Rhumeatoid arthritis Clinical features Diagnosis Treatment
Reading File
Finding Sources
Searching PubMed
"rheumatoid arthritis"[MeSH Terms] AND treatment
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive, well-illustrated content. Let me compile the full answer.
Rheumatoid Arthritis (RA)
Source: Goldman-Cecil Medicine, 26th ed. | Firestein & Kelley's Textbook of Rheumatology
Definition
Rheumatoid arthritis is a chronic systemic inflammatory disease of unknown etiology that primarily targets synovial tissues. While the joint is the primary target, systemic inflammation drives important comorbidities including cardiovascular disease, osteoporosis, cognitive dysfunction, and cancer.
Epidemiology
- Global prevalence: 0.5-1% of adults
- Women are affected ~3x more than men (before menopause)
- Incidence: ~40/100,000 per year in women; ~20/100,000 in men
- Can occur at any age; prevalence rises with each decade
- Heritability ~60%; monozygotic twin concordance 12-15%
Clinical Features
Articular (Joint) Manifestations
Early disease:
- Typically begins in the small joints of the hands (PIP and MCP joints) and toes (MTP joints)
- Importantly, DIP joints are characteristically spared (unlike OA and psoriatic arthritis)
- Morning stiffness lasting >1 hour is characteristic
- Joints are warm, swollen, and tender - symmetrical involvement
Later disease:
- Larger joints become involved: wrists, knees, elbows, ankles, hips, and shoulders
- Cervical spine (C1-C2 articulation) - uniquely involved among the axial skeleton; can cause atlantoaxial subluxation, cervical myelopathy, and even death
- Temporomandibular, cricoarytenoid (hoarseness, respiratory distress), and sternoclavicular joints can be affected
Characteristic deformities (advanced disease):

| Deformity | Description |
|---|---|
| Ulnar deviation | MCPs deviate toward the ulnar side |
| Swan-neck deformity | PIP hyperextension + DIP flexion |
| Boutonniere deformity | PIP flexion + DIP hyperextension |
| Z-deformity of thumb | IP hyperextension + MCP flexion |
| Volar subluxation | MCPs and wrists |
Extra-Articular Manifestations
Systemic features (fatigue, weight loss, low-grade fever) are common. All other extra-articular features are more common in seropositive (RF+ or ACPA+) patients.
Skin:
- Rheumatoid nodules - in ~20% of patients, almost exclusively seropositive; firm, non-tender; extensor surfaces (forearms), over joints and pressure points; can also appear in lungs, heart, and eye
- Rheumatoid vasculitis - small brown infarcts of palms/fingers
Pulmonary:
- Pleural effusion (most common pulmonary manifestation)
- Interstitial lung disease (ILD) - NSIP and UIP patterns
- Pulmonary nodules, bronchiectasis
- Caplan syndrome (pneumoconiosis + RA)
Cardiac:
- Pericarditis (most common cardiac manifestation)
- Accelerated atherosclerosis/coronary artery disease (major cause of excess mortality)
- Myocarditis, conduction defects
Neurologic:
- Carpal tunnel syndrome (median nerve entrapment) - common
- Tarsal tunnel syndrome
- Mononeuritis multiplex (from vasculitis)
- C1-C2 subluxation causing cervical myelopathy
Ocular:
- Keratoconjunctivitis sicca (secondary Sjögren's) - most common
- Episcleritis, scleritis, scleromalacia perforans
Hematologic:
- Anemia of chronic disease (most common)
- Felty syndrome - triad of RA + splenomegaly + neutropenia; seen in severe RF/ACPA-positive disease
Diagnosis
RA has no single pathognomonic finding. Diagnosis requires a combination of history, physical exam, labs, and imaging.
2010 ACR/EULAR Classification Criteria
(Score ≥6/10 = classifiable as RA)
| Domain | Criteria | Points |
|---|---|---|
| Joint involvement | 1 large joint | 0 |
| 2-10 large joints | 1 | |
| 1-3 small joints (±large) | 2 | |
| 4-10 small joints (±large) | 3 | |
| >10 joints (at least 1 small) | 5 | |
| Serology | Negative RF and ACPA | 0 |
| Low-positive RF or ACPA | 2 | |
| High-positive RF or ACPA (>3x ULN) | 3 | |
| Acute-phase reactants | Normal CRP and ESR | 0 |
| Abnormal CRP or ESR | 1 | |
| Duration | <6 weeks | 0 |
| ≥6 weeks | 1 |
Laboratory Findings
| Test | Findings |
|---|---|
| Rheumatoid Factor (RF) | Positive in ~70-80%; non-specific (also positive in SLE, Sjögren's, infections, healthy elderly) |
| Anti-CCP (ACPA) | More specific (~95%) than RF; high-titer ACPA predicts more aggressive disease |
| CRP / ESR | Elevated - correlate with disease activity |
| CBC | Normocytic anemia; thrombocytosis; neutropenia in Felty's |
| Synovial fluid | Inflammatory (WBC 5,000-50,000; predominantly neutrophils) |
Imaging
- X-ray - periarticular osteopenia and soft tissue swelling (early); bony erosions and joint space narrowing (later)
- Ultrasound - detects synovitis and erosions in early disease before X-ray changes
- MRI - most sensitive for early synovitis, bone marrow edema, and erosions
Differential Diagnosis
Conditions that must be excluded include:
- Systemic lupus erythematosus (oral ulcers, rash, renal disease)
- Psoriatic arthritis (DIP involvement, nail changes, rash)
- Reactive arthritis (urethritis, history of infection)
- Crystal arthropathies (gout, CPPD)
- Viral polyarthritis (self-limiting ~2-3 weeks)
- Polymyalgia rheumatica (elderly, shoulder/hip girdle, high ESR)
Treatment
The guiding principle is "treat-to-target" - aiming for clinical remission (DAS28 <2.6) or at minimum low disease activity. Early aggressive therapy with DMARDs prevents irreversible joint damage.
Treatment Algorithm
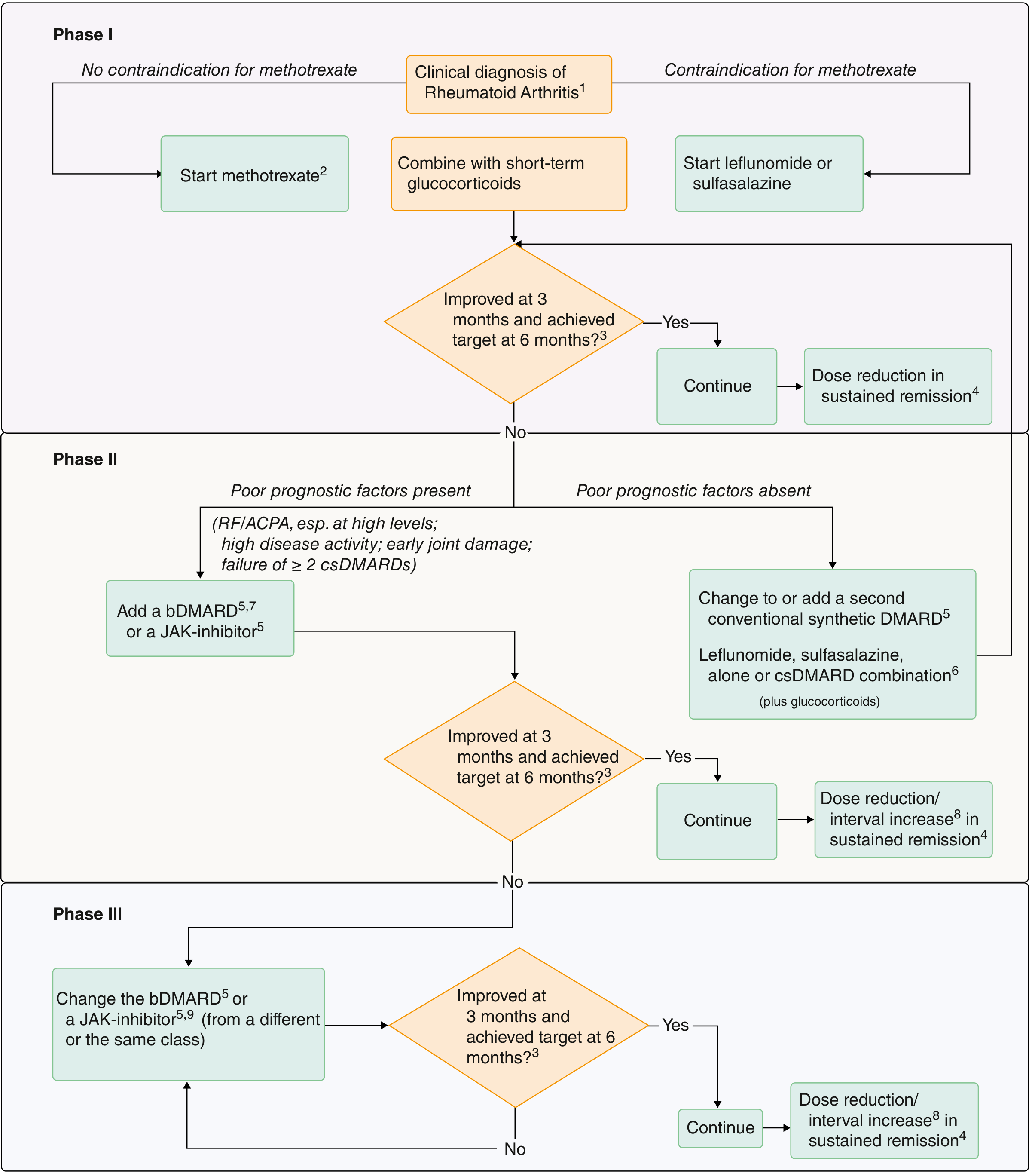
Phase I - Conventional Synthetic DMARDs (csDMARDs)
Methotrexate (MTX) - anchor drug and first-line therapy
- Oral or SC; usually 15-25 mg/week
- Folic acid supplementation required to reduce side effects (mucositis, cytopenias)
- Monitor: LFTs, CBC, creatinine
- Contraindicated in pregnancy, hepatic disease, significant renal impairment
Leflunomide - alternative to MTX
- Prodrug converted to teriflunomide; inhibits pyrimidine synthesis
- 10-20 mg/day; teratogenic (very long half-life - requires cholestyramine washout)
- Monitor LFTs
Hydroxychloroquine (antimalarial)
- 200-400 mg/day (max 5 mg/kg)
- Least toxicity of all DMARDs; no blood test monitoring needed
- Annual ophthalmology review after 5 years (retinal toxicity - rare)
- Decreases cholesterol and reduces incidence of diabetes
Sulfasalazine
- 1-3 g/day
- Monitor CBC (especially WBC) in first 6 months
Triple therapy (MTX + sulfasalazine + hydroxychloroquine) has efficacy similar to TNF inhibitor + MTX, and is more economical.
Glucocorticoids - bridge therapy during DMARD initiation; short-term only; avoid long-term use
Phase II - Biologic DMARDs (bDMARDs) or JAK Inhibitors
Used when csDMARDs fail, especially if poor prognostic factors are present (high-titer RF/ACPA, high disease activity, early joint damage, failure of ≥2 csDMARDs).
| Drug Class | Examples | Notes |
|---|---|---|
| TNF inhibitors | Etanercept, infliximab, adalimumab, golimumab, certolizumab | Most widely used; always screen for latent TB before starting |
| IL-6 receptor blockers | Tocilizumab, sarilumab | Tocilizumab superior to rituximab; effective as monotherapy |
| T-cell costimulation blocker | Abatacept (anti-CTLA4-Ig) | Blocks CD80/86-CD28 interaction |
| B-cell depletion | Rituximab (anti-CD20) | Useful in patients with prior malignancy; requires premedication |
| IL-1 inhibitor | Anakinra | Rarely used in RA |
| JAK inhibitors (tsDMARDs) | Tofacitinib, baricitinib, upadacitinib | Oral; comparable to biologics; caution re: thromboembolism, cardiac events |
All biologic therapies require infection monitoring - risk of atypical and opportunistic infections. Screen for latent TB and hepatitis B before initiation.
Phase III - Refractory Disease
Switch to a bDMARD or JAK inhibitor from a different class (or same class, different agent). Continue reassessing at 3 months; target at 6 months. Dose reduction is possible in sustained remission.
Non-Pharmacologic Measures
- Occupational therapy and joint protection strategies
- Physiotherapy to maintain range of motion and muscle strength
- Orthotics/splints (especially wrist and hand)
- Surgical intervention for severely damaged joints (synovectomy, joint replacement)
- Cardiovascular risk factor management (RA independently doubles CV risk)
- Osteoporosis prophylaxis (calcium, vitamin D; bisphosphonates if on glucocorticoids)
- Smoking cessation (smoking is a major modifiable risk factor for RA and worsens disease)
Key takeaway: RA is a treat-to-target disease. Start MTX early, assess at 3 months, and escalate to bDMARDs/JAK inhibitors if targets are not met - particularly when poor prognostic markers are present.
Sources: Goldman-Cecil Medicine 26e (pp. 2784-2800) | Firestein & Kelley's Textbook of Rheumatology, 11e
This is a shared conversation. Sign in to Orris to start your own chat.