Aps in hypothyroidism
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Finding Sources
I now have all the information needed to give a comprehensive answer about Action Potentials (APs) in hypothyroidism. Here is the full answer:
Action Potentials (APs) in Hypothyroidism
Mechanism - Ion Channel Changes
Thyroid hormones (T3/T4) regulate the expression of multiple cardiac ion channel genes. In hypothyroidism, reduced thyroid hormone levels alter this channel expression, leading to characteristic changes in the cardiac action potential:
- Decreased K⁺ channel expression (especially IKr/IKs) - reduces repolarizing current
- Altered Na⁺/Ca²⁺ channel function - slows depolarization and conduction
- Increased parasympathetic tone - slows sinoatrial node firing
These changes combine to prolong the action potential duration (APD), particularly affecting Phase 3 repolarization.
ECG Correlates
As a direct result of the above ion channel changes and increased parasympathetic tone, the ECG in hypothyroidism classically shows:
| ECG Finding | Mechanism |
|---|---|
| Sinus bradycardia | Increased vagal tone + reduced SA node automaticity |
| Low voltage | Pericardial effusion + myxedematous infiltration |
| Prolonged QT interval | Prolonged action potential duration (delayed repolarization) |
| Prolonged PR interval | Slowed AV conduction |
Clinical Consequence - Torsades de Pointes
The prolongation of the AP duration extends the QT interval, which predisposes patients to ventricular arrhythmias. Some patients develop acquired torsades de pointes (TdP) - a potentially fatal polymorphic ventricular tachycardia. Importantly, this arrhythmia can improve or completely resolve with thyroid hormone replacement therapy, confirming the causal link. (Braunwald's Heart Disease, p. 1150)
Broader Cardiac Effects in Hypothyroidism
The AP changes occur in the context of wider hemodynamic disturbances:
- Reduced cardiac output - can fall by 30-40%
- Increased systemic vascular resistance - rises up to 30%; diastolic hypertension in ~20%
- Impaired LV diastolic relaxation - reduced preload and filling
- Pericardial effusion - present echocardiographically in up to 30% of overt hypothyroid patients; contributes to low ECG voltage
- Reduced LV ejection fraction at rest and during exercise - reverses with treatment
In subclinical hypothyroidism, diastolic dysfunction and vascular stiffness occur even before overt symptoms appear.
Thyroid Hormones and Cardiovascular Risk
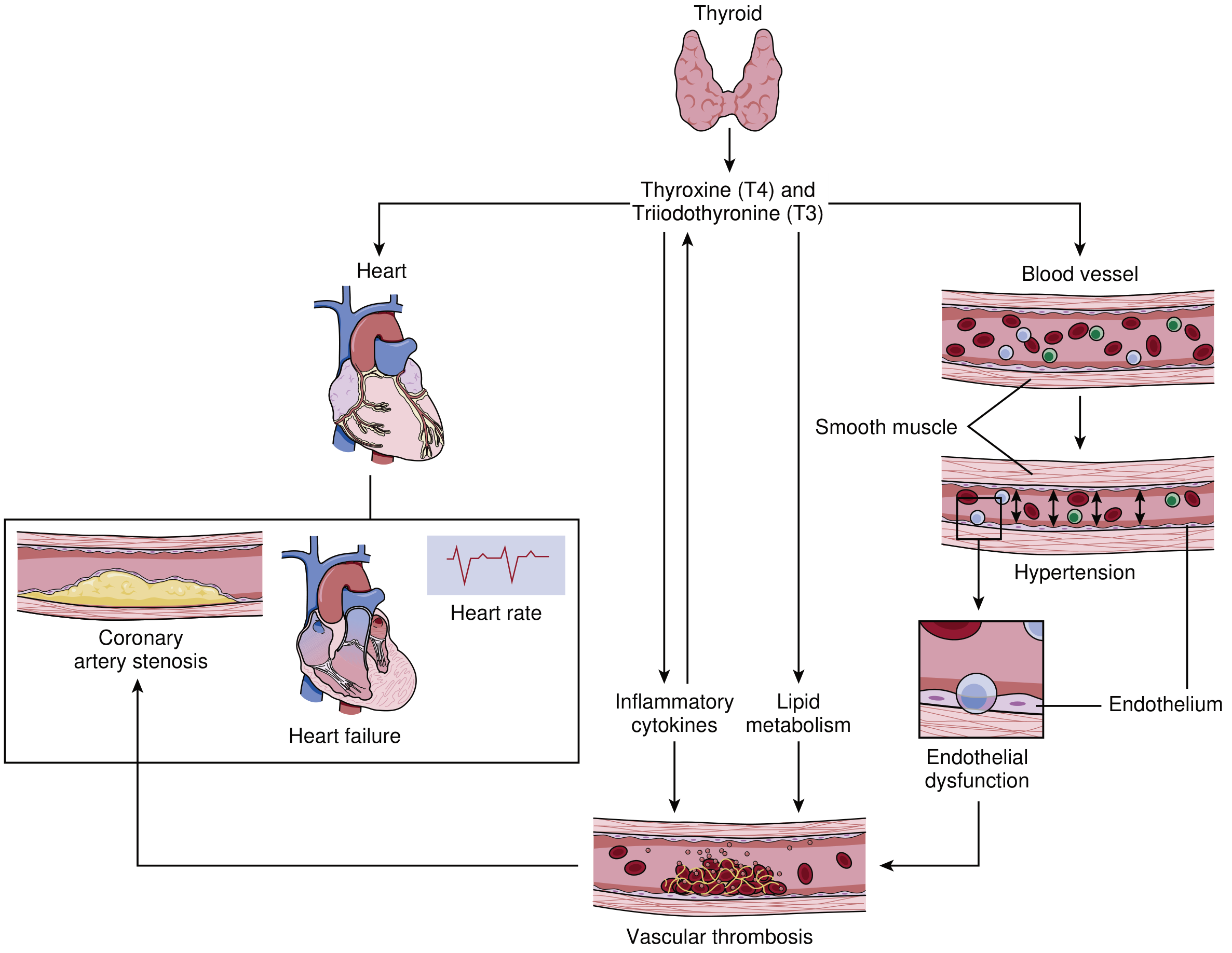
Figure: T3/T4 effects on heart rate, cardiac function, vascular smooth muscle, endothelium, lipid metabolism, and inflammatory pathways - all impaired in hypothyroidism (Braunwald's Heart Disease)
Coronary and Vascular Risk
Hypothyroidism also raises total and LDL cholesterol (via reduced hepatic LDL receptor expression and reduced cholesterol 7α-hydroxylase activity), contributes to hypertension, endothelial dysfunction, and elevated homocysteine - all increasing atherosclerotic risk. Perfusion scan defects suggestive of ischemia are described and tend to resolve with hormone replacement.
Key Takeaway
The cardinal AP change in hypothyroidism is prolonged action potential duration due to reduced K⁺ channel expression, manifesting as QT prolongation on ECG, with the risk of acquired torsades de pointes - reversible with levothyroxine replacement.
- Source: Braunwald's Heart Disease, 15th Ed., pp. 1150-1151 (Cardiovascular Effects of Overt and Subclinical Hypothyroidism)
This is a shared conversation. Sign in to Orris to start your own chat.