Aetiology of leg ulcer
Aetiology of leg ulcer. headings_fts and paragraphs_fts, read relevant sections, fetch images, compile comprehensive structured answer
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
"leg ulcer" AND aetiology
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Finding Sources
Reading File
Reading File
Finding Sources
I now have rich, comprehensive content from multiple textbooks. Let me compile the full structured answer.
Aetiology of Leg Ulcer
A leg ulcer is defined as a break in the epithelial continuity of the skin of the lower limb that fails to heal within the expected timeframe. A prolonged inflammatory phase leads to overgrowth of granulation tissue; attempts at healing by scarring leave a fibrotic margin. Necrotic tissue at the ulcer centre is called slough.
- Bailey and Love's Short Practice of Surgery, 28th Ed.
Prevalence & General Principles
- Leg ulcers are the most common chronic wounds in developed countries.
- Community prevalence: 0.1-0.3% in adults, rising to 2-4% in the elderly.
- About 1% of people in industrialised countries will suffer a leg ulcer at some point in their lives.
- Effective treatment of any leg ulcer depends on identifying and treating the underlying cause; diagnosis is therefore vital before starting therapy.
Classification of Aetiology (Summary Box)
From Bailey & Love's Summary Box 3.7:
| Category | Specific Causes |
|---|---|
| Vascular | Venous (superficial incompetence, deep incompetence, obstruction), Arterial ischaemia, Mixed (venous + arterial) |
| Trauma | Bites, self-inflicted, burns |
| Infection | Bacterial, fungal, mycobacterial, syphilis |
| Metabolic disorders | Diabetes mellitus, gout, calciphylaxis |
| Autoimmune disorders | Vasculitis, systemic sclerosis, rheumatoid arthritis |
| Neoplastic | Squamous cell carcinoma, basal cell carcinoma |
1. Venous (Chronic Venous Insufficiency) - Most Common
Venous disease accounts for ~85% of all chronic lower limb ulcers in resource-rich countries.
Mechanism (Pathophysiology)
- The only accepted underlying mechanism is ambulatory venous hypertension - this explains why venous ulcers are never seen in the upper limb.
- Venous hypertension arises from:
- Primary valve incompetence of the saphenous veins
- Incompetence of the perforating (Cockett) veins
- Incompetence or obstruction of the deep veins
- Calf-muscle pump failure
This generates capillary wall distention and leakage of macromolecules, limiting oxygen delivery. The sequence of proposed mechanisms includes:
- Fibrin cuff theory - High venous pressure causes pericapillary fibrin deposition, acting as an impediment to oxygen and nutrient diffusion.
- White cell trapping - Leukocytes are sequestered in the microcirculation of hypertensive legs, releasing proteolytic enzymes and reactive oxygen species (ROS) that cause tissue damage.
- Growth factor trap hypothesis - Macromolecules leaked from capillaries bind and inactivate growth factors needed for repair.
- ROS/proteolytic enzyme theory - Reactive oxygen species and matrix metalloproteinases are elevated in the ulcer environment, sustaining tissue damage.
Clinical Features
-
Location: Gaiter region (between calf muscles and ankle), predominantly medial side near the Cockett perforators / posterior arch vein
-
Gently sloping ulcer edge with a granulating, sloughy base
-
Surrounding haemosiderosis (brown pigmentation from haemosiderin + melanin)
-
Chronic cases develop lipodermatosclerosis (LDS) - thickening, fibrosis, pigmentation, induration of calf skin
-
Extension onto the foot or upper calf is uncommon; if present, other diagnoses must be considered
-
Bailey and Love's Short Practice of Surgery, 28th Ed., pp. 1061-1063
-
Sabiston Textbook of Surgery, p. 2320
2. Arterial (Ischaemic) Ulcers
- Arise from atherosclerotic occlusive disease causing peripheral arterial insufficiency.
- 15-30% of patients with apparent 'venous' ulcers have concomitant arterial occlusive disease - these are termed mixed ulcers.
Causes / Risk Factors
- Atherosclerosis (long-standing hypertension, smoking, hyperlipidaemia, diabetes)
- Thromboangitis obliterans (Buerger disease) in progressive cases
- Cholesterol emboli (sudden onset, eosinophilia, palpable pulses, associated renal insufficiency)
Clinical Features
-
Location: Lateral ankle, tips of toes, lateral heel, distal digits, pretibial area
-
Very tender, well-demarcated, deep ulcer with irregular borders and a pale base
-
Minimal granulation tissue; membranous inactive eschar
-
Surrounding skin: atrophic, dry, shiny; absent hair; pallor on elevation; dependent rubor; cold extremity
-
Decreased or absent peripheral pulses; ABI < 0.75 confirms arterial insufficiency; ABI < 0.5 indicates severe insufficiency
-
Andrews' Diseases of the Skin, pp. 67-69
-
Sabiston Textbook of Surgery, p. 2323
-
Fitzpatrick's Dermatology, Table 148-5
3. Neuropathic Ulcers
- Most commonly associated with diabetic sensory neuropathy and leprosy.
- Result from repeated unperceived pressure/trauma at pressure points on an insensate foot.
- Tissue necrosis and failure to heal are compounded by vascular disease and secondary infection.
Clinical Features
-
Location: Heels, toes, shins, pressure points (plantar aspect of metatarsal heads)
-
Painless ulcer surrounded by callus (hyperkeratosis)
-
Smooth surrounding skin with possible anhidrosis and sensory deficit
-
Risk of secondary osteomyelitis
-
Andrews' Diseases of the Skin, pp. 80-84
-
Robbins & Cotran Pathologic Basis of Disease, p. 115
4. Mixed Ulcers (Venous + Arterial)
-
15-30% of clinically apparent venous leg ulcers have co-existing arterial occlusive disease.
-
Compression therapy (the cornerstone of venous ulcer management) is contraindicated if ABI ≤ 0.5, per SVS/AVF practice guidelines.
-
These ulcers are harder to heal and require both vascular assessment and careful wound care.
-
Bailey and Love's Short Practice of Surgery, 28th Ed.
5. Autoimmune / Inflammatory Ulcers
| Condition | Mechanism |
|---|---|
| Rheumatoid arthritis | Vasculitis of small vessels; skin fragility from corticosteroid use |
| Systemic lupus erythematosus | Immune complex vasculitis |
| Systemic sclerosis | Microvascular obliteration leading to digital and leg ischaemia |
| Pyoderma gangrenosum | Neutrophilic dermatosis with pathergic ulceration |
| Vasculitis (other) | Leukocytoclastic or systemic vasculitis causing ulceration |
These diagnoses should be considered when ulcers are atypical, fail to respond to standard treatment, or occur in patients with known connective tissue disease.
- Bailey and Love's Short Practice of Surgery, 28th Ed.
6. Infective Ulcers
Particularly important in low- and middle-income countries:
- Bacterial: Tropical phagedaenic ulcer (Fusobacterium/Borrelia), Buruli ulcer (Mycobacterium ulcerans)
- Fungal: Deep mycoses (e.g. sporotrichosis, blastomycosis)
- Mycobacterial: Tuberculosis cutis, Buruli ulcer
- Treponema: Syphilis (gumma), yaws
- Parasitic: Leishmaniasis
7. Metabolic Ulcers
| Condition | Mechanism |
|---|---|
| Diabetes mellitus | Combination of neuropathy, microvascular disease, and infection susceptibility |
| Gout | Tophaceous deposits may ulcerate through skin |
| Calciphylaxis | Calcium deposition in small vessel walls causing ischaemic necrosis (seen in renal failure/hyperparathyroidism) |
8. Neoplastic Ulcers
-
Marjolin's ulcer - malignant transformation (usually squamous cell carcinoma, occasionally basal cell carcinoma) arising within a chronic longstanding venous ulcer.
-
Primary skin neoplasms: BCC, SCC, malignant melanoma, Kaposi's sarcoma, cutaneous lymphoma.
-
Any chronic ulcer unresponsive to standard treatment should be biopsied to exclude malignancy. A significant elevation of the ulcer edge is a warning sign for carcinoma.
-
Bailey and Love's Short Practice of Surgery, 28th Ed.
9. Traumatic Ulcers
- Burns, bites, self-inflicted wounds, radiation-induced ulcers
- May fail to heal due to underlying vascular insufficiency or wound infection
10. Haematological / Systemic Causes
Investigated in atypical or treatment-resistant ulcers:
| Cause | Notes |
|---|---|
| Sickle cell disease | Medial ankle ulceration from sickling in microvasculature |
| Pernicious anaemia | Tissue hypoxia from anaemia |
| Other haemolytic anaemias | Thalassaemia, hereditary spherocytosis |
| Antiphospholipid syndrome | Thrombotic microangiopathy |
| Polycythaemia/cryoglobulinaemia | Hyperviscosity/cold-induced vascular occlusion |
Comparison of Major Leg Ulcer Types
(From Fitzpatrick's Dermatology, Table 148-5)
| Feature | Arterial | Venous | Neuropathic |
|---|---|---|---|
| Common site | Tips of toes, lateral heel, lower calf | Below knee; medial malleolar area | Heels, toes, shins, pressure points |
| Appearance | Very tender, irregular borders, pale base; gangrene may be present | Tender, shallow, irregular red base | Painless, surrounding callus |
| Surrounding skin | Atrophic, dry, shiny | Hyperpigmented; stasis dermatitis, oedema, visible varicosities | Smooth; anhidrosis; sensory deficit |
Clinical Images
Fig. A-D: The four main types of chronic leg ulcer (Robbins & Cotran Pathologic Basis of Disease):

(A) Venous leg ulcer - medial gaiter region, shallow with red granulating base. (B) Arterial ulcer - more extensive tissue necrosis, pale base. (C) Diabetic ulcer - plantar surface. (D) Pressure sore. (E-F) Histology: epithelial ulcer crater with chronic inflammation and granulation tissue in dermis.
Investigations to Establish Aetiology
- ABPI (Ankle-Brachial Pressure Index): essential in all leg ulcers to exclude arterial disease
- Duplex ultrasonography: assess deep and superficial venous reflux/obstruction
- FBC, blood glucose, ESR/CRP: screen for systemic/haematological causes
- Sickle cell test: in appropriate ethnic backgrounds
- Biopsy: mandatory for atypical, non-healing, or suspicious ulcers (raised edge, pigmented base) to exclude malignancy
- Wound swab: if infection suspected
- Autoimmune screen (ANA, ANCA, RF, antiphospholipid antibodies): if vasculitic or inflammatory cause suspected
Summary
The vast majority of leg ulcers (~85%) in developed countries are venous in origin, driven by ambulatory venous hypertension from valvular incompetence. Arterial ischaemia, neuropathy (especially diabetic), and mixed causes account for most of the remainder. Rarer causes include autoimmune/vasculitic disease, infection, metabolic disorders, haematological conditions, and neoplasia. A systematic approach - combining history, examination (including pulses and ABPI), duplex imaging, and biopsy when needed - is essential to establish the correct aetiology and direct appropriate treatment.
- Bailey and Love's Short Practice of Surgery, 28th Ed.
- Sabiston Textbook of Surgery
- Andrews' Diseases of the Skin
- Fitzpatrick's Dermatology, 5th Ed.
- Robbins & Cotran Pathologic Basis of Disease
Monitoring of patient in shock
Reading File
Finding Sources
Finding Sources
Searching PubMed
"shock" AND "hemodynamic monitoring"
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
I now have comprehensive, multi-source content to compile a thorough structured answer. Let me synthesize everything.
Monitoring of the Patient in Shock
Definition and Clinical Context
Shock is a state of circulatory failure in which oxygen delivery is inadequate to meet cellular metabolic demands, resulting in tissue hypoxia, anaerobic metabolism, and - if uncorrected - irreversible organ dysfunction. The primary goal of monitoring is to:
- Detect the presence and severity of haemodynamic instability and inadequate tissue oxygen delivery
- Identify the type of shock (hypovolaemic, cardiogenic, distributive, obstructive) to guide treatment
- Guide resuscitation in real time
- Determine endpoints - knowing when resuscitation is adequate
- Barash Clinical Anesthesia, 9th Ed.
- Harrison's Principles of Internal Medicine, 22nd Ed.
Overview: Minimum vs. Advanced Monitoring
(Bailey & Love's Summary Box 2.4)
| Level | Modalities |
|---|---|
| Minimum (all shocked patients) | ECG (continuous HR), Pulse oximetry (SpO₂), Blood pressure (non-invasive), Urine output (hourly) |
| Additional / invasive | Central venous pressure (CVP), Invasive arterial BP (arterial line), Cardiac output monitoring, Serum lactate + base deficit |
| Advanced / emerging | Echocardiography, Pulse pressure variation (PPV) / Stroke volume variation (SVV), Mixed/central venous O₂ saturation (SvO₂/ScvO₂), Near-infrared spectroscopy, Sublingual capnometry |
1. Cardiovascular Monitoring
A. Heart Rate (ECG)
- Continuous ECG monitoring is mandatory in all shocked patients.
- Tachycardia is an early compensatory response to shock, but is neither sensitive nor specific - pain, anxiety, drugs, and arrhythmias all alter HR.
- ECG also detects causative arrhythmias, ST changes in cardiogenic shock, and conduction abnormalities.
- Bradycardia may occur in neurogenic shock or severe vagal stimulation.
B. Blood Pressure
- Non-invasive BP: Minimum standard; frequent automated cuff measurements.
- Invasive arterial line (radial/femoral): Indicated when shock is not rapidly corrected by initial fluids, or when vasopressors are required. Provides continuous beat-to-beat BP, arterial waveform analysis, and allows repeated ABG sampling.
- Despite its limitations, BP remains the most clinically useful single measure in shock.
- Restoration of blood pressure alone does not confirm that oxygen delivery or tissue perfusion has been restored - clinical and biochemical markers may lag by hours.
- Mean Arterial Pressure (MAP) is the key pressure target: MAP ≥ 65 mmHg is the standard resuscitation target in septic shock (Surviving Sepsis guidelines), though the optimal MAP may vary by patient.
C. Central Venous Pressure (CVP)
-
CVP is measured via a central venous catheter (internal jugular, subclavian, or femoral vein).
-
There is no single "normal" CVP in shock; the absolute value alone is an unreliable predictor of fluid responsiveness or volume status.
-
CVP is a poor reflection of preload (end-diastolic volume) because ventricular compliance changes rapidly in shock.
-
CVP should be used dynamically - assess the response to a fluid challenge (250-500 mL over 5-10 minutes):
- Normal response: rise of 2-5 cmH₂O, drifts back in 10-20 min → patient euvolaemic
- No change: patient still volume-depleted → needs more fluid
- Large, sustained rise: high preload, cardiac insufficiency or volume overload → cease fluids
-
Bailey and Love's Short Practice of Surgery, 28th Ed., p. 40
2. Pulse Oximetry and Respiratory Monitoring
- Continuous SpO₂ is the minimum standard and provides non-invasive estimation of arterial oxygenation.
- Arterial blood gas (ABG) provides precise PaO₂, PaCO₂, pH, bicarbonate, base deficit, and lactate.
- Respiratory rate is monitored continuously - tachypnoea is an early sign of shock and metabolic acidosis.
- In ventilated patients, dynamic respiratory indices (see below) are particularly useful.
3. Urine Output
-
Urine output via urinary catheter is the best clinical measure of organ perfusion and the cornerstone of monitoring adequacy of resuscitation.
-
A urinary catheter should be inserted in every patient being evaluated for shock.
-
Target:
- Adults: 0.5-1 mL/kg/hour
- Most children: ≥ 1 mL/kg/hour
- Children < 2 years: 1-2 mL/kg/hour
-
Oliguria (< 0.5 mL/kg/hour) indicates inadequate renal perfusion and persistent cellular hypoxia.
-
Limitation: hourly measure only; does not provide minute-to-minute data.
-
Mulholland & Greenfield's Surgery, 7th Ed.
-
Bailey and Love's Short Practice of Surgery, 28th Ed.
4. Biochemical / Metabolic Monitoring
A. Serum Lactate
- Lactate is generated by cells undergoing anaerobic respiration due to inadequate oxygen delivery.
- Serum lactate is sensitive for both the diagnosis of shock and monitoring response to therapy.
- The time required to normalise serum lactate is an important prognostic factor for survival.
- Key thresholds:
- Lactate ≥ 2 mmol/L = elevated (concern for hypoperfusion)
- Lactate ≥ 4 mmol/L = consider shock until proven otherwise
- Serial measurements guide resuscitation progress.
- Important caveat: Not all lactic acidosis is from hypoperfusion (Type B lactic acidosis) - causes include seizure, malignancy, metformin, propofol, thiamine deficiency, cyanide, hepatic dysfunction. Treatment decisions should be based on global assessment, not lactate alone.
B. Base Deficit
- Defined as the amount of base (or acid) needed to restore blood pH to 7.40.
- Categorised as: Normal (2 to -2), Mild (-3 to -5), Moderate (-6 to -9), Severe (> -10).
- Patients with base deficit > -6 mmol/L have significantly higher morbidity and mortality.
- Base deficit has greater prognostic significance than lactate alone in assessing response to resuscitation and predicting chronic critical illness.
- Measured from ABG; reflects global tissue perfusion.
- Should be measured routinely until normalised.
C. Arterial Blood Gas (ABG)
- Provides pH, PaO₂, PaCO₂, base deficit, lactate - complete picture of metabolic state.
- Should be obtained in every patient suspected of being in shock.
- Serial ABGs assess the trajectory of resuscitation.
D. Other Biochemical Markers
- FBC: Haemoglobin level (anaemia worsens oxygen delivery); WBC (infection/sepsis)
- Serum electrolytes, creatinine, urea: Assess renal function
- Blood glucose: Hyperglycaemia common in shock; hypoglycaemia possible
- Clotting screen/INR: DIC, coagulopathy assessment
- Troponin: Myocardial injury in cardiogenic shock or demand ischaemia
- Blood cultures: Before antibiotics in septic shock
5. Cardiac Output Monitoring
Measurement of cardiac output (CO), systemic vascular resistance (SVR), and preload helps:
- Distinguish types of shock (hypovolaemic, distributive, cardiogenic)
- Guide fluid therapy and vasopressor/inotrope dosing in real time
Cardiac output monitoring is particularly indicated in:
- Patients not responding to first-line therapy
- Evidence of cardiogenic shock or myocardial dysfunction
- Patients requiring vasopressor or inotropic support
Methods:
| Method | Details |
|---|---|
| Pulmonary Artery Catheter (PAC/Swan-Ganz) | Monitors CO (thermodilution), PCWP, SVR, SvO₂. Multiple RCTs have failed to show mortality benefit; use has greatly declined. No longer routinely recommended. |
| Transpulmonary thermodilution (e.g. PiCCO) | Less invasive than PAC; provides CO, global end-diastolic volume (preload), extravascular lung water |
| Pulse waveform analysis | Continuous CO estimation from arterial line waveform; requires calibration |
| Oesophageal Doppler | Non-invasive CO measurement; Doppler ultrasound of descending aorta |
| Echocardiography (TTE/TEE) | Provides real-time ventricular function, valvular anatomy, pericardial effusion, intracardiac pressures; does not provide continuous monitoring but increasingly used in ICU/ED |
| Indicator dilution (LiDCO, etc.) | Lithium dilution technique; less invasive than PAC |
- Barash Clinical Anesthesia, 9th Ed., p. 4833
- Bailey and Love's Short Practice of Surgery, 28th Ed., p. 40
6. Dynamic Indices of Fluid Responsiveness
Static measures (CVP, PCWP) poorly predict whether a patient will respond to fluids. Dynamic respiratory indices are superior predictors:
Pulse Pressure Variation (PPV) and Stroke Volume Variation (SVV)
- During positive pressure ventilation (PPV), there are predictable cyclic changes in LV stroke volume with each respiratory cycle.
- These changes are magnified when a patient is on the steep part of the Frank-Starling curve (i.e., preload-dependent / fluid-responsive).
- PPV or SVV > 10-15% indicates the patient is likely to respond to a fluid bolus with an increase in stroke volume.
- Limitation: only valid in mechanically ventilated patients with no spontaneous breaths and sinus rhythm.
Passive Leg Raise (PLR) Test
- Raising the legs to 45° transiently increases venous return (auto-fluid challenge of ~300 mL).
- A rise in cardiac output or pulse pressure of ≥ 10% predicts fluid responsiveness.
- Advantage: reversible, applicable even in spontaneously breathing patients.
Systolic Pressure Variation (SPV)
-
Similar principle to PPV; uses systolic BP variation across respiratory cycle.
-
Barash Clinical Anesthesia, 9th Ed., pp. 4833-4834
-
Rosen's Emergency Medicine
7. Mixed and Central Venous Oxygen Saturation
Mixed Venous O₂ Saturation (SvO₂)
- Measures oxygen saturation of blood returning from the entire body to the right heart (pulmonary artery sample via PAC).
- Reflects the balance between oxygen delivery (DO₂) and consumption (VO₂).
- Normal range: 50-70%
- SvO₂ < 50%: inadequate oxygen delivery, increased tissue O₂ extraction → hypovolaemic or cardiogenic shock
- SvO₂ > 70% in a septic patient: disordered O₂ utilisation at cellular level (arteriovenous shunting); less oxygen presented to cells that cannot use it
Central Venous O₂ Saturation (ScvO₂)
-
Measured from a central line (superior vena cava).
-
ScvO₂ is a practical surrogate for SvO₂ in clinical settings.
-
In healthy individuals, ScvO₂ ≈ 2-3% less than SvO₂; in shock, ScvO₂ is typically 5-10% higher than SvO₂ (blood redistributed from abdominal to cerebral/coronary circulation).
-
Low values of either measurement reflect inadequate oxygen transport and portend worse outcomes.
-
ScvO₂ < 70% in a septic patient requires urgent correction of hypovolaemia and low cardiac output.
-
A low ScvO₂ is always abnormal; a normal or high ScvO₂ does not guarantee adequate regional perfusion.
-
Bailey and Love's Short Practice of Surgery, 28th Ed., p. 41
-
Tintinalli's Emergency Medicine
-
Mulholland & Greenfield's Surgery, 7th Ed.
8. Organ-Specific Perfusion Monitoring
(Bailey & Love, Table 2.4)
| Organ | Clinical Measure | Investigational |
|---|---|---|
| Kidney | Hourly urine output | - |
| Brain | Conscious level (GCS) | Near-infrared spectroscopy, tissue O₂ electrode |
| Gut | - (no bedside clinical measure) | Sublingual capnometry, gut mucosal pH (tonometry), laser Doppler flowmetry |
| Muscle | - | Near-infrared spectroscopy (NIRS), tissue oxygen electrode |
| Systemic | - | Lactate, base deficit, SvO₂/ScvO₂ |
Note: The brain and kidneys are organs whose blood flow is preserved until the late stages of shock by autoregulation. Therefore, consciousness and urine output are maintained until shock is severe - they are insensitive early markers of resuscitation adequacy.
9. End Points of Resuscitation
Knowing when resuscitation is adequate is as important as knowing when to start. Traditional endpoints (normal pulse, BP, urine output) are insufficient because:
"Occult hypoperfusion" - A state in which vital signs have normalised but gut and muscle beds remain underperfused, sustaining ongoing anaerobic metabolism, inflammation, and coagulation activation.
- Occult hypoperfusion is manifested only by persistent lactic acidosis and low SvO₂/ScvO₂.
- Patients in occult hypoperfusion for > 12 hours have 2-3 times the mortality of those with a limited duration of shock.
Recommended End Points of Resuscitation:
| Parameter | Target |
|---|---|
| MAP | ≥ 65 mmHg |
| Urine output | 0.5-1 mL/kg/hour |
| Serum lactate | < 2 mmol/L (or clearance ≥ 10% per hour) |
| Base deficit | > -6 mmol/L (trending towards normal) |
| ScvO₂ / SvO₂ | ≥ 70% (in septic shock); ≥ 50% others |
| Mental status | Improving consciousness |
| HR | Returning towards normal |
- Bailey and Love's Short Practice of Surgery, 28th Ed., p. 41
- Mulholland & Greenfield's Surgery, 7th Ed.
- Goldman-Cecil Medicine
10. Haemodynamic Patterns by Type of Shock
Cardiac output monitoring allows differentiation of shock types:
| Parameter | Hypovolaemic | Cardiogenic | Distributive (Septic) | Obstructive |
|---|---|---|---|---|
| CO | ↓ | ↓↓ | ↑ (early) / ↓ (late) | ↓ |
| SVR | ↑ | ↑ | ↓↓ | ↑ |
| CVP/Preload | ↓ | ↑ | ↓ (or normal) | ↑ (in tamponade/PE) |
| SvO₂ | ↓ | ↓ | ↑ (early) | ↓ |
| PCWP | ↓ | ↑ | Low/Normal | ↑ (in PE) |
Summary Table: Monitoring Modalities at a Glance
| Modality | What it measures | Limitations |
|---|---|---|
| ECG/HR | Heart rate, rhythm | Non-specific; altered by pain, drugs |
| Non-invasive BP | Systemic BP | Inaccurate in profound shock |
| Arterial line | Continuous BP, waveform, ABG access | Invasive, thromboembolic risk |
| Pulse oximetry | Arterial O₂ saturation | Inaccurate in vasoconstriction, anaemia |
| Urine catheter | Hourly urine output (renal perfusion) | Hourly only; renal autoregulation preserved late |
| CVP | Central venous pressure | Poor predictor of preload; use dynamically |
| ABG | pH, PaO₂, PaCO₂, lactate, base deficit | Intermittent; requires arterial access |
| PAC | CO, PCWP, SvO₂, SVR | Invasive; no mortality benefit proven |
| Echocardiography | Cardiac function, valve pathology, tamponade | Not continuous; operator-dependent |
| PPV/SVV | Fluid responsiveness | Only valid in fully ventilated patients, sinus rhythm |
| ScvO₂ | Global oxygen delivery/extraction | Overestimates SvO₂; regional hypoperfusion can be missed |
| Serum lactate | Global tissue hypoxia | Type B causes (non-hypoperfusion) exist |
| Base deficit | Metabolic acidosis severity | ABG-based; intermittent |
| NIRS | Regional tissue oxygenation (muscle, brain) | Investigational; limited clinical evidence |
Key Principle
Monitoring of the shocked patient must be multimodal and dynamic. No single parameter is sufficient. The clinician must integrate HR, BP, urine output, lactate, base deficit, and SvO₂/ScvO₂ together to assess both the degree of shock and the adequacy of resuscitation. Restoration of normal vital signs does not equal restoration of tissue perfusion.
Sources:
- Bailey and Love's Short Practice of Surgery, 28th Ed.
- Barash, Cullen & Stoelting's Clinical Anesthesia, 9th Ed.
- Harrison's Principles of Internal Medicine, 22nd Ed. (2025)
- Mulholland & Greenfield's Surgery: Scientific Principles & Practice, 7th Ed.
- Tintinalli's Emergency Medicine: A Comprehensive Study
- Goldman-Cecil Medicine, International Ed.
- Rosen's Emergency Medicine
Create a summary PDF of shock monitoring parameters and targets
Reading File
Running Command
Running Command
Writing File
Running Command
Running Command
Your PDF is ready - 5 pages, A4, fully formatted.
Shock Monitoring Parameters
PDF Document · PDF
Here's what's inside across the 5 pages:
| Section | Content |
|---|---|
| 1. Minimum Monitoring Standard | ECG, SpO₂, NIBP, urine output, RR, temperature, GCS - with targets and clinical notes |
| 2. Invasive Cardiovascular Monitoring | Arterial line, CVP (with fluid challenge interpretation), cardiac output methods, PAWP, SVR |
| 3. Biochemical & Metabolic Monitoring | Lactate, base deficit, ABG, Hb, glucose, creatinine, troponin, coagulation |
| 4. Oxygen Transport Monitoring | SvO₂, ScvO₂, DO₂, O₂ extraction ratio - with targets and interpretation |
| 5. Dynamic Fluid Responsiveness Indices | PPV, SVV, SPV, passive leg raise, fluid challenge - with thresholds and limitations |
| 6. Haemodynamic Patterns by Shock Type | Colour-coded table comparing hypovolaemic, cardiogenic, distributive and obstructive shock across all key parameters |
| 7. Endpoints of Resuscitation | Includes the occult hypoperfusion warning callout box and a full target table |
| 8. Organ-Specific Perfusion Monitoring | Kidney, brain, heart, gut, muscle, systemic |
| 9. Quick Reference Thresholds | Single at-a-glance table of critical values with immediate actions |
Avoidable factors that compound the response to injury
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
I now have all the content needed. Let me compile the comprehensive answer.
Avoidable Factors That Compound the Response to Injury
Background: The Metabolic Response to Injury
The body responds to significant tissue injury - whether surgical or accidental - with a series of systemic changes collectively called the metabolic (stress) response to injury. These include hormonal, neural, and cytokine-mediated changes that alter metabolism, immunity, wound healing, and organ function.
While the stress response is designed to limit damage and initiate repair, it is not entirely beneficial. It can lead to complications - particularly sepsis - which then amplify and prolong the abnormal processes and contribute to multiple organ dysfunction syndrome (MODS).
Several factors prolong the acute-phase response and keep the patient in a catabolic state. These are the avoidable factors - their recognition and control forms the basis of modern perioperative care.
- Bailey and Love's Short Practice of Surgery, 28th Ed., Ch. 1
Summary of Avoidable Factors (Bailey & Love, Summary Box 1.8)
Avoidable factors that compound the metabolic response to injury during elective surgery:
- Continuing haemorrhage / volume loss
- Hypothermia
- Tissue oedema
- Tissue underperfusion
- Starvation (including preoperative fasting)
- Immobility
Additional compounding factors also include: anaesthesia, dehydration, acute medical illness, frailty, chronic diseases, and severe psychological stress.
The Key Pathogenic Mechanism
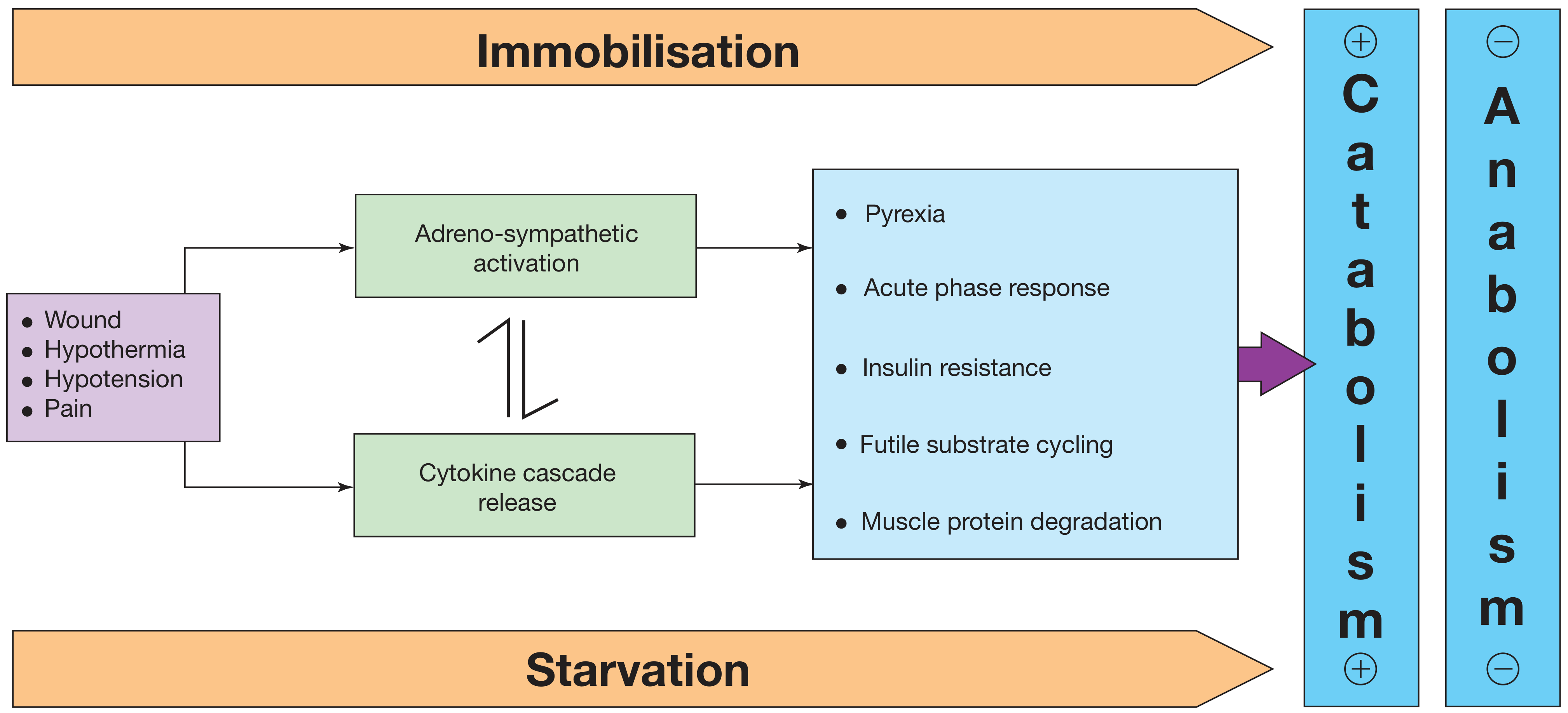
Fig. 1.7: Wound, hypothermia, hypotension, and pain → adrenosympathetic activation + cytokine cascade release → pyrexia, acute phase response, insulin resistance, futile substrate cycling, muscle protein degradation → net catabolism. Immobilisation and starvation both further amplify catabolism and inhibit anabolism.
1. Continuing Haemorrhage and Volume Loss
Mechanism
- During haemorrhage, baroreceptors in the carotid artery and aortic arch and volume receptors in the left atrial wall initiate afferent nerve signals to the CNS.
- This triggers release of:
- Aldosterone (via renin-angiotensin system activation by decreased renal perfusion pressure at the juxtaglomerular apparatus)
- ADH (antidiuretic hormone) - also stimulated by pain
- ACTH - which further augments aldosterone release
- Net effect: oliguria, sodium and water retention in the extracellular space.
- Resuscitation with saline-rich fluids exacerbates salt and water retention, leading to:
- Peripheral oedema
- Visceral oedema (e.g. stomach) → reduced gastric emptying, delayed resumption of food intake, prolonged hospital stay
Clinical Implications
- Careful limitation of intraoperative balanced crystalloids - targeting no net weight gain after elective surgery - has been proven to reduce postoperative complications and length of stay.
- Uncontrolled volume loss perpetuates the neuroendocrine stress response and maintains the catabolic state.
2. Hypothermia
Mechanism
- Hypothermia results in increased production of adrenal steroids and catecholamines.
- Even mild hypothermia (compared with normothermic controls) produces:
- A 2- to 3-fold increase in postoperative cardiac arrhythmias
- Increased catabolism
- Impaired coagulation (enzymatic coagulation cascade is temperature-sensitive)
- Increased bleeding and transfusion requirements
- Impaired immune function → increased wound infection rate
Evidence
- Randomised trials have shown that maintaining normothermia during surgery using an upper-body forced-air heating cover:
- Reduces wound infections
- Reduces cardiac complications
- Reduces bleeding and transfusion requirements
Clinical Implications
- Active warming intraoperatively (forced air blankets, fluid warmers, warm theatre)
- Temperature monitoring is mandatory in all major surgery and trauma patients
3. Tissue Oedema
Mechanism
- During systemic inflammation, fluid, plasma proteins, leukocytes, macrophages, and electrolytes leave the vascular space and accumulate in tissues.
- The mediators of increased capillary leak include:
- Cytokines (IL-1, IL-6, TNF-α)
- Prostanoids
- Bradykinin
- Nitric oxide (NO)
- Consequences:
- Diminished alveolar diffusion of oxygen → impaired gas exchange
- Impaired renal function
- Cellular hypoxia and dysfunction - intracellular volume decreases as the cell gives up fluid to replenish extravascular extracellular volume
Clinical Implications
- Goal-directed fluid therapy avoiding excessive crystalloid administration reduces oedema formation.
- Modern ERAS (Enhanced Recovery After Surgery) protocols restrict unnecessary intraoperative fluid.
4. Tissue Underperfusion (Systemic Inflammation)
Mechanism
- The vascular endothelium controls vasomotor tone, microvascular flow, and trafficking of nutrients and biologically active molecules.
- When endothelial activation is excessive (from systemic inflammation, sepsis, or haemodynamic instability):
- Compromised microcirculation
- Subsequent cellular hypoxia
- Contributes to risk of organ failure
- Hyperglycaemia commonly accompanies critical illness; insulin resistance amplifies it.
- Controlling blood glucose with insulin infusion during critical illness has been proposed to protect the endothelium, in part by inhibiting excessive iNOS-induced NO release.
Clinical Implications
- Goal: restore and maintain adequate tissue perfusion.
- Monitor with lactate, base deficit, urine output, and ScvO₂.
- Occult hypoperfusion (normal vital signs, persistent lactic acidosis) carries 2-3× increased mortality if sustained > 12 hours.
5. Starvation (Including Preoperative Fasting)
Mechanism
During starvation the body must generate ~100 g of glucose per day for obligate cerebral energy metabolism:
| Phase | Substrate Used |
|---|---|
| First 24 hours | Glycogen stores (hepatic + muscle) |
| After 24 hours | Hepatic gluconeogenesis from amino acids, glycerol, lactate |
| Prolonged starvation | Lipolysis from adipose tissue; ketone bodies replace glucose for cerebral metabolism |
- The main source of amino acids for hepatic gluconeogenesis is lean tissue (skeletal muscle) → accelerated lean tissue loss if starvation is prolonged.
- This is compounded by the pre-existing catabolic state of surgical injury.
Insulin Resistance (Related Factor)
- Following surgery or trauma, postoperative hyperglycaemia results from:
- Increased hepatic glucose production
- Decreased peripheral glucose uptake (insulin resistance)
- Insulin resistance is proportional to the magnitude of the injury.
- After routine upper abdominal surgery it persists ~2 weeks; longer with prolonged sepsis.
- Pre-operative carbohydrate loading helps attenuate this.
Clinical Implications
- 2 L of 4% dextrose / 0.18% NaCl provides 80 g glucose/day → significant protein-sparing effect.
- Modern fasting guidelines allow clear fluids up to 2 hours before anaesthesia.
- A carbohydrate drink 2 hours pre-operatively reduces perioperative anxiety and thirst and decreases postoperative insulin resistance.
- Early oral/enteral/parenteral nutrition prevents lean tissue loss.
- Avoid unnecessary fasting in all surgical and injured patients.
6. Immobility
Mechanism
- Immobility is a potent stimulus for muscle wasting.
- Inactivity impairs the normal meal-derived amino acid stimulation of protein synthesis in skeletal muscle.
- Combined with the catabolic state of injury, this dramatically accelerates loss of lean body mass.
Consequences of Prolonged Immobility
- Muscle wasting → weakness, prolonged recovery, poor wound healing
- Hypostatic pneumonia (reduced respiratory excursion, secretion retention)
- Venous thromboembolism (DVT, pulmonary embolism)
- Pressure injuries / decubitus ulcers
- Insulin resistance worsens
- Psychological morbidity (depression, delirium especially in elderly)
Clinical Implications
- Early mobilisation is one of the most important ERAS interventions.
- Avoidance of unnecessary bed rest must be actively pursued.
- Pre-habilitation programmes - optimising fitness before elective surgery - provide a better metabolic starting point, reducing susceptibility to the above effects.
7. Additional Compounding Factors (Beyond the Core Six)
Anaesthesia
- Anaesthetic agents modify the neuroendocrine stress response variably.
- Regional anaesthesia (epidural / spinal) blocks afferent nociceptive signals, attenuating the cortisol and catecholamine stress response.
- Epidural analgesia reduces postoperative insulin resistance and attenuates the catabolic response in open surgery - though it is no longer recommended for laparoscopic cases where patient-controlled analgesia (PCA) is sufficient.
Uncontrolled Pain
- Pain is a major driver of adrenosympathetic activation (see Fig. 1.7):
- Stimulates ADH release → fluid retention
- Drives catecholamine release → catabolic state, tachycardia, increased oxygen demand
- Inhibits mobility
- Adequate analgesia is not merely comfort - it is metabolic medicine that reduces the extent of the stress response.
Sepsis and Infection
- Sepsis amplifies and prolongs the acute-phase response beyond the initial injury.
- Drives ongoing cytokine cascade (IL-1, IL-6, TNF-α)
- Worsens insulin resistance
- Accelerates muscle protein degradation (via ubiquitin-proteasome pathway)
- Leads to or prolongs MODS
Pre-existing Disease / Frailty
- Frailty and chronic diseases (diabetes, malnutrition, cardiac/renal failure, immunosuppression) reduce physiological reserve and the capacity to mount and resolve the stress response appropriately.
- Patients with pre-existing poor glycaemic control pose particular challenges in managing perioperative insulin resistance.
Psychological Stress
- Severe psychological stress independently activates the adrenosympathetic axis, augmenting the catecholamine and cortisol responses to injury.
- Pre-operative carbohydrate loading and anxiolysis reduce this component.
How These Factors Interact: The Vicious Cycle
Injury
↓
Stress response (catecholamines, cortisol, cytokines)
↓
Volume loss → underperfusion → cellular hypoxia
Hypothermia → ↑ catabolism, ↑ arrhythmias, ↑ coagulopathy
Oedema → impaired O₂ diffusion, renal impairment
Starvation → lean tissue loss, insulin resistance
Immobility → muscle wasting, DVT, pneumonia
Pain → ↑ sympathetic drive, ↑ ADH
Sepsis → amplifies and prolongs all of the above
↓
Prolonged catabolism → MODS → death
Preventive Strategies: The ERAS Framework
Modern perioperative care aims to attenuate or eliminate each avoidable factor:
| Avoidable Factor | Preventive Strategy |
|---|---|
| Volume loss | Goal-directed fluid therapy; control haemorrhage promptly; avoid excess saline |
| Hypothermia | Active intraoperative warming (forced-air blankets, fluid warmers); temperature monitoring |
| Tissue oedema | Restrict crystalloid to zero net weight gain in elective surgery; colloids selectively |
| Tissue underperfusion | Optimise MAP, CO, Hb; monitor lactate/base deficit; insulin control for hyperglycaemia |
| Starvation | Carbohydrate loading 2 hrs pre-op; allow clear fluids to 2 hrs; early enteral/parenteral nutrition |
| Immobility | Early mobilisation (day 1 post-op); pre-habilitation; physiotherapy |
| Pain | Epidural (open surgery), PCA, spinal analgesia, wound catheters, IV lidocaine infusion; multimodal analgesia |
| Sepsis | Early source control; prompt antibiotics; avoid unnecessary invasive lines; infection surveillance |
ERAS programmes applying these principles together produce reductions in hospital stay of 30-50% with associated improvements in outcomes and healthcare costs.
(Bailey & Love's Short Practice of Surgery, 28th Ed., Summary Box 1.9)
Source: Bailey and Love's Short Practice of Surgery, 28th Edition, Chapter 1 - Metabolic Response to Injury
Briefly describe workup of a patient of morbid obesity and classification of bariatric procedures.
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive content from multiple authoritative sources. Let me compile the complete structured answer.
Workup of a Patient with Morbid Obesity & Classification of Bariatric Procedures
Definition and BMI Classification
Morbid (severe) obesity is defined by the WHO as:
| Class | BMI (kg/m²) | Category |
|---|---|---|
| Overweight | 25.0–29.9 | Pre-obese |
| Class I | 30.0–34.9 | Obese |
| Class II | 35.0–39.9 | Severely obese |
| Class III | ≥ 40.0 | Morbid (severe) obesity |
| Super-obese | ≥ 50.0 | Very severe obesity |
Obesity is the second leading cause of preventable death in adults in the United States (after tobacco use). Bariatric surgery is currently the only durable method of obtaining sustained weight loss and improvement of obesity-related comorbidities for most patients.
- Schwartz's Principles of Surgery, 11th Ed.
- Current Surgical Therapy, 14th Ed.
Part 1: Workup of a Patient with Morbid Obesity
A. Indications for Surgery (NIH Consensus / ASMBS Criteria)
(Current Surgical Therapy, Box 1)
- BMI ≥ 40 kg/m² (with or without comorbidities)
- BMI 35–39.9 kg/m² with significant obesity-related comorbidities (type 2 diabetes, hypertension, obstructive sleep apnoea, non-alcoholic fatty liver disease, dyslipidaemia, osteoarthritis)
- BMI 30–34.9 kg/m² with obesity-related comorbidities who have failed nonsurgical treatments (especially type 2 diabetes - ASMBS strongly recommends surgery in this group)
- Prior documented failure of nonsurgical weight loss methods (diet, physical activity, pharmacotherapy, behavioural modification)
- Clearance by a dietitian and mental health professional
- No medical contraindications to surgery
B. Contraindications
Relative contraindications:
- Inability to comply with postoperative dietary and lifestyle requirements
- Active alcohol or substance abuse
- Uncontrolled psychiatric disease
- Hostile abdomen or large incisional hernia (consider endoscopic approaches)
Absolute contraindications:
- Active malignancy
- End-stage organ failure not amenable to transplant
- Inability to tolerate general anaesthesia
C. Multidisciplinary Team Evaluation
The preoperative assessment must be multidisciplinary, including:
| Team Member | Role |
|---|---|
| Bariatric surgeon | Surgical assessment, procedure selection, risk stratification |
| Dietitian / Nutritionist | Complete dietary and behavioural eating history; postoperative dietary education; identify nutritional deficiencies |
| Psychiatrist / Psychologist | Screen for psychiatric/behavioural disorders; assess social support; ensure realistic expectations; identify eating disorders (binge eating, night eating syndrome) |
| Physician / Internist | Comorbidity assessment and optimisation |
| Anaesthetist | Airway assessment (difficult intubation), OSA/ventilation planning |
| Physiotherapist | Pre-habilitation, mobility assessment |
All patients should attend preoperative education seminars and are encouraged to join postoperative support groups.
D. History
Obesity history:
- Duration of obesity; childhood vs adult onset
- Maximum weight and BMI history
- Previous weight loss attempts (diets, exercise programmes, pharmacotherapy, prior bariatric procedures)
- Eating behaviour: binge eating, night eating, sweet eating, volume eating
Comorbidity screen (obesity-related diseases):
- Cardiovascular: hypertension, ischaemic heart disease, heart failure
- Metabolic: type 2 diabetes, dyslipidaemia, hyperuricaemia/gout, non-alcoholic fatty liver disease (NAFLD/NASH)
- Respiratory: obstructive sleep apnoea (OSA), obesity hypoventilation syndrome (Pickwickian syndrome), asthma
- Musculoskeletal: osteoarthritis (knee, hip, spine), back pain
- Gastrointestinal: GERD/hiatus hernia, cholelithiasis
- Endocrine: hypothyroidism, Cushing's syndrome (exclude secondary obesity)
- Reproductive: polycystic ovary syndrome (PCOS), infertility
- Psychological: depression, anxiety, body dysmorphic disorder, history of abuse
- Venous: DVT, chronic venous insufficiency, leg ulcers
- Neurological: idiopathic intracranial hypertension
Drug and social history:
- Current medications (especially diabetic agents, antihypertensives, anticoagulants)
- Alcohol and substance use
- Smoking status
- Social support network
E. Physical Examination
- Weight, height, BMI calculation; waist circumference
- Blood pressure (with appropriately sized large cuff)
- Cardiovascular and respiratory examination
- Abdominal examination: hepatomegaly, previous scars/hernias
- Musculoskeletal assessment: mobility, joint disease
- Skin fold assessment (intertrigo, pressure ulcers)
- Airway assessment (Mallampati score, neck circumference, thyromental distance)
- Signs of hypothyroidism / Cushing's syndrome
F. Investigations
Routine blood tests:
- FBC (anaemia, polycythaemia)
- Fasting glucose, HbA1c (diabetes assessment and control)
- Fasting lipid profile
- Urea, electrolytes, creatinine (renal function)
- LFTs (NAFLD/NASH is very common in morbid obesity)
- Serum uric acid
- TFTs (exclude hypothyroidism)
- Coagulation screen
Nutritional / micronutrient screen (important pre-operatively):
- Iron studies, ferritin
- Vitamin B12 and folate
- Vitamin D and calcium
- Thiamine (B1)
- Zinc, selenium
Cardiac:
- ECG
- Echocardiography (if cardiac disease suspected; assess for pulmonary hypertension, cardiomyopathy)
- Stress testing if indicated
Respiratory:
- Chest X-ray
- Polysomnography / sleep study: OSA is present in up to 70% of morbidly obese patients; if confirmed, CPAP/BiPAP is started pre-operatively
- Spirometry / pulmonary function tests if respiratory symptoms present
- ABG if obesity hypoventilation syndrome suspected
Gastrointestinal:
- Upper GI endoscopy: recommended pre-operatively to assess for H. pylori (eradicate before surgery), peptic ulcer disease, Barrett's oesophagus, GERD, gastric polyps
- Upper GI contrast study (barium swallow) - to assess hiatus hernia
- Ultrasound abdomen: assess for gallstones (cholecystectomy may be performed concurrently)
- Liver biopsy if severe NAFLD/NASH is suspected (occasionally intraoperative)
Endocrine:
- Overnight dexamethasone suppression test if Cushing's suspected
- Pituitary assessment if secondary obesity
Psychological:
- Formal psychiatric evaluation
- Beck Depression Inventory / PHQ-9
- Assessment for eating disorders and body image disturbance
G. Pre-operative Optimisation
- Very low calorie diet (VLCD) for 2–6 weeks before surgery: reduces hepatic volume (critical for laparoscopic access), reduces visceral fat, improves glucose control
- Optimise glycaemic control (target HbA1c < 8%)
- Treat OSA with CPAP
- Smoking cessation (minimum 6–8 weeks before surgery)
- DVT prophylaxis planning
- Alcohol cessation
- Physiotherapy / pre-habilitation
Part 2: Classification of Bariatric Procedures
Traditional Classification (Anatomic)
Bariatric procedures were classically divided into:
| Mechanism | Description | Examples |
|---|---|---|
| Restrictive | Reduce gastric capacity → early satiety, reduce intake volume | Sleeve gastrectomy, LAGB, VBG |
| Malabsorptive | Bypass segments of small bowel → reduce nutrient absorption | Jejunoileal bypass (abandoned), BPD |
| Combined (Restrictive + Malabsorptive) | Both mechanisms together | RYGB, BPD-DS, SADI-S |
Important: The traditional restrictive/malabsorptive classification is now being superseded by understanding of the underlying physiological and neurohormonal mechanisms - particularly changes in ghrelin, GLP-1, PYY, bile acids, and gut microbiota. Future classification will be based on physiologic effects rather than anatomic descriptions.
- Schwartz's Principles of Surgery, 11th Ed.
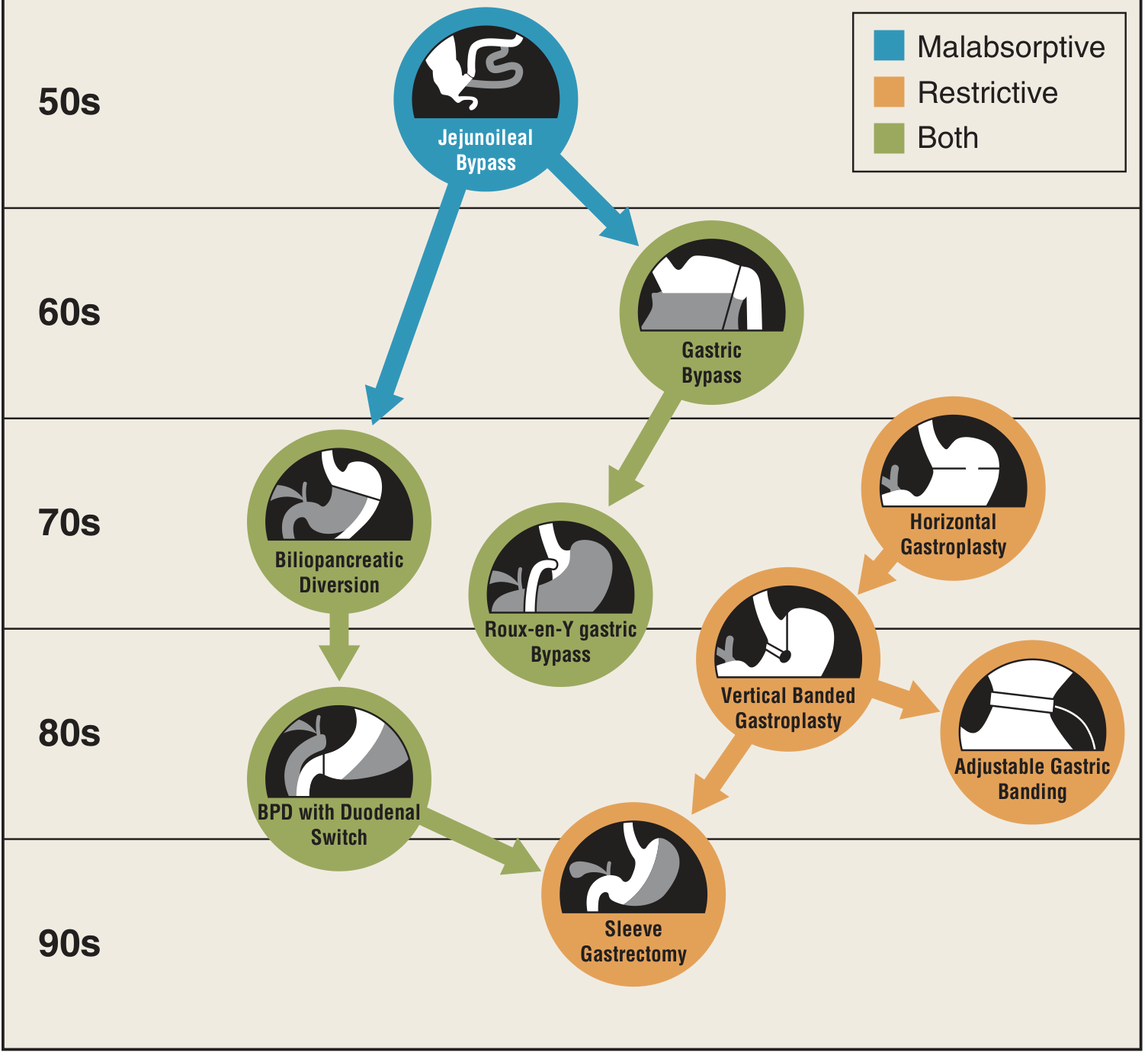
Fig. 27-1 (Schwartz's): Evolution of bariatric procedures from the 1950s to present. Blue = malabsorptive; Orange = restrictive; Green = combined.
Currently Performed Procedures
1. Sleeve Gastrectomy (SG) - Most Common Worldwide (~46%)
- Type: Primarily restrictive (+ neurohormonal effects)
- Mechanism: ~80% of the stomach is resected along the greater curvature using a linear stapler, leaving a tubular gastric "sleeve" of ~100-150 mL capacity. The fundus (main source of ghrelin) is removed.
- Key effects: Reduced gastric volume + significant reduction in ghrelin (hunger hormone) → reduced appetite
- % Excess weight loss (EWL): ~60-70% at 1 year
- Advantages: Technically simpler; no anastomosis; maintains normal GI continuity; reversible to RYGB/DS if needed
- Disadvantages: Irreversible (stomach removed); may worsen GERD; weight regain more common than RYGB long-term; staple line leak risk
- Note: Can be used as a first-stage procedure in super-obese patients (BMI > 60) before conversion to RYGB or DS
2. Roux-en-Y Gastric Bypass (RYGB) - Second Most Common (~40%)
- Type: Combined restrictive + malabsorptive + neurohormonal
- Mechanism:
- A small gastric pouch (~30 mL) is created from the proximal stomach
- A Roux limb of jejunum (alimentary limb, ~150 cm) is brought up and anastomosed to the gastric pouch (gastrojejunostomy)
- The biliopancreatic limb (containing bile and pancreatic juices) joins the Roux limb ~75-150 cm downstream at the jejunojejunostomy (creating a common channel)
- The distal stomach, duodenum, and proximal jejunum are bypassed
- Key effects: Restriction + bypass of upper gut → reduced caloric absorption + major incretin effects (↑↑ GLP-1, PYY) → improved insulin secretion and T2DM remission even before significant weight loss
- % EWL: ~70-80% at 1 year; durable at 10 years
- Advantages: Gold standard; excellent long-term weight loss and metabolic outcomes; superior T2DM remission; improves GERD
- Disadvantages: Complex procedure (2 anastomoses); risk of internal hernia; dumping syndrome; nutritional deficiencies (iron, B12, calcium); bowel obstruction requires surgery (not conservative management)
3. Biliopancreatic Diversion with Duodenal Switch (BPD-DS)
- Type: Combined (predominantly malabsorptive)
- Mechanism:
- Sleeve gastrectomy component (restrictive)
- Duodenum divided just beyond pylorus; a long Roux limb (alimentary limb ~250 cm) brought to the duodenum (duodenoileostomy)
- Very short common channel (~100 cm) → profound malabsorption
- Key effects: Maximum malabsorption → greatest weight loss of all procedures; highest rates of T2DM remission
- % EWL: ~80-90%
- Advantages: Greatest long-term weight loss; best metabolic outcomes for T2DM
- Disadvantages: Most complex; highest surgical risk; significant nutritional deficiencies (fat-soluble vitamins A, D, E, K; protein; B12, iron, zinc); requires lifelong intensive nutritional supplementation and follow-up; diarrhoea, malodorous stools
4. Single Anastomosis Duodeno-Ileal Bypass with Sleeve (SADI-S)
- Type: Combined (simplified version of BPD-DS)
- Mechanism: Sleeve gastrectomy + single duodeno-ileal anastomosis (loop anastomosis, measured 300 cm from ileocaecal valve)
- Advantages over BPD-DS: Single anastomosis reduces complexity and leak risk; similar weight loss
- Increasingly performed as an alternative to the traditional DS
5. Laparoscopic Adjustable Gastric Band (LAGB) - Now < 1% Globally
- Type: Purely restrictive
- Mechanism: An inflatable silicone band placed around the upper stomach (just below the gastro-oesophageal junction), creating a small gastric pouch (~30 mL) above the band. Band tightness adjusted via a subcutaneous port connected by tubing.
- Advantages: Reversible; no gastric resection or intestinal rerouting; adjustable; low operative risk
- Disadvantages: Poor long-term weight loss; high reoperation rates (slippage, erosion, port problems, oesophageal dilatation); nearly abandoned due to poor durability; now represents <1% of global bariatric procedures
6. Vertical Banded Gastroplasty (VBG) - Largely Abandoned
- Historically performed; combined a stapled gastric pouch with a polypropylene mesh band outlet
- Now largely replaced by sleeve gastrectomy; poor long-term outcomes
Endoscopic / Non-Surgical Procedures (for BMI 30-40 or surgical contraindications)
| Procedure | Mechanism | Duration | EWL |
|---|---|---|---|
| Intragastric Balloon (IGB) | Space-occupying fluid/gas-filled balloon; reduces gastric volume and may alter emptying | 6–12 months (temporary) | 10–15% total body weight |
| Endoscopic Sleeve Gastroplasty (ESG) | Full-thickness sutures placed endoscopically to plicate the stomach, reducing volume and compliance | Permanent (though revisable) | ~15–20% total body weight |
Both are less effective than surgical options but useful in patients with contraindications to surgery, super-obese patients as a bridge, or as adjuncts to GLP-1 agonist therapy.
Comparison Summary Table
| Procedure | Type | % EWL | T2DM Remission | Complexity | Key Risk |
|---|---|---|---|---|---|
| Sleeve gastrectomy | Restrictive + neurohormonal | 60–70% | Good | Moderate | Staple line leak; GERD |
| RYGB | Combined | 70–80% | Excellent | High | Internal hernia; nutritional deficiency |
| BPD-DS | Malabsorptive + restrictive | 80–90% | Best | Highest | Severe nutritional deficiency |
| SADI-S | Combined | 75–85% | Excellent | High | Nutritional; bile reflux |
| LAGB | Restrictive only | 40–50% | Poor | Low | Band slippage; erosion; poor durability |
| IGB (endoscopic) | Restrictive | 10–15% TBW | Minimal | Very low | Intolerance; weight regain on removal |
| ESG (endoscopic) | Restrictive | 15–20% TBW | Moderate | Low | Less durable than surgery |
EWL = Excess Weight Loss; TBW = Total Body Weight loss
Current Trends (Global, 2014 data)
- Sleeve gastrectomy: 46% (most common)
- RYGB: 40%
- LAGB: 7% (rapidly declining; <1% in USA by 2019)
- BPD-DS: remaining %
The major global shift is towards SG, with simultaneous decline in LAGB. Extension of indications from pure weight loss to metabolic surgery for T2DM (even at lower BMI) is an emerging trend backed by Level 1 randomised controlled trial evidence.
- Schwartz's Principles of Surgery, 11th Ed., Ch. 27
- Current Surgical Therapy, 14th Ed.
- Sabiston Textbook of Surgery
Damage control surgery
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
I now have rich, comprehensive content from four major surgical textbooks plus key images. Let me compile the full structured answer.
Damage Control Surgery
1. Concept and Historical Background
Damage Control Surgery (DCS) is an abbreviated, staged operative strategy applied to critically injured or physiologically deranged patients in whom a full definitive operation would prove fatal. The concept originates from a naval shipbuilding strategy: ships were designed so that damage was kept "local" and only minimal repairs were needed to prevent sinking, while definitive repairs waited until the ship reached port.
Clinically, the approach recognises that protracted surgery in the physiologically unstable patient can itself prove fatal - the lethal combination of metabolic failure ("the deadly triad" or "bloody vicious cycle") renders definitive repair impossible and dangerous.
DCS developed through the 1970s-1990s as surgeons recognised that irreversible metabolic failure made definitive surgical intervention futile, and that abbreviated laparotomy followed by ICU resuscitation and staged definitive repair improved survival.
- Bailey and Love's Short Practice of Surgery, 28th Ed.
- Sabiston Textbook of Surgery
- Schwartz's Principles of Surgery, 11th Ed.
2. The Lethal Triad ("Bloody Vicious Cycle")
The physiological basis of DCS is the recognition that three derangements interact synergistically in a downward spiral:
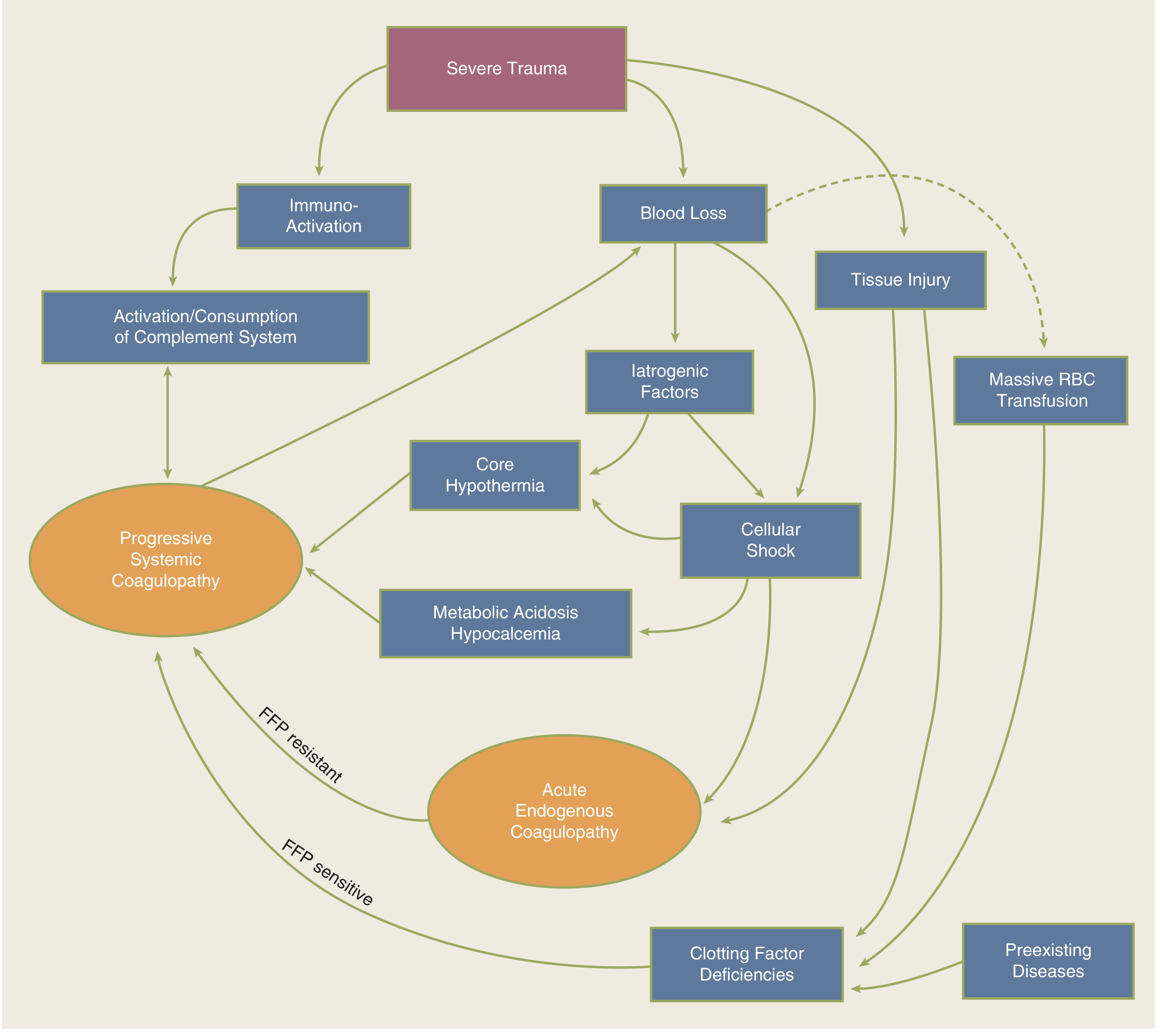
Fig. 7-48 (Schwartz's): The bloody vicious cycle. Severe trauma → blood loss + tissue injury → cellular shock, hypothermia, metabolic acidosis/hypocalcaemia → acute endogenous coagulopathy and progressive systemic coagulopathy, each component magnifying the others, culminating in fatal arrhythmia.
| Component | Mechanism | Consequence |
|---|---|---|
| Hypothermia (core temp < 35°C) | Evaporative and conductive heat loss in the open abdomen; impaired heat production; massive cold blood transfusion | Impairs enzymatic coagulation cascade; cardiac arrhythmias; ↑ catabolism; platelet dysfunction |
| Acidosis (pH < 7.2) | Anaerobic metabolism from haemorrhagic shock; aortic clamping; vasopressors; impaired myocardial performance | Directly impairs coagulation factor activity; myocardial depression; vasodilatation |
| Coagulopathy (INR/PT > 1.5×normal) | Acute traumatic coagulopathy (ATC) - caused by haemodilution, hypothermia, acidosis, consumption of clotting factors, fibrinolysis | Surgical bleeding becomes uncontrollable; haemorrhagic death |
Once the cycle starts, each component magnifies the others, leading to a fatal arrhythmia if not interrupted. The purpose of DCS is to limit operative time so the patient can be returned to the ICU for physiological restoration, thereby breaking the cycle.
3. Goals of Damage Control Surgery
DCS is restricted to only three goals:
- Stop all active surgical bleeding (haemorrhage control)
- Control contamination (GI spillage, faecal/enteric contamination)
- Restore vascular continuity where necessary (via temporary shunts if required)
After achieving the first two goals, the operation is suspended and the abdomen temporarily closed. The patient's resuscitation continues in the ICU.
4. Indications for Damage Control Surgery
(Bailey & Love Table 29.7; Sabiston Box 37.1)
Anatomical Indications
- Inability to achieve haemostasis
- Complex abdominal injury (e.g. liver and pancreas combined)
- Combined vascular, solid organ, and hollow organ injury (e.g. aortic or caval injury with bowel)
- Inaccessible major venous injury (e.g. retrohepatic inferior vena cava)
- Demand for non-operative control of other injuries (e.g. fractured pelvis requiring external fixation)
- Anticipated need for a time-consuming definitive procedure
Physiological Indications (Decline of Physiological Reserve)
| Parameter | Threshold for DCS |
|---|---|
| Core temperature | < 34°C (Bailey & Love) / < 35°C (Schwartz) |
| Arterial pH | < 7.2 |
| Serum lactate | > 5 mmol/L (Bailey) / > 4 mmol/L (Sabiston) |
| Prothrombin time | > 16 seconds |
| Partial thromboplastin time | > 60 seconds |
| Blood transfused | > 10 units PRBC intraoperatively |
| Systolic blood pressure | < 90 mmHg for > 60 minutes |
| Estimated blood loss | > 4 L |
| Clinically observed coagulopathy | Oozing from raw surfaces |
Environmental / Surgical Indications
- Operating time > 60 minutes (core temperature falls ~2°C/hour in open abdomen)
- Inability to approximate the abdominal incision
- Desire to reassess intra-abdominal contents (directed relook)
For Emergency General Surgery (Non-Trauma)
- Preoperative severe sepsis / septic shock
- Lactate ≥ 3 mmol/L
- pH ≤ 7.25
- Age ≥ 70 years
- Male sex
- Multiple comorbidities
Key principle: DCS should be considered in patients more likely to succumb to the physiological effects of shock than to the inability to complete a definitive operation.
5. Stages of Damage Control Surgery
(Bailey & Love Table 29.6)
| Stage | Intervention | Details |
|---|---|---|
| Stage 0 | Pre-hospital / ED phase | Damage control resuscitation begins in the field; time in ED minimised; resuscitation moved to the operating theatre |
| Stage I | Patient selection | Early decision to pursue DCS approach; whole surgical and anaesthetic team informed; minimise time to ICU admission |
| Stage II | Abbreviated initial surgery | Control haemorrhage + control contamination; temporary abdominal closure |
| Stage III | ICU resuscitation | Correct hypothermia, acidosis, coagulopathy; ventilatory support; physiological restoration |
| Stage IV | Definitive surgery | Return to theatre within 24-72 hours of injury for anastomoses, vascular reconstruction, bowel continuity |
| Stage V | Abdominal closure | Close fascia; if not possible: skin closure only; occasionally mesh closure with skin graft |
6. Stage 0 - Damage Control Resuscitation (DCR)
DCR is the resuscitation component of the damage control concept, extending the philosophy to the pre-hospital and emergency department phases:
- Time in the emergency department is minimised - the majority of resuscitation is carried out in the operating theatre, not the resuscitation bay
- Resuscitation is individualised through repeated point-of-care testing of:
- Haemoglobin
- Acidosis (pH and lactate)
- Clotting (INR, ROTEM/TEG)
- Directed towards early delivery of:
- Biologically active colloids
- Clotting products (FFP, cryoprecipitate, platelets)
- Whole blood (or balanced 1:1:1 ratio of PRBC:FFP:platelets)
- The physiological disturbances of the deadly triad are predicted and prevented rather than reacted to
- Permissive hypotension: In haemorrhagic shock, target systolic BP ~80-90 mmHg until haemorrhage is controlled surgically (to avoid "popping the clot" and worsening acidosis with excessive crystalloid)
- Avoid crystalloid overload: Large volumes worsen haemodilutional coagulopathy, hypothermia, and tissue oedema
7. Stage II - Operative Techniques in DCS
Haemorrhage Control
| Structure | Technique |
|---|---|
| Bleeding vessels (small) | Simple ligation |
| Major arteries | Interposition PTFE graft (aorta); temporary intravascular shunt (SMA, iliac) - arterial reconstruction within 6 hours optimal |
| Venous injuries | Preferentially ligated (except suprarenal IVC and popliteal vein) |
| Liver | Perihepatic packing (tamponades bleeding in most hepatic injuries); Foley catheter inflation in deep laceration tracks; balloon catheter tamponade for translobar gunshot wounds |
| Spleen/kidney | Splenectomy or nephrectomy - excision preferred over repair in DCS setting |
| Celiac artery | May be ligated |
| SMA | Must maintain flow - early intravascular shunt mandatory |
| Pelvic haemorrhage | Pre-peritoneal packing; REBOA (Resuscitative Endovascular Balloon Occlusion of the Aorta) |
Contamination Control
- Primary repair of simple hollow viscus perforations where feasible
- Resection of injured, perforated, or ischaemic bowel segment
- Bowel left in discontinuity (no anastomosis at this stage) - stapled ends or clamps
- Abdominal irrigation to limit ongoing contamination
- Drainage of bile/urine leaks
Extremity Damage Control
- Vascular shunting of damaged vessels (temporary restoration of flow)
- Identification and marking of damaged nerves (for later repair)
- Fasciotomy (decompression of compartment syndrome)
- Removal of contaminated/necrotic tissue
- Definitive reconstruction at subsequent operation
Thoracic Damage Control
- Control bleeding and limit air leaks using staplers (fastest available technique)
- Pulmonary tractotomy using GIA stapler (for pulmonary vessel bleeding)
- Clamshell or anterolateral thoracotomy as access
- Same philosophy: control haemorrhage → close → ICU
8. Temporary Abdominal Closure (TAC)
After haemorrhage and contamination control, the abdomen is closed in a temporary fashion:
The "Vac-Pac" / OPSITE® Sandwich Technique
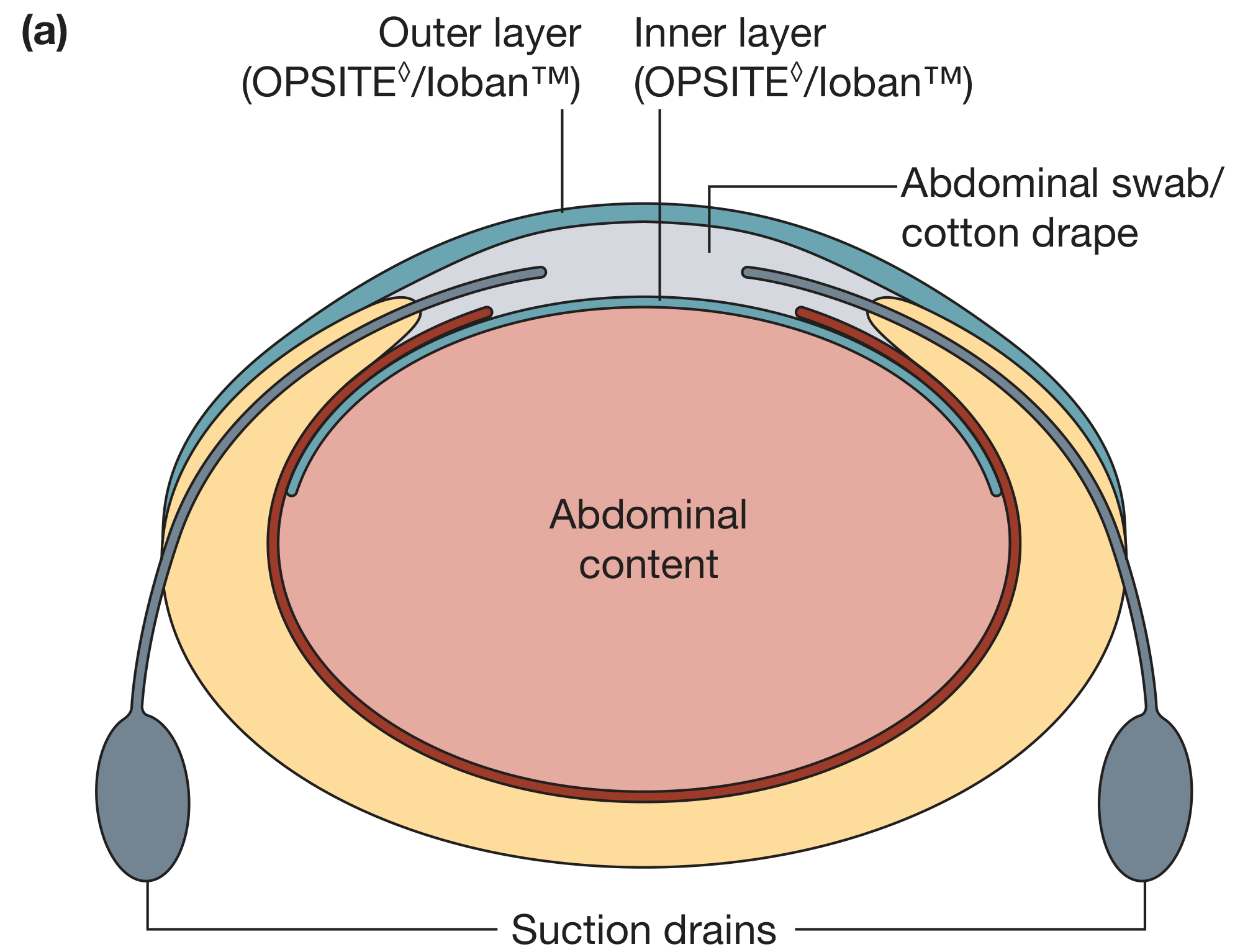
Fig. 29.12a (Bailey & Love): Temporary abdominal closure layers: inner plastic sheet over bowel, intermediate absorbent pack, outer adhesive plastic drape sealed to skin, with suction drains.
Technique:
- Inner layer: Sheet of plastic (OPSITE® or similar) placed over the bowel (not adherent to viscera)
- Middle layer: Abdominal swab/cotton drape (allows suction and collects abdominal fluid)
- Outer layer: Adherent plastic drape sealed to skin forming a watertight and airtight seal
- Suction applied to the intermediate pack to drain abdominal fluid
Commercially available alternatives: KCI ABThera, Kinetic Concepts systems with active negative pressure wound therapy - shown to achieve faster fascial closure rates than passive systems.
Goals of TAC:
- Prevent evisceration
- Collect abdominal exudate
- Allow re-exploration
- Prevent/manage abdominal compartment syndrome
9. Stage III - ICU Resuscitation
The patient is immediately transferred to the ICU for:
- Warming: Active rewarming to correct hypothermia (warming blankets, warm IV fluids, warm humidified ventilator gases, bladder irrigation)
- Correction of coagulopathy: FFP, platelets, cryoprecipitate, tranexamic acid; guided by TEG/ROTEM
- Correction of acidosis: Fluid resuscitation; sodium bicarbonate if severe; correction of underlying perfusion deficits
- Ventilatory support: Lung-protective ventilation; PEEP management
- Vasopressor support as needed (noradrenaline)
- Monitoring: Continuous lactate, base deficit, urine output, ScvO₂ trends
- Bladder pressure monitoring every 4 hours (for IAH/ACS surveillance)
- Nutritional support: Early enteral nutrition where possible
- Prevention of secondary hits: Avoid further operations until physiology corrected
10. Abdominal Compartment Syndrome (ACS)
A critical complication to anticipate and prevent in DCS patients:
Definition (World Society of ACS):
- Sustained intra-abdominal pressure (IAP) > 20 mmHg with accompanying new-onset organ dysfunction
Grading of Intra-abdominal Hypertension (IAH):
- Grade I: IAP 12-15 mmHg
- Grade II: IAP 16-20 mmHg
- Grade III: IAP 21-25 mmHg
- Grade IV: IAP > 25 mmHg
Organ effects of raised IAP (Bailey & Love Table 29.8):
| System | Effect |
|---|---|
| Renal | ↑ renal vascular resistance → ↓ GFR → AKI |
| Cardiovascular | ↓ venous return → ↓ preload → ↓ cardiac output; ↑ afterload |
| Respiratory | Diaphragmatic splinting → ↓ lung compliance, ↑ airway pressures, hypoxia |
| Visceral | ↓ gut perfusion → mesenteric ischaemia |
| Intracranial | Severe rise in ICP (via ↑ intrathoracic pressure transmitted to cerebral venous drainage) |
Measurement: Bladder pressure (indirect surrogate for IAP) measured every 4 hours in at-risk patients, at end-expiration with relaxed abdominal muscles.
Risk factors for ACS: Intra-abdominal packing, visceral/retroperitoneal oedema, haematoma, >10 units PRBC or >15 L crystalloid resuscitation, acute pancreatitis, major burns.
Prevention: Open abdomen in high-risk cases; early TAC; avoiding excessive crystalloid (damage control resuscitation).
11. Stage IV - Definitive Surgery
- Aim: return to theatre within 24-72 hours of injury
- Objectives:
- Restore bowel continuity (anastomoses)
- Definitive vascular reconstruction (replace shunts with grafts)
- Definitive repair of other injuries
- Remove packs (hepatic, pelvic)
- Closure of body cavities
- This must be individualised to the patient's response to ICU resuscitation and progression of injury
- Subsequent revisit operations may be needed (every 24-48 hours) until definitive closure is possible
12. Stage V - Abdominal Closure
- Fascial closure is the ideal - best protects against long-term complications
- If not achievable: skin closure only
- If skin closure not possible: mesh closure with skin grafting over mesh; subsequent planned abdominal wall reconstruction
- Closure complications include:
- SSI, intra-abdominal abscess
- Enteroatmospheric fistula (EAF)
- Ventral hernia
- Difficult fascial closure (fascial retraction after > 5-7 days)
- Faster time to fascial closure reduces complication rates
13. Extended Applications of DCS
DCS was originally developed for abdominal trauma but is now applied to:
| Setting | Application |
|---|---|
| Thoracic trauma | Haemorrhage control, air leak control with staplers; deferred definitive repair |
| Extremity trauma | Vascular shunting; fasciotomy; delayed reconstruction |
| Pelvic fractures | Pre-peritoneal packing; external fixation; REBOA; angio-embolisation |
| Emergency general surgery | Perforated viscus with severe sepsis/shock; intra-abdominal sepsis |
| Non-traumatic haemorrhage | Ruptured AAA, obstetric haemorrhage, spontaneous organ rupture |
14. Complications of DCS
| Complication | Notes |
|---|---|
| Abdominal compartment syndrome | Prevented by TAC; monitor IAP |
| Difficult abdominal closure | Fascial retraction; may need mesh |
| Surgical site infection | Open abdomen contamination |
| Intra-abdominal abscess | From uncontrolled contamination |
| Enteroatmospheric fistula (EAF) | Serious; bowel exposed in open abdomen |
| Ventral hernia (planned) | If skin-only closure; reconstructed electively |
| Nutritional impairment | From prolonged open abdomen |
| Overuse/misapplication of DCS | Unnecessary complications in patients suitable for definitive surgery |
A period of overutilisation of DCS following its introduction resulted in unnecessary complications in patients who were appropriate for definitive management at the index operation. Selection criteria should be rigorously applied.
Summary Box (Bailey & Love)
- Resuscitation is carried out in the operating theatre using biologically active fluids (blood) - damage control resuscitation
- Surgery performed is the minimum needed to stabilise the patient
- Aims of surgery: control haemorrhage and limit contamination
- Secondary surgery is aimed at definitive repair
Sources:
- Bailey and Love's Short Practice of Surgery, 28th Ed., Ch. 29
- Schwartz's Principles of Surgery, 11th Ed., Ch. 7
- Sabiston Textbook of Surgery, Ch. 37
- Morgan & Mikhail's Clinical Anesthesiology, 7th Ed.
- Rockwood & Green's Fractures in Adults, 10th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.