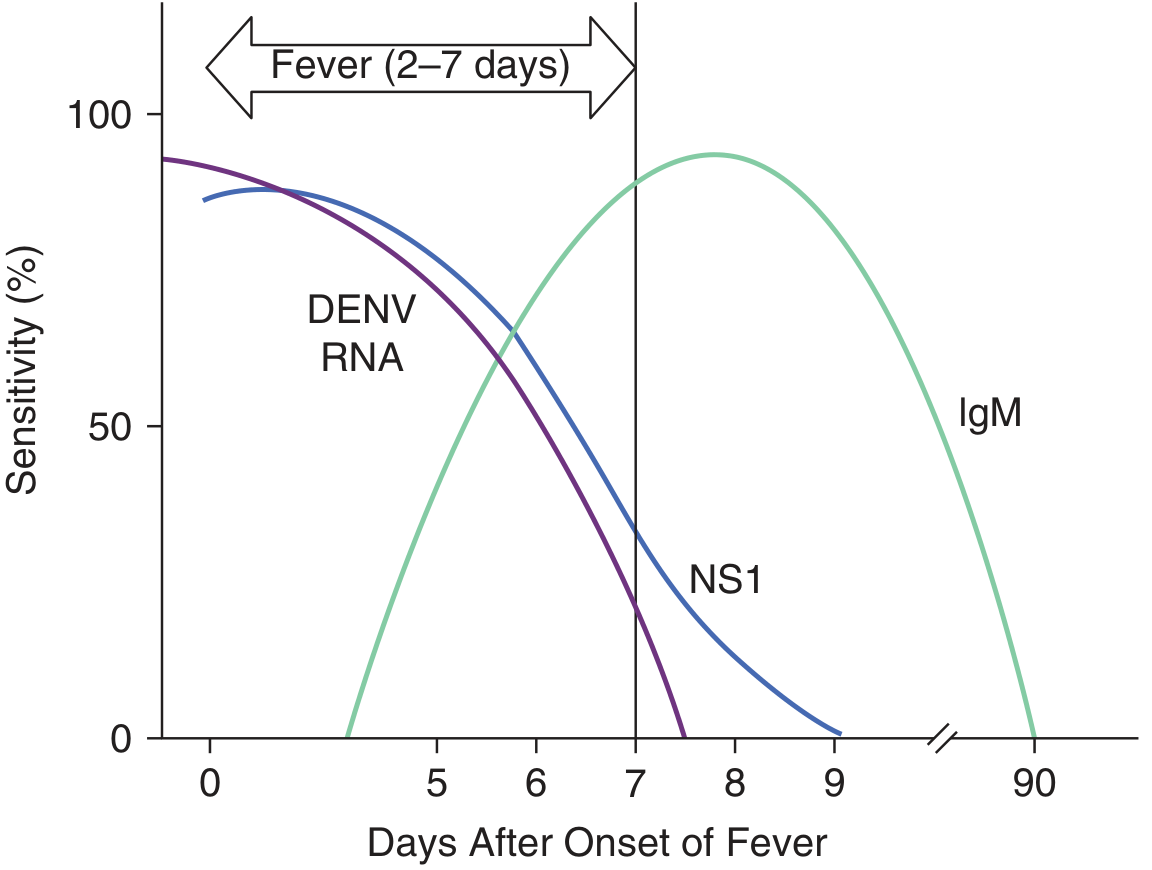
As shown above, DENV RNA (RT-PCR) and NS1 antigen are best in the first 7 days; IgM rises after day 4-5 and peaks at ~2 weeks.
| Test | Optimal Timing | Notes |
|---|---|---|
| RT-PCR (DENV RNA) | Days 1-7 | Most specific; ~90% sensitivity early |
| NS1 antigen ELISA/RDT | Days 1-6 | Rapid, commercially available; does not differentiate serotypes |
| IgM (MAC-ELISA) | Day 3 onwards; 99% positive by day 10 | Can cross-react with Zika, other flaviviruses |
| IgG (paired sera) | ≥4-fold rise between acute and convalescent (>15 days) | Confirms recent infection |
| Combined NS1 + IgM | Days 1-10 | Identifies ≥90% of primary and secondary cases |
Key CBC findings: Leukopenia, thrombocytopenia, rising hematocrit (hemoconcentration), elevated transaminases. In DHF: coagulopathy may be present.
- Red Book 2021, p. 523; Goldman-Cecil Medicine, p. 3657
Differential diagnosis: Malaria, chikungunya, Zika, leptospirosis, rickettsial infections, other viral hemorrhagic fevers (Ebola, Marburg, yellow fever), measles.
4. Management
Core Principle: No specific antiviral therapy exists. Management is entirely supportive, stratified by disease severity.
A. Dengue Fever (Without Warning Signs) - Outpatient
- Oral hydration: ORS, fruit juices, electrolyte-rich fluids to replace losses from fever and vomiting. Goal: urine output at least once every 6 hours
- Antipyretics: Paracetamol (acetaminophen) only; dose interval should not be less than 6 hours; tepid sponging for high fever
- STRICTLY AVOID: Aspirin (risk of Reye's syndrome and bleeding), NSAIDs (ibuprofen - aggravate gastritis and bleeding tendency), steroids
- Monitoring: Daily clinical review; serial hematocrit and platelet counts from day 3
- Return to hospital immediately if: no improvement, deterioration around defervescence, severe abdominal pain, persistent vomiting, cold clammy extremities, lethargy, any bleeding (black stools, coffee-ground vomitus), no urine output for >4-6 hours
- Park's Textbook, p. 294; Red Book 2021, p. 524
B. Dengue WITH Warning Signs or DHF Grades I-II - Hospitalize
- IV fluid therapy if unable to tolerate oral fluids or persistent vomiting
- Use isotonic crystalloids (normal saline, Ringer's lactate) as first-line IV fluid
- Serial hematocrit monitoring: Rising Hct indicates plasma leakage; guide fluid rate accordingly. If Hct rises ≥20% from baseline = significant leakage
- Platelet monitoring: Serial counts every 6-12 hours during critical phase
- Watch for: early shock, occult bleeding, fluid overload, electrolyte disturbances
- Paracetamol continues for fever; temperature target <39°C
- Urine output monitoring: Target >0.5 mL/kg/hr
C. Severe Dengue - DHF Grades III/IV (DSS) - ICU Level Care
- Fluid resuscitation: Immediate crystalloid bolus (10-20 mL/kg over 15-30 minutes in children; guided by clinical status in adults). Reassess frequently.
- Colloids (e.g., dextran, HES) if refractory shock after initial crystalloid trial
- Blood products: For significant hemorrhage or refractory shock; packed red cells if active bleeding with low Hb; platelet transfusions for active bleeding with severe thrombocytopenia (not prophylactic at any specific count)
- Oxygen supplementation as indicated
- Organ support as required (renal replacement, mechanical ventilation if respiratory failure)
- Avoid fluid overload: With recovery/reabsorption of leaked fluid, reduce IV fluids promptly; diuretics may be required if overloaded with adequate hemodynamics
- Steroids: Current evidence is inconclusive and insufficient to recommend - do NOT use routinely
- Platelet transfusions: Only for active significant bleeding; prophylactic transfusions are not recommended even with very low platelet counts in the absence of bleeding
Early recognition and aggressive supportive care reduces case fatality rate (CFR) from 5-10% to <1%. - Red Book 2021, p. 524; Goldman-Cecil, p. 3658
Fluid Management Algorithm Principles (Park's / WHO)
Patient with suspected severe dengue (Grade III/IV):
│
├─ Give crystalloid bolus (10-20 mL/kg over 15-30 min)
│
├─ Response? ──YES──► Slow to maintenance; monitor closely
│
└─ No response after 2 boluses?
├─ Check hematocrit
│ ├─ Rising Hct → Add colloid
│ └─ Falling Hct → Suspect bleeding → Blood/blood products
└─ Monitor for fluid overload continuously
D. Disposition Summary
| Severity | Setting |
|---|---|
| Dengue fever, no warning signs, tolerating oral fluids | Outpatient with daily follow-up |
| Warning signs, mild DHF (Grade I-II), poor oral intake | Hospital ward |
| DHF Grade III-IV (DSS), severe bleeding, organ failure | ICU |
5. Special Populations
Pregnancy
- Vertical transmission rate ~20% (higher near delivery)
- Supportive treatment (hydration + paracetamol); avoid NSAIDs
- Close fetal monitoring; severe dengue in pregnancy associated with preterm labor and adverse perinatal outcomes
- Creasy & Resnik's Maternal-Fetal Medicine
Children (Pediatric)
- Higher risk of severe disease and DSS
- Weight-based fluid calculations essential
- WHO paediatric drug optimization for dengue meeting held Oct 2025 - see WHO PADO report
6. Vaccines
| Vaccine | Details |
|---|---|
| Dengvaxia (CYD-TDV) | Recombinant live attenuated tetravalent vaccine; 3 doses (0, 6, 12 months); approved for ages 9-45 years; only for seropositive individuals - seronegative recipients have increased risk of severe dengue upon natural infection |
| Qdenga (TAK-003) | Quadrivalent live attenuated; ~80% efficacy against infection in children 4-16 years; 90% protection against hospitalization |
| Wolbachia | Infecting Aedes aegypti with Wolbachia pipientis reduces dengue infection in endemic areas by ~75% |
Key safety note on Dengvaxia: Pre-vaccination dengue serology testing is required. In dengue-naive individuals, the vaccine acts like a primary infection, increasing severe disease risk with subsequent natural infection.
- Goldman-Cecil Medicine, p. 3658
7. Isolation and Infection Control
- Standard precautions in hospital; attention to bloodborne transmission risk
- Prevent secondary transmission: control Aedes mosquitoes around infected patients
- Patient should use mosquito nets/repellent to prevent mosquito feeding during viremic phase (days 1-5 of fever)
8. Monitoring Parameters During Hospitalization
| Parameter | Frequency | Action Threshold |
|---|---|---|
| Temperature | Every 4-6 hours | Paracetamol if >38.5°C |
| Hematocrit | Every 6-12 hours | Rise ≥20% = IV fluids |
| Platelet count | Daily (or more if falling) | Active bleeding = transfuse |
| BP, pulse, CRT | Every 1-4 hours (critical phase) | Narrow pulse pressure = early shock |
| Urine output | Hourly (severe cases) | <0.5 mL/kg/hr = adjust fluids |
| Fluid balance | Continuous | Positive balance in recovery = diuretics |
Summary of Key "Do's and Don'ts"
| ✅ DO | ❌ DO NOT |
|---|---|
| Paracetamol for fever | Aspirin / NSAIDs / Ibuprofen |
| Oral hydration (ORS, juices) | Prophylactic platelet transfusions |
| Serial Hct and platelet monitoring | Steroids (no proven benefit) |
| Crystalloids first for shock | Aggressive fluids in convalescent phase |
| ICU for DSS / severe dengue | Delay recognition of warning signs |
| Blood products for active bleeding | Antibiotics (unless secondary bacterial infection) |
Sources:
- Red Book 2021: Report of the Committee on Infectious Diseases, pp. 520-524
- Park's Textbook of Preventive and Social Medicine, pp. 293-297
- Goldman-Cecil Medicine (International Edition), pp. 3656-3659
- Rosen's Emergency Medicine, pp. 2629-2631
- Harrison's Principles of Internal Medicine, 22nd Ed. (2025)
- WHO Guidelines for Clinical Management of Arboviral Diseases: Dengue, Chikungunya, Zika and Yellow Fever (Published July 10, 2025)
This is a shared conversation. Sign in to Orris to start your own chat.