Continuous GnrH and pulsatile GNRh mechanism
GnRH: Pulsatile vs. Continuous Administration - Mechanisms
What is GnRH?
Pulsatile GnRH - The Physiological Mode
Normal Pattern
- GnRH is secreted intermittently - a few minutes at a time, once every 1 to 3 hours (approximately 60-90 min intervals).
- Its plasma half-life is only 2-4 minutes, so these pulses create sharp oscillations in portal blood GnRH, driving corresponding surges in LH and FSH.
Mechanism of Action (Pulsatile)
- GnRH binds its Gq-protein coupled receptor (GnRHR) on gonadotrophs.
- This activates phospholipase C, generating IP3 and DAG.
- IP3 raises intracellular Ca²+, triggering exocytosis of LH and FSH granules.
- DAG activates protein kinase C, supporting ongoing synthesis.
- Pulses spaced 60-90 min apart upregulate GnRH receptors on gonadotrophs (receptor sensitization).
- This leads to robust LH and FSH secretion, gonadal stimulation, and normal reproductive function.
The KNDy Pulse Generator
| Neuropeptide | Effect |
|---|---|
| Kisspeptin (Kp) | Stimulates GnRH neurons via Kiss1R receptors |
| Neurokinin B (NKB) | Stimulates kisspeptin release (auto-activating) |
| Dynorphin (Dyn) | Inhibits kisspeptin release (terminates pulse) |
Continuous GnRH - Paradoxical Suppression
Mechanism of Downregulation
- The GnRH receptor is persistently occupied - there is no "rest" period.
- This triggers receptor internalization and downregulation - the number of GnRH receptors on gonadotrophs is progressively reduced.
- With fewer receptors available, gonadotrophs become desensitized to GnRH.
- LH and FSH secretion is suppressed (initially there may be a short "flare" of gonadotropin release before suppression kicks in).
- Reduced gonadotropins lead to decreased gonadal steroid production - a state of "medical castration."
Side-by-Side Comparison
| Feature | Pulsatile GnRH | Continuous GnRH |
|---|---|---|
| Receptor effect | Upregulation (sensitization) | Downregulation (desensitization) |
| Gonadotropin output | LH & FSH stimulated | LH & FSH suppressed |
| Gonadal function | Activated | Suppressed |
| Sex steroid levels | Normal/increased | Markedly decreased |
| Physiological analog | Normal HPG axis | Medical hypogonadism |
Clinical Applications
Pulsatile GnRH (Upregulation Goal)
- Kallmann syndrome - GnRH-neuron migration defect causes hypogonadotropic hypogonadism + anosmia. Pulsatile GnRH via a programmed infusion pump restores normal folliculogenesis, ovulation, and fertility.
- Delayed puberty due to GnRH deficiency - pulsatile GnRH initiates puberty.
- Hypothalamic amenorrhea - pulsatile GnRH restores menstrual cycles.
Continuous GnRH / GnRH Agonists (Downregulation Goal)
- Endometriosis - continuous GnRH analogue suppresses estrogen, causing involution of ectopic endometrial tissue.
- Uterine fibroids (leiomyomas) - estrogen-dependent growth is blocked by hypoestrogenism.
- Prostate cancer - testosterone suppression slows hormone-sensitive tumor growth (equivalent to surgical castration).
- Breast cancer - estrogen suppression in hormone-receptor positive tumors.
- Central precocious puberty - continuous GnRH agonist halts premature pubertal progression.
Puberty: The Pivotal Role of Pulsatile GnRH
- Guyton and Hall Textbook of Medical Physiology (Chapters 81-82)
- Costanzo Physiology 7th Edition (Chapter 10)
- Medical Physiology (Boron & Boulpaep), Box 55-2 and Chapter 55
- Goodman & Gilman's The Pharmacological Basis of Therapeutics
Create a visual diagram comparing pulsatile vs continuous GnRH pathways
A clean, professional medical education diagram comparing pulsatile vs continuous GnRH pathways, split into two vertical panels side by side. LEFT PANEL - labeled "PULSATILE GnRH" with a green color theme: - At top: Hypothalamus with KNDy neurons (arcuate nucleus) shown as a brain region - Below: A wave graph showing intermittent GnRH pulses every 60-90 minutes (sharp peaks with gaps) - Arrow pointing down to: Anterior Pituitary (gonadotroph cells) - Label: "GnRH Receptor UPREGULATION" - Arrow pointing down to: LH and FSH (shown as up arrows, increased) - Arrow pointing down to: Gonads (testes/ovaries) - Label: "Gonadal Steroids INCREASED (Testosterone / Estrogen)" - At bottom: green box labeled "OUTCOMES: Normal puberty, Fertility, Reproductive function" - Clinical uses box: "Kallmann syndrome, Hypothalamic amenorrhea, Delayed puberty" RIGHT PANEL - labeled "CONTINUOUS GnRH" with a red/orange color theme: - At top: Hypothalamus with continuous GnRH release shown - Below: A flat continuous line graph showing sustained GnRH (no peaks, constant high level) - Arrow pointing down to: Anterior Pituitary (gonadotroph cells) - Label: "GnRH Receptor DOWNREGULATION (Desensitization)" - Arrow pointing down to: LH and FSH (shown as down arrows, suppressed) - Arrow pointing down to: Gonads (suppressed) - Label: "Gonadal Steroids DECREASED (Medical Castration)" - At bottom: red box labeled "OUTCOMES: Gonadal suppression, Hypoestrogenism/Hypogonadism" - Clinical uses box: "Endometriosis, Prostate cancer, Uterine fibroids, Precocious puberty" CENTER DIVIDER: A vertical dashed line separating the two panels, with a middle section showing: - GnRH molecular structure icon - KNDy neuron feedback loop diagram: Kisspeptin → GnRH neuron, Neurokinin B stimulates (+), Dynorphin inhibits (-) Overall style: Clean medical textbook illustration with clear labels, anatomical icons for hypothalamus and pituitary, color-coded arrows (green for stimulation, red for suppression), white background, professional typography
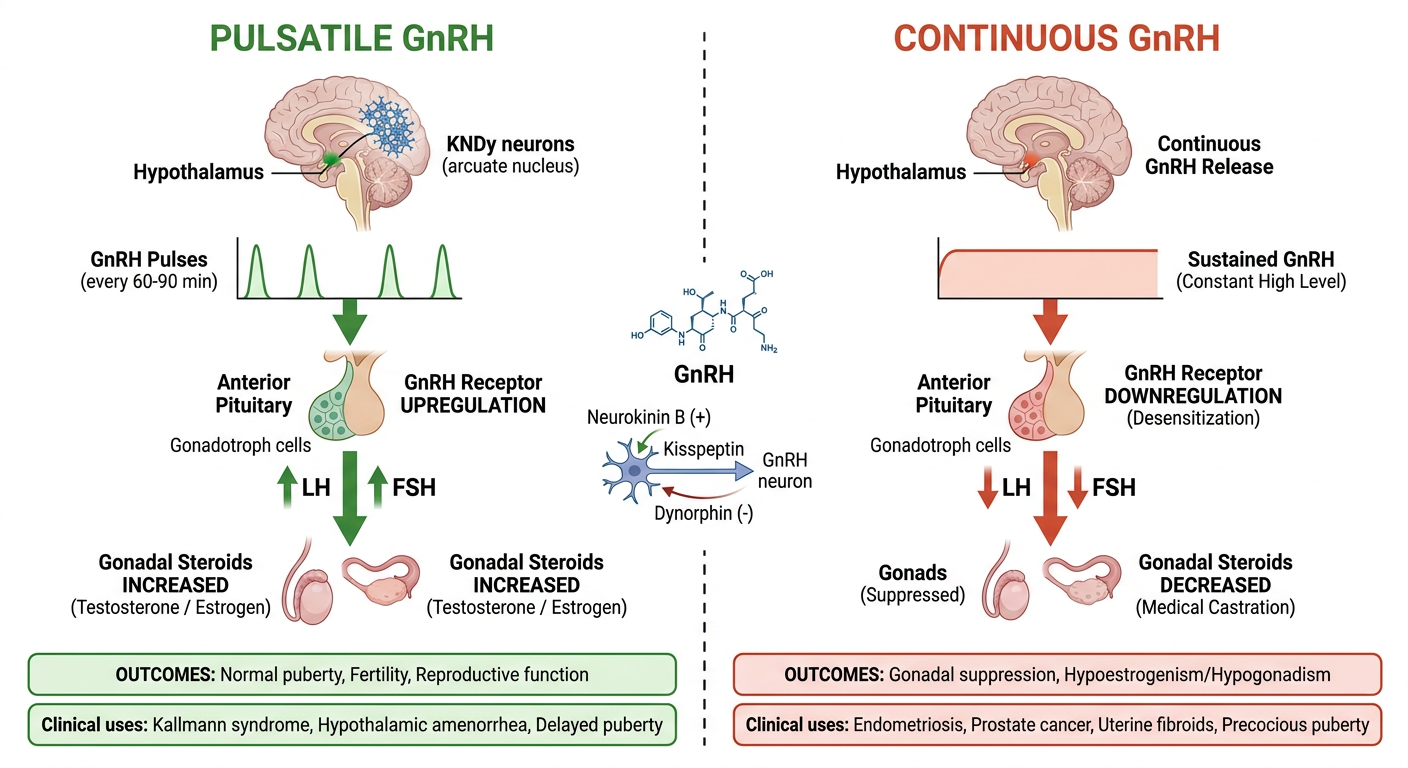
- KNDy neurons in the arcuate nucleus generate intermittent pulses every 60-90 min
- Pulse pattern upregulates GnRH receptors on gonadotrophs
- LH and FSH are stimulated - gonads are activated
- Clinical uses: Kallmann syndrome, delayed puberty, hypothalamic amenorrhea
- Neurokinin B (+) and Dynorphin (-) regulate Kisspeptin, which drives GnRH neuron firing rhythmically
- Sustained GnRH occupancy causes receptor internalization and downregulation
- Gonadotrophs become desensitized - LH and FSH are suppressed
- Leads to medical castration (hypoestrogenism/hypogonadism)
- Clinical uses: Endometriosis, prostate cancer, uterine fibroids, central precocious puberty