CT coronary calcium scoring
Reading File
Finding Sources
Finding Sources
Searching PubMed
"coronary artery calcium" AND scoring
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive data from multiple authoritative textbooks. Let me compile the full answer.
CT Coronary Calcium Scoring (CAC)
What It Is
CT coronary calcium scoring (also called coronary artery calcification scoring, CAC) is the simplest application of cardiac CT and does not require iodinated contrast. It acquires non-contrast axial images through the heart to detect and quantify calcified deposits within the coronary artery walls. Calcium on CT appears as dense, bright-white structures even without contrast - because hydroxyapatite (the main crystal in atherosclerotic calcification) has high x-ray attenuation. The procedure delivers a very low radiation dose (~1-2 mSv). - Harrison's Principles of Internal Medicine 22E, p. 1923
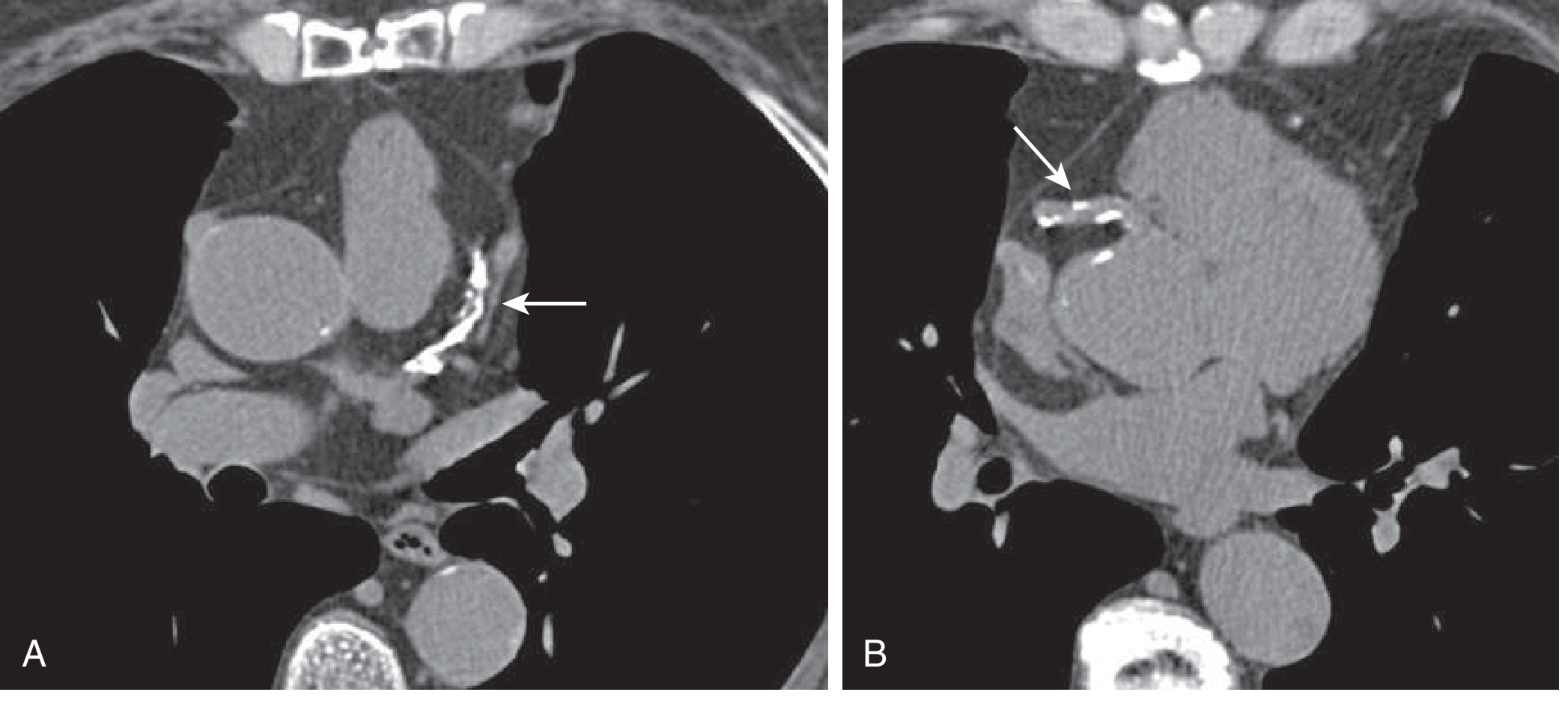
Non-contrast cardiac CT for coronary calcium scoring. A: Proximal LAD with extensive calcification (arrow). B: Proximal RCA with spotty calcification (arrow). Agatston score = 457, placing this patient in a higher risk group regardless of Framingham risk score. - Goldman-Cecil Medicine
The Agatston Score - How It's Calculated
The Agatston score is the standard quantification method. For each calcified lesion:
- The area of each calcified focus (pixels >130 Hounsfield units) is measured
- Multiplied by a density factor based on the peak CT attenuation of that lesion
- All lesions across the entire coronary tree are summed to give the total score
Volume scores and mass scores are less commonly used alternatives. Reference data stratified by age and sex are available, allowing the score to be reported as a percentile. - Grainger & Allison's Diagnostic Radiology; Goldman-Cecil Medicine
Score Categorization
| Agatston Score | Category | Interpretation |
|---|---|---|
| 0 | No calcification | No detectable plaque; excellent prognosis |
| 1-10 | Minimal | Very small calcium burden |
| 10-100 | Mild | Mild atherosclerosis |
| 100-400 | Moderate | Moderate atherosclerotic burden |
| >400 | Severe | Extensive calcification |
- Harrison's Principles of Internal Medicine 22E, p. 1923
What CAC Score Measures - and What It Does NOT
- Measures: Overall atherosclerotic plaque burden in the coronary arteries
- Does NOT correlate with the physiologic or anatomic significance of any individual stenosis - a high calcium score does not mean there is flow-limiting disease
- In young symptomatic patients, a negative (zero) calcium score does NOT exclude significant coronary artery stenoses (non-calcified plaques can still cause obstructive CAD)
- In high CAC score settings (>400), CT angiography specificity drops because the blooming artifact of calcium obscures luminal evaluation
- Goldman-Cecil Medicine; Grainger & Allison's Diagnostic Radiology
Clinical Indications and Appropriate Use
CAC scoring is most useful for intermediate-risk patients - those with a 10-year Framingham/Pooled Cohort risk of 10-20% - where the result can meaningfully shift management:
- Upgrade risk (score high for age/sex) -> intensify preventive therapy, consider statins
- Downgrade risk (score unexpectedly low or zero) -> avoid unnecessary statin therapy, reassure
For low-risk patients, a CAC rarely changes management. For already high-risk patients, the result also rarely changes the clinical approach (statins and risk reduction are already indicated). Per the 2010 ACC Appropriate Use Criteria, CAC scoring is appropriate in:
- Asymptomatic patients without known CAD who have a family history of premature ischemic heart disease
- Asymptomatic intermediate-risk patients for risk stratification
- Grainger & Allison's Diagnostic Radiology; Goldman-Cecil Medicine
Prognostic Power
The prognostic value of CAC is well established:
- CAC = 0: 12-year ASCVD event rate well below the 7.5% threshold used for statin recommendations; associated with excellent long-term prognosis
- CAC > 100 Agatston units: Relative hazard for coronary events 7-10 fold higher than individuals with no calcification, even after adjustment for all major established risk factors
- 15-year all-cause mortality in asymptomatic patients ranges from ~3% (CAC = 0) to ~28% (CAC > 1000)
- CAC scoring is the most effective and reliable means for reclassifying risk after standard risk factor assessment - it correctly reclassifies both lower-risk individuals who will have events and higher-risk individuals who will not
- Goldman-Cecil Medicine; Harrison's 22E
Sex Differences
From the CAC Consortium (Fuster/Hurst data):
- Prevalence of detectable CAC in women ranges from 26% to 72% for ages 50-70
- Women with multivessel CAC have nearly 2-fold higher long-term ASCVD mortality than men with equivalent multivessel CAC, possibly because calcium burden layered onto smaller epicardial vessels disproportionately worsens risk in women
- CAC scoring is particularly helpful in women, where global risk scores (e.g., Pooled Cohort Equations) can be imprecise
- Fuster and Hurst's The Heart, 15th Ed., p. 2252
Key Technical Notes
- Performed without contrast; ECG-gated to minimize cardiac motion
- Radiation dose: ~1-2 mSv (very low)
- Modern CT equipment with iterative reconstruction can now perform diagnostic CT angiography even in patients with very high CAC scores (previously >400-1000 was considered a contraindication to CTA) - Grainger & Allison's
- CAC score is age, sex, and race dependent - always interpret using population-specific percentiles
Recent Evidence Update
A 2025 meta-analysis (PMID 39243235) in JACC Cardiovascular Imaging examined coronary artery calcium density (not just volume/area) and found that calcium density independently predicts cardiovascular events, adding nuance beyond the standard Agatston score - higher density calcium may actually confer lower risk per unit of calcium area, suggesting plaque stability differences.
Summary: CAC scoring is a fast, low-radiation, non-contrast CT tool that quantifies coronary atherosclerosis via the Agatston score. A score of 0 carries excellent prognosis. Its greatest clinical value lies in risk reclassification of intermediate-risk asymptomatic patients to guide statin and preventive therapy decisions. It does not localize stenoses or assess physiology - that requires coronary CTA or stress testing.
This is a shared conversation. Sign in to Orris to start your own chat.