Cerebellum pathologies
Reading File
Finding Sources
Finding Sources
Searching PubMed
cerebellum pathology ataxia
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Now I have enough material for a comprehensive answer. Let me compile it.
Cerebellum Pathologies
Anatomy & Functional Zones (Brief Recap)
The cerebellum is organized into three functional zones, each with distinct clinical implications when damaged:
| Zone | Input/Function | Lesion Effects |
|---|---|---|
| Vestibulocerebellum (flocculonodular lobe) | Balance, vestibulo-ocular reflex | Truncal ataxia, gait instability, nystagmus |
| Spinocerebellum (vermis + intermediate hemisphere) | Limb coordination, posture | Gait ataxia, ipsilateral limb dysmetria |
| Cerebrocerebellum (lateral hemispheres) | Planning & timing of voluntary movement | Appendicular ataxia, intention tremor, dysarthria |
I. Clinical Features of Cerebellar Disease
From Adams and Victor's Principles of Neurology (12th ed.), cerebellar lesions produce a recognizable constellation:
- Ataxia - incoordination of volitional movement; decomposition of smooth sequences into irregular, jerky components ("decomposition of movement" per Holmes)
- Intention tremor - side-to-side oscillation as the limb approaches a target (also called ataxic tremor)
- Dysmetria - undershooting or overshooting a target; failure of the normal ballistic agonist-antagonist-agonist triphasic sequence
- Dysdiadochokinesis - impaired rapid alternating movements (adiadochokinesis, per Babinski)
- Dysarthria - scanning/staccato speech from incoordination of articulation muscles
- Gait and equilibrium disorders - wide-based, truncal instability
- Hypotonia - particularly with acute cerebellar lesions
- Nystagmus - impaired ocular pursuit, inaccurate saccades
Lesions of one cerebellar hemisphere cause ipsilateral ataxia (due to double-crossing of pathways). Cognitive effects - including frontal-type dysexecutive syndrome - can occur with cerebellar disease ("cerebellar cognitive affective syndrome").
II. Vascular Pathologies
Cerebellar Hemorrhage
(Plum and Posner's Diagnosis and Treatment of Stupor and Coma)
About 10% of intraparenchymal hemorrhages occur in the cerebellum. Classic presentation:
- Sudden occipital headache, nausea/vomiting, vertigo
- Truncal and gait ataxia, dysarthria
- Nystagmus, ipsilateral gaze paralysis
- Ipsilateral facial palsy, contralateral extensor plantar response
Causes: hypertension (~75%), cerebellar angiomas, anticoagulants, amyloid angiopathy in the elderly. Hypertensive hemorrhages arise near the dentate nuclei. The hemorrhage can cause coma by compressing the brainstem - early diagnosis is critical as surgical evacuation can be life-saving; once the patient is comatose, mortality is high despite intervention.
Cerebellar Infarction
Accounts for ~2% of all strokes. Symptoms resemble hemorrhage but progress more slowly (edema over 2-3 days). Key features:
- Acute/subacute vertigo, dizziness, unsteadiness, dull headache
- Nystagmus toward the infarct, ipsilateral dysmetria
- Risk factors: hypertension, atrial fibrillation, hypercholesterolemia; vertebral artery dissection in younger patients
A mass effect from edema can compress the brainstem and fourth ventricle, requiring urgent surgical decompression. From the admission data of 293 patients: vertigo/dizziness (70%), limb ataxia (59%), truncal ataxia (45%), dysarthria (42%), nystagmus (38%).
III. Tumors
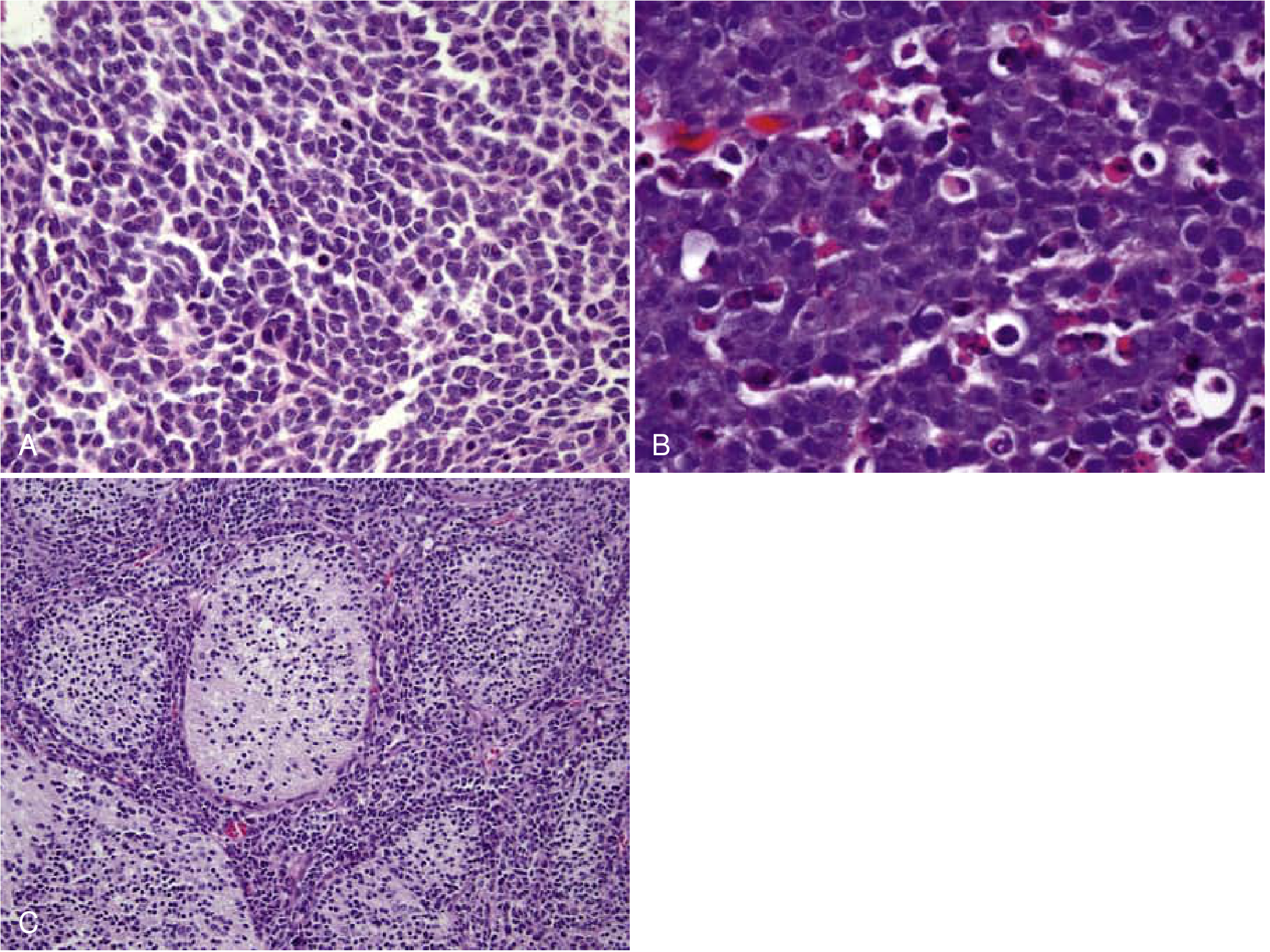
Medulloblastoma (WHO Grade IV)
(Bradley and Daroff's Neurology in Clinical Practice)
- Most common malignant brain tumor in children (>50% under age 10); second peak at 18-25 years
- Arises from external granular layer or subependymal matrix cells of the fourth ventricle
- Small immature cells with hyperchromatic nuclei, numerous mitoses, Homer Wright rosettes
- High propensity to invade the fourth ventricle and disseminate along CSF pathways
- 5-year survival: 70-80% with current treatment
Molecular subgroups (WHO 2016):
- WNT-activated (best prognosis; CTNNB1 mutations)
- SHH-activated (linked to Gorlin syndrome / PTCH mutations on 9q)
- Group 3 and Group 4 (less favorable)
Histological variants: classic, anaplastic/large-cell (worst prognosis), desmoplastic/nodular (better prognosis, associated with Gorlin syndrome in lateral hemispheres).
Hemangioblastoma (WHO Grade I)
(Bradley and Daroff's Neurology in Clinical Practice)
- Most common primary cerebellar neoplasm in adults
- Benign vascular tumor; peak frequency at age 40; more common in males
- Classic appearance: cyst with an enhancing mural nodule
- Rich vascular supply (dark red) - predisposes to spontaneous hemorrhage
- ~10% associated with von Hippel-Lindau (VHL) disease (VHL gene at 3p25-26)
- Histology: abundant capillaries + foamy lipid-laden stromal cells (stain with inhibin, S100, brachyury)
- Can also occur in retina, brainstem, spinal cord (especially in VHL)
IV. Degenerative / Hereditary Diseases
Friedreich's Ataxia
The most common autosomal recessive cerebellar ataxia. Caused by GAA trinucleotide repeat expansion in the frataxin gene on chromosome 9. Features include:
- Progressive cerebellar ataxia (gait onset, then limbs)
- Absent tendon reflexes, positive Babinski sign
- Loss of proprioception and vibration sense (dorsal column involvement)
- Dysarthria, nystagmus
- Cardiomyopathy (major cause of death), kyphoscoliosis, pes cavus
Spinocerebellar Ataxias (SCAs)
A family of autosomal dominant disorders caused by various genetic mutations (most commonly CAG/polyglutamine repeat expansions). Over 40 types identified. Shared features: progressive cerebellar ataxia, often with variable brainstem, spinal cord, and extrapyramidal involvement. SCA3 (Machado-Joseph disease) is the most common worldwide.
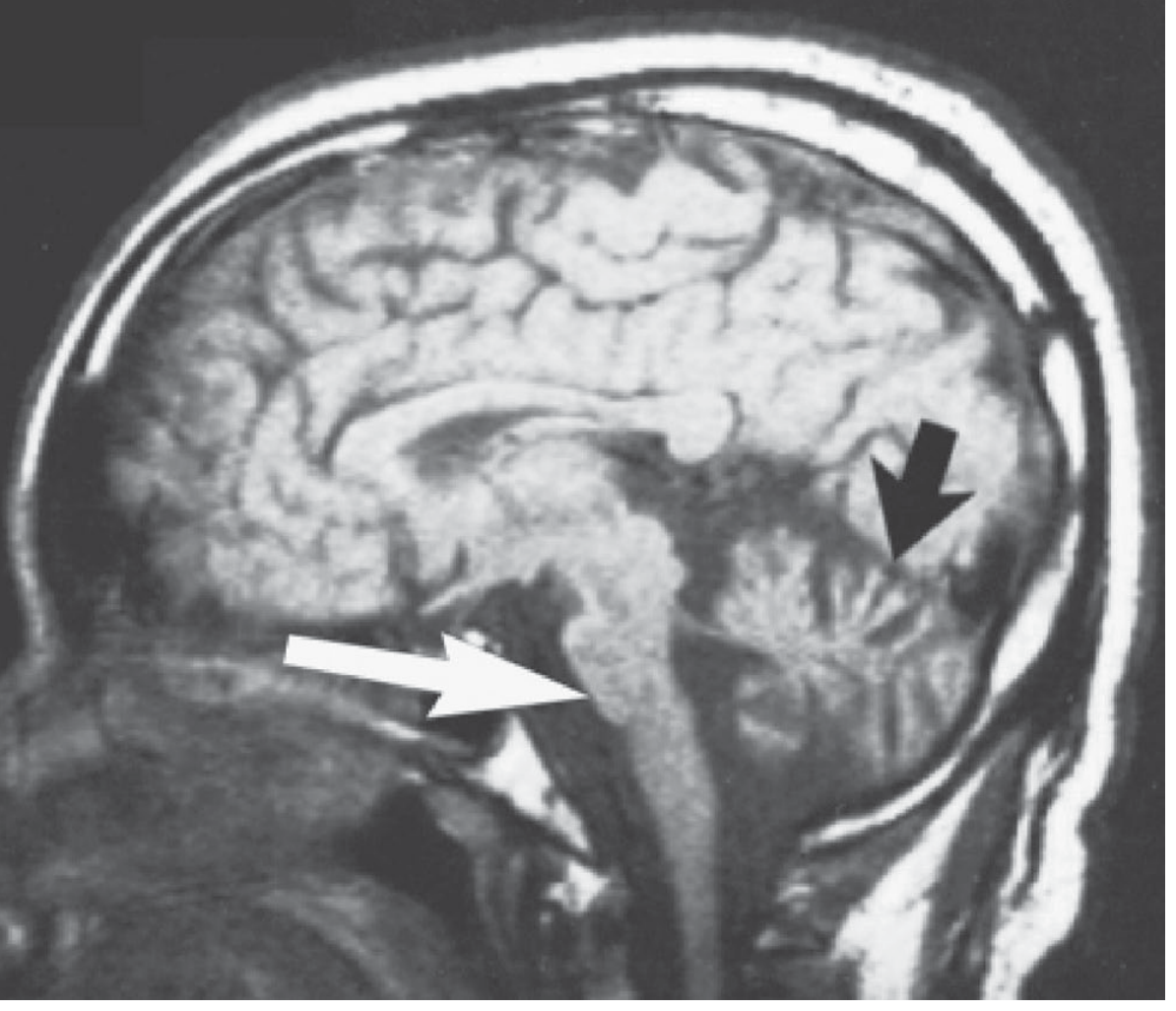
Multiple System Atrophy - Cerebellar type (MSA-C)
(Adams and Victor's Principles of Neurology, formerly olivopontocerebellar atrophy / OPCA)
- Sporadic, progressive; mean age of onset ~6th decade
- Degeneration of pontocerebellar and olivocerebellar fibers, middle cerebellar peduncles, cerebellar white matter
- Loss of Purkinje cells variable
- MRI: vermian atrophy + smallness of the pons ("hot cross bun" sign)
- Autonomic failure (urinary dysfunction, erectile dysfunction) and REM sleep behavior disorder are prominent
- Often associated with extrapyramidal features (parkinsonism)
Alcoholic Cerebellar Degeneration
(Adams and Victor's Principles of Neurology)
- Pathologically related to Wernicke's disease (thiamine deficiency); predominantly anterior vermis degeneration
- Clinically dominated by gait ataxia; arm ataxia is less prominent
- Characteristic that limb tremor is less marked than in paraneoplastic or familial types
- Progresses with continued alcohol use; partial improvement with thiamine and abstinence
V. Paraneoplastic Cerebellar Degeneration (PCD)
(Adams and Victor's Principles of Neurology; Bradley and Daroff's Neurology)
One of the most characteristic paraneoplastic syndromes.
Associated tumors:
- Small cell lung carcinoma (SCLC) - ~1/3 of cases
- Ovarian carcinoma - ~25%
- Hodgkin lymphoma - ~15%
- Breast, bowel, uterine carcinomas
Key antibodies:
| Antibody | Associated Cancer |
|---|---|
| Anti-Yo (PCA-1) | Breast, gynecological |
| Anti-Hu | SCLC (with PEM) |
| Anti-VGCC | SCLC (also with Lambert-Eaton) |
| Anti-Tr (anti-DNER) | Hodgkin lymphoma |
| Sox1 | SCLC (~50% of PCD cases) |
| Anti-Ki | Breast, gynecological, SCLC |
Clinical features:
- Subacute onset (weeks-months) of symmetric pancerebellar dysfunction - gait and limb ataxia, dysarthria, nystagmus
- In >50% of cases, cerebellar signs precede tumor diagnosis
- May also have vertigo, diplopia, Babinski signs, sensorineural hearing loss, cognitive changes
- CSF: mild pleocytosis, elevated protein possible
- FDG-PET shows cerebellar hypometabolism before MRI changes
Prognosis: Poor due to irreversible Purkinje cell loss; most patients do not improve with immunotherapy (IVIG, plasma exchange, rituximab, corticosteroids). Early tumor treatment is paramount.
VI. Other Notable Cerebellar Pathologies
| Condition | Key Features |
|---|---|
| Cerebellar abscess | Usually from otogenic/sinogenic source or hematogenous spread; subacute fever + cerebellar signs + raised ICP |
| Multiple sclerosis | Demyelinating plaques in cerebellar peduncles or white matter; intention tremor, INO, ataxia; relapsing-remitting course |
| Cerebellar hypoplasia | Congenital underdevelopment; may be isolated or part of syndromes (Dandy-Walker, Joubert syndrome) |
| Cerebellar abscess | Post-infectious or direct extension; urgently requires drainage |
| Anti-GAD ataxia | Autoimmune; associated with anti-GAD65 antibodies; downbeat nystagmus prominent |
| Celiac-related ataxia (gluten ataxia) | Subacute cerebellar syndrome associated with anti-gliadin/anti-transglutaminase antibodies; responds to gluten-free diet |
| Hypothyroidism | Reversible cerebellar ataxia; slow movements, gait unsteadiness |
| Drug/toxin-induced | Phenytoin, carbamazepine, lithium, alcohol, heavy metals; often reversible |
VII. Differential Diagnosis Summary
Cerebellar ataxia must be distinguished from:
- Sensory ataxia (posterior column/large fiber neuropathy) - worsened by eye closure, Romberg positive, proprioception lost, no dysarthria/nystagmus
- Vestibular ataxia - rotatory nystagmus, past-pointing toward one side
- Frontal lobe ataxia - gait apraxia, cognitive features prominent
- Miller Fisher syndrome - post-infectious; ataxia + ophthalmoplegia + areflexia (anti-GQ1b)
Sources: Adams and Victor's Principles of Neurology (12th ed.) | Bradley and Daroff's Neurology in Clinical Practice | Plum and Posner's Diagnosis and Treatment of Stupor and Coma | Robbins & Kumar Basic Pathology | Harrison's Principles of Internal Medicine (22nd ed., 2025)
This is a shared conversation. Sign in to Orris to start your own chat.