Acl surgery and grafting with physiotherapy rehabilitation
Reading File
Finding Sources
Finding Sources
Searching PubMed
"anterior cruciate ligament" AND "reconstruction" AND "rehabilitation"
Searching the Web
ACL surgery graft types rehabilitation physiotherapy protocol 2024 2025
Finding Sources
Finding Sources
Reading Web Page
ACL graft types surgery rehabilitation physiotherapy protocol phases
Reading File
Reading File
Finding Sources
Searching Images
ACL anterior cruciate ligament reconstruction graft surgery
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Loading Image
Here is a comprehensive, evidence-based overview of ACL surgery, grafting, and physiotherapy rehabilitation.
ACL Surgery, Graft Selection & Physiotherapy Rehabilitation
1. ACL Anatomy & Biomechanics
The ACL consists of two distinct fiber bundles:
- Anteromedial (AM) bundle — taut in flexion; primary restraint to anterior tibial translation
- Posterolateral (PL) bundle — taut in extension; contributes to rotational stability
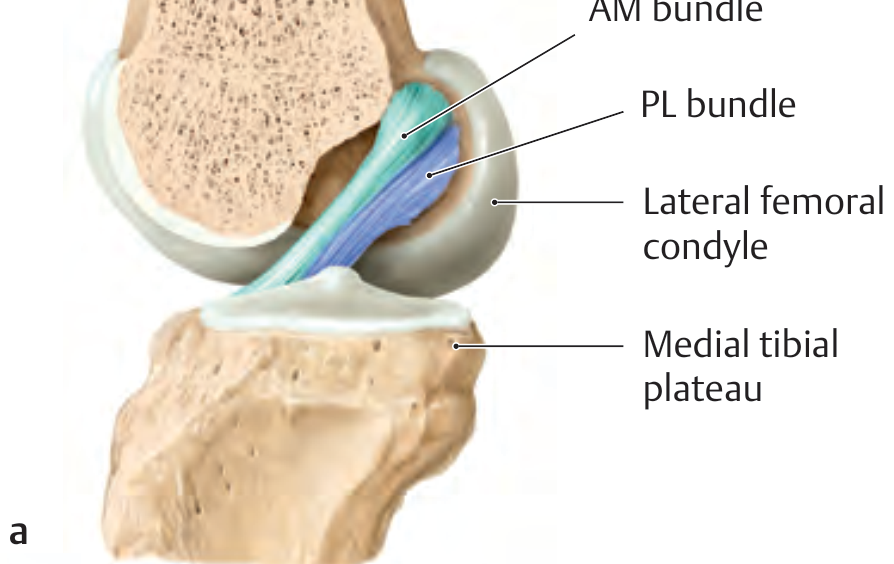
The most common injury mechanism is a non-contact valgus collapse with a flexed, externally-rotated knee (sudden change of direction). ACL ruptures represent ~20% of all knee injuries; 70% occur between ages 15–45, with women affected significantly more often than men. The classic "unhappy triad" combines ACL rupture with medial collateral ligament (MCL) and medial meniscus tears.
- General Anatomy and Musculoskeletal System (THIEME Atlas), p. 473
2. Indications for Surgery
Surgery is generally indicated for:
- Young/active patients with functional instability
- Concomitant meniscal or chondral injuries requiring repair
- High-demand athletes or those in pivoting sports
- Failure of conservative management
Key principle: Full range of motion (ROM) and good quadriceps control should be achieved prior to surgery to minimize arthrofibrosis risk.
- Miller's Review of Orthopaedics 9th Ed.
3. Surgical Technique
Modern ACL reconstruction is performed arthroscopically. The key technical principle is anatomic tunnel placement — centering the graft in the native ACL footprint using independent femoral tunnel drilling (rather than transtibial drilling). A more horizontal graft position (10- or 2-o'clock femoral position) reduces rotational instability.
Double-bundle reconstruction replaces both the AM and PL bundles via 4 bony tunnels, restoring both anterior-posterior and rotational stability more anatomically — though clinical superiority over single-bundle reconstruction remains debated.

4. Graft Options
| Graft Type | Key Advantages | Key Disadvantages |
|---|---|---|
| Bone-Patellar Tendon-Bone (BPTB) autograft | Fastest bone tunnel incorporation; "gold standard" for early return to sport | Anterior knee pain, kneeling pain, extension loss, higher arthritis risk at 5–7 yrs |
| 4-strand Hamstring autograft | Similar strength to native ACL; less arthritis risk | Less stiff; donor site: knee flexion weakness, saphenous nerve injury risk |
| Quadriceps tendon autograft | Large graft diameter; growing popularity | Patellar fracture risk (with bone block) |
| Allograft | No donor site morbidity; good for revisions/low-demand patients | Slower incorporation; higher rupture rate in young active patients; infection risk (~1:6 million) |
| Peroneus longus tendon | Minimal donor site morbidity; emerging option | Less established evidence |
| Synthetic grafts | Useful for revision in low-demand patients | Long-term durability concerns |
BPTB is often preferred for athletes seeking rapid return to sport. Hamstring grafts are preferred where anterior knee pain must be avoided. Allografts are avoided in young, high-demand patients due to significantly higher re-rupture rates.
- Miller's Review of Orthopaedics 9th Ed., pp. 350–352
5. Physiotherapy Rehabilitation
Modern rehabilitation is criteria-based rather than purely time-based — progression requires achieving specific functional and strength milestones, not just waiting a set number of weeks (Aspetar Clinical Practice Guideline, 2024/2025).
Phase 1 — Immediate Post-Op (Weeks 0–4)
Goals: Protect graft, control pain/swelling, restore full knee extension, initiate quadriceps activation
Key interventions:
- RICE (rest, ice, compression, elevation)
- Ankle pumps, quad sets, heel slides, straight leg raises (only once quad activation is confirmed — no SLR with extension lag)
- Multi-angle isometrics at 90° and 60°
- Weight-bearing as tolerated with crutches; wean as tolerated
- For hamstring grafts: delay resisted hamstring exercises for 12 weeks
- For BPTB: closed-chain quad exercises (wall sit, leg press 90–30°) tolerated earlier
Progression criteria:
- Knee extension = 0° (full extension without pain)
- Minimal/absent effusion (grade 0–1 stroke test)
- Active quadriceps contraction (SLR without extension lag)
- Tolerance to partial weight-bearing
Phase 2 — Early Strengthening (Weeks 4–12)
Goals: Restore full flexion and normalize gait, begin controlled loading
Key interventions:
- Stationary bicycle, elliptical
- Closed kinetic chain (CKC) exercises: step-ups, mini-squats (0–60°), ball squats, leg press
- Hip abductor/lumbopelvic strengthening: bridges, clamshells, hip hikes
- Proprioception: single-leg balance → dynamic balance → unstable surfaces
- Open kinetic chain (OKC) extension exercises (e.g., terminal knee extensions) should be avoided in the first 6 weeks due to increased graft stress near full extension
Progression criteria:
- Flexion ≥ 120° (within 10° of contralateral side)
- Extension equal to contralateral side
- Quadriceps strength ≥ 60% of contralateral limb
- Uncompensated gait under full weight-bearing
Evidence note: A 2024 systematic review (Pamboris et al., PMID 38887689) found that both CKC and OKC exercises improve pain, function, and quadriceps strength in ACL rehabilitation — OKC exercises introduced after 6 weeks are safe and beneficial.
Phase 3 — Advanced Strengthening & Neuromuscular Control (Weeks 6/12–20)
Goals: Progress strength symmetry, develop sport-specific neuromuscular control
Key interventions:
- Progressive eccentric training (proven to improve quadriceps and gluteus maximus mass/function)
- Running progression (straight-line jogging introduced at 8–12 weeks criteria-permitting)
- Lateral step-overs, perturbation training
- Plyometric progression: bilateral → unilateral jumps, eccentric single-leg hops
- Blood flow restriction (BFR) training — a 2025 meta-analysis (Gopinatth et al., PMID 38889851) demonstrates BFR enhances muscle strength and size recovery post-ACLR
- Limb Symmetry Index (LSI): measured via single-leg hop tests; target ≥ 90% symmetry
Progression criteria:
- Quadriceps strength ≥ 80% of contralateral limb
- Hop test LSI ≥ 90%
- No pain or effusion with progressive loading
- Appropriate landing mechanics and movement quality
Phase 4 — Return to Sport (Week 20+)
Goals: Full sport-specific conditioning, confidence, psychological readiness
Key interventions:
- Sport-specific drills: cutting, pivoting, deceleration
- Reactive agility tasks
- ACL-RSI (psychological readiness scale) assessment
- Gradual return to training → team training → competitive play
Return-to-sport criteria (Aspetar Guideline):
- LSI ≥ 90% on all hop tests
- Isokinetic quadriceps strength ≥ 90% symmetry
- ACL-RSI ≥ 65
- Confirmed movement quality and absence of pain/effusion
Important 2025 finding: A meta-analysis (Filbay et al., PMID 40603829) found no difference in return-to-sport rate or activity level between ACL reconstruction and rehabilitation alone at long-term follow-up, reinforcing that rehabilitation quality — not surgery alone — determines outcomes.
6. Graft-Specific Rehabilitation Nuances
| Graft | Phase 1 Emphasis | Phase 2–3 Caution |
|---|---|---|
| BPTB | Aggressive quad activation; early CKC | Anterior knee pain monitoring; extension work |
| Hamstring | Gentle ROM; quad focus | Avoid resisted hamstring curls for 12 weeks (graft harvest site protection) |
| Quadriceps tendon | Quad activation with care | Monitor for anterior thigh pain/patellar irritation |
| Allograft | Slower biological incorporation → extend each phase | Avoid aggressive early loading; longer timeline to RTS |
7. Complications & Their Rehabilitation Implications
| Complication | Notes |
|---|---|
| Arthrofibrosis | Most common complication; prevented by achieving full ROM before and immediately after surgery |
| Tunnel malposition | Most common technical error leading to graft failure; vertical graft → decreased rotational stability |
| Re-rupture | Risk is reduced by criteria-based (not time-based) return to sport; BFR training and eccentric protocols help |
| Donor site morbidity | BPTB → anterior knee pain; hamstring → flexion weakness; managed with targeted physiotherapy |
8. Key Evidence Summary
| Study | Finding |
|---|---|
| Pamboris et al. 2024 (PMID 38887689) | OKC and CKC both effective; OKC safe after 6 weeks |
| Gopinatth et al. 2025 (PMID 38889851) | Blood flow restriction training significantly enhances post-ACLR recovery |
| Fontanier et al. 2025 (PMID 39985872) | Early OKC in first weeks is safe with some benefit to quad strength |
| Filbay et al. 2025 (PMID 40603829) | Rehab-only ≈ ACLR for return-to-sport rates; rehabilitation quality is paramount |
Bottom line: ACL reconstruction success depends as much on the rehabilitation program as on the surgery itself. Graft selection should be individualized (BPTB for early return to sport in high-demand athletes; hamstring for those where anterior knee pain is a concern; allograft for revision/low-demand). Rehabilitation must be criteria-driven, progressing through phase milestones — not simply calendar-based — with a particular emphasis on quadriceps symmetry, neuromuscular control, and psychological readiness before return to sport.
This is a shared conversation. Sign in to Orris to start your own chat.