Massive haematemesis in 60 year old man, emergency investigations and management
Reading File
Finding Sources
Finding Sources
Searching PubMed
"upper gastrointestinal bleeding"[MeSH Terms] AND management
Reading File
Finding Sources
Finding Sources
Searching PubMed
"gastrointestinal hemorrhage" AND management
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Reading File
Searching PubMed
"upper gastrointestinal bleeding" AND "endoscopy" AND "management"
I now have comprehensive information to provide a complete, well-sourced answer. Let me compile it.
Massive Haematemesis in a 60-Year-Old Man: Emergency Investigations and Management
Massive haematemesis (vomiting of large volumes of fresh blood) in a 60-year-old man is a life-threatening emergency with in-hospital mortality of 5-10%, rising to 33% when bleeding first presents in an already-hospitalised patient. Upper GI haemorrhage incidence increases with age and is strongly associated with NSAID use. (Bailey and Love's Short Practice of Surgery 28th Edition, p. 1187)
Causes (at this age)
| Condition | Approximate % |
|---|---|
| Peptic ulcer (duodenal 33%, gastric 21%, oesophageal 6%) | 60% |
| Erosions (oesophageal, gastric, duodenal) | 26% |
| Oesophageal varices | 4% |
| Mallory-Weiss tear | 4% |
| Tumour / vascular lesions | ~1% |
| Others | 5% |
In a 60-year-old, duodenal ulcer is the most common cause. Varices must be suspected if there is any clinical evidence of chronic liver disease (jaundice, spider naevi, ascites, splenomegaly).
Immediate Priorities: ABC + Resuscitation
Airway
- If haematemesis is massive or the patient is encephalopathic, protect the airway - consider early endotracheal intubation before endoscopy to prevent aspiration.
Circulation - Resuscitation
- Two large-bore IV cannulae (14-16G) peripherally; for severe bleeding add a central venous pressure line
- Urinary catheter for urine output monitoring
- Fluid resuscitation - start with crystalloid, but transfuse blood as soon as available; transfuse when >30% of blood volume has been lost
- Blood products: Correct coagulopathy (most common causes: liver disease, anticoagulation therapy) with fresh-frozen plasma or concentrated clotting factors; vitamin K 10 mg IV if liver disease suspected
- Platelets: Transfuse if count <50 × 10⁹/L (thrombocytopenia from hypersplenism in cirrhosis)
- Avoid hypervolaemia in variceal bleeding - it increases portal pressure and exacerbates bleeding
(Bailey and Love's, pp. 1187-1188, 1225-1226)
Emergency Investigations
Bloods (send immediately)
| Investigation | Rationale |
|---|---|
| FBC | Haemoglobin, haematocrit, platelet count |
| Cross-match + Group & Save | 4-6 units of packed red cells; activate major haemorrhage protocol if massive |
| Coagulation (PT/INR, APTT) | Identifies coagulopathy (liver disease, anticoagulants) |
| Urea & electrolytes | BUN:creatinine ratio >30:1 suggests upper GI source; baseline renal function |
| LFTs + bilirubin | Identifies underlying liver disease/varices |
| Serum glucose | Hypoglycaemia in liver failure |
| ABG | Oxygenation, acid-base status, lactate (tissue perfusion) |
| Amylase/lipase | Exclude pancreatitis with haemosuccus pancreaticus |
| ECG | Exclude myocardial ischaemia (especially in elderly) |
| CXR | Baseline; exclude perforation (pneumoperitoneum) |
Point-of-Care
- Bedside ultrasound (FAST/POCUS): Ascites, splenomegaly, portal hypertension signs
Risk Stratification: Rockall Score
Apply the pre-endoscopy Rockall score to guide disposition and urgency:
| Variable | Score 0 | Score 1 | Score 2 | Score 3 |
|---|---|---|---|---|
| Age | <60 | 60-79 | >80 | - |
| Shock | HR <100, SBP >100 | HR >100, SBP >100 | HR >100, SBP <100 | - |
| Comorbidities | None | - | Cardiac failure/IHD | Renal/liver failure, malignancy |
| Endoscopic diagnosis | Mallory-Weiss/none | All others | Upper GI malignancy | - |
| Endoscopic stigmata | None/dark spot | - | Blood, clot, visible/spurting vessel | - |
- A pre-endoscopy score ≥3 warrants urgent endoscopy and high-dependency care
- A Blatchford score of 0 (or ≤1) may identify patients safe for outpatient management, but NOT applicable here
(Bailey and Love's, p. 1188; a 2024 emergency medicine review confirms Rockall and Blatchford remain the standard scoring tools)
Management
Step 1: Pharmacological (start immediately, before endoscopy)
Non-variceal (suspected peptic ulcer):
- IV PPI (e.g., omeprazole 80 mg bolus then 8 mg/h infusion) - reduces rebleeding after endoscopy; no proven benefit prior to endoscopy but commonly given
- Tranexamic acid - meta-analysis data suggests may reduce overall mortality (fibrinolysis inhibition)
Variceal (suspected or known cirrhosis):
- Terlipressin 2 mg IV 6-hourly (splanchnic vasoconstrictor - first-line) - reduces portal pressure
- Alternatively: Octreotide or somatostatin infusion
- Prophylactic antibiotics (e.g., IV ceftriaxone 1 g/day) - reduces infection risk, improves survival in cirrhotic patients with variceal bleeding
Step 2: Emergency Endoscopy (OGD)
- For severe bleeding: carry out immediately after haemodynamic stabilisation
- For mild/moderate bleeding: may defer to next morning, guided by local protocol
- Do NOT delay surgery waiting for endoscopy if bleeding persists
Important: Even in suspected variceal bleeding, confirm the source endoscopically - 30% will have a non-variceal cause.
Therapeutic endoscopy (non-variceal - peptic ulcer):
- Combination therapy: Adrenaline (epinephrine) injection + heater probe/clips achieves haemostasis in ~70%
- Endoscopic clips (haemoclips) alone or combined
- Forrest classification guides intervention:
- Ia (spurting) / Ib (oozing): endoscopic therapy mandatory
- IIa (visible vessel) / IIb (adherent clot): endoscopic therapy recommended
- IIc / III (flat pigmented spot/clean base): medical management, safe discharge
Therapeutic endoscopy (variceal):
- Oesophageal varices: Band ligation preferred over sclerotherapy (lower rebleeding rate); sclerotherapy if bleeding is too profuse for ligation
- Gastric (fundal) varices: Cyanoacrylate glue injection or thrombin injection
Step 3: When Endoscopy Fails
Non-variceal:
- Interventional radiology - transcatheter embolisation (angiography): valuable alternative to surgery for unidentified source or rebleeding after endoscopy; low ischaemia risk due to rich gastroduodenal collateral supply
- Surgery: Indicated if bleeding persists or >6 units of blood required
- Frail/elderly patients paradoxically need earlier surgery (higher risk of death from continued bleeding)
- At laparotomy: duodenotomy + underrunning of gastroduodenal artery for duodenal ulcer; partial gastrectomy for gastric ulcer
Variceal:
- Balloon tamponade (Sengstaken-Blakemore tube or Minnesota tube): emergency bridge when rate of blood loss prohibits endoscopy
- Gastric balloon inflated with 300 mL air, retracted to fundus; oesophageal balloon inflated to 60 mmHg
- Maximum 24 hours (risk of oesophageal pressure necrosis)
- Self-expanding covered metal oesophageal stents are an equivalent modern alternative
- TIPSS (Transjugular Intrahepatic Portosystemic Stent Shunt): when pharmacological + endoscopic therapy have failed; now the preferred method for refractory portal hypertension; inserted under local anaesthetic via internal jugular vein under fluoroscopic/USS guidance
(Bailey and Love's, pp. 1187-1188, 1225-1226; Shung & Laine meta-analysis, 2024, PMID 38517201)
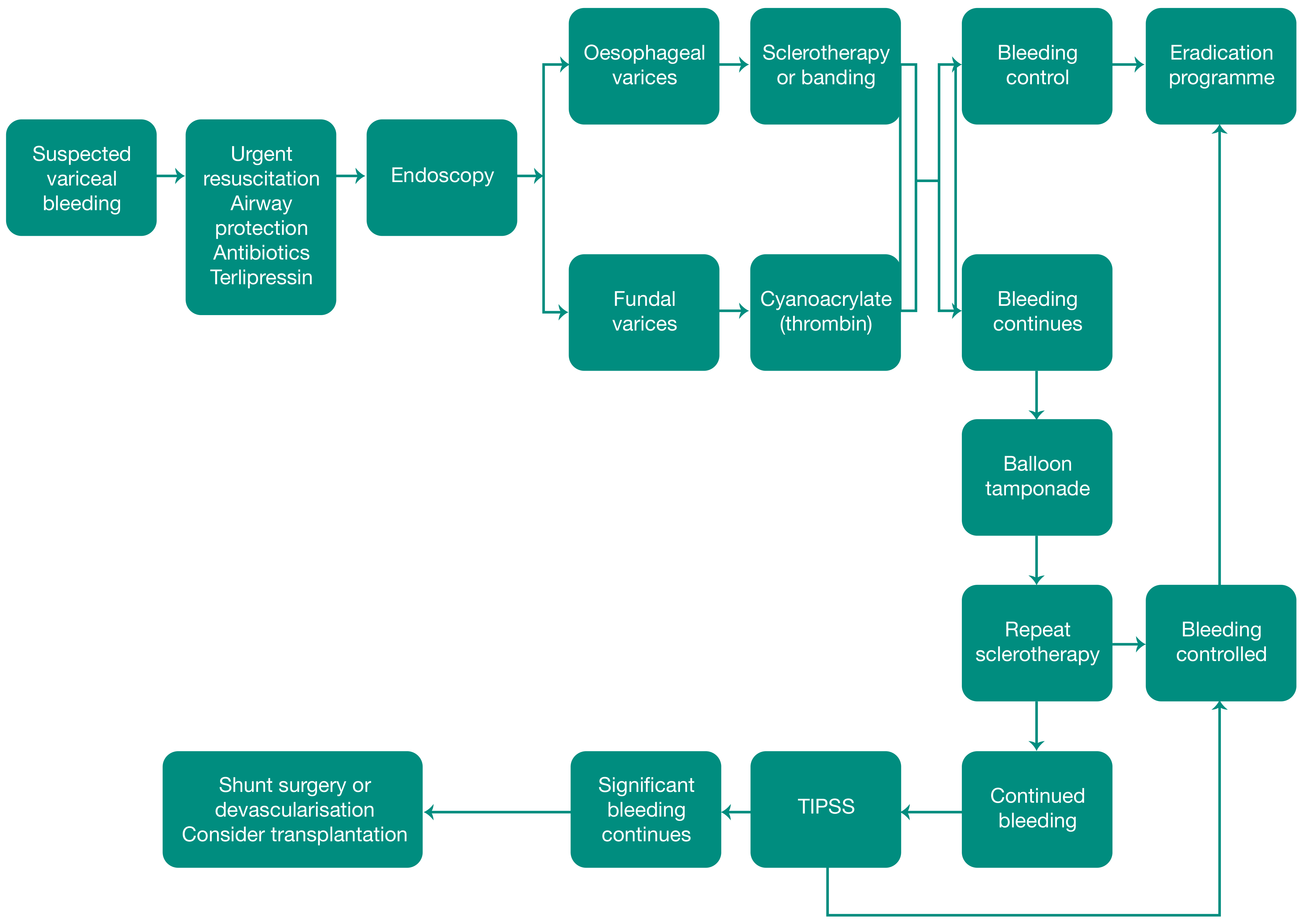
Variceal Bleeding Management Flowchart
(From Bailey and Love's Surgery, Figure 69.13)
Ongoing Monitoring
- Hourly urine output (target >0.5 mL/kg/hr)
- Serial Hb every 4-6 hours in active bleeding
- CVP monitoring in severe cases
- Coagulation profile - recheck after FFP administration
- Watch for rebleeding - in peptic ulcer: visible vessel at endoscopy, large ulcer >2 cm, vessel >2 mm diameter, and prior ulcer bleeding are independent predictors of endoscopic therapy failure (per Forrest classification data from Maingot's Abdominal Operations)
- Ward level: HDU/ITU for all cases of massive haematemesis
Key Points for a 60-Year-Old
- Age 60 scores 1 on the Rockall scale (60-79 years category) - already elevated risk
- NSAID use is a major predisposing factor at this age and should be stopped
- Comorbidities (IHD, renal impairment) shift Rockall score toward 2-3 and influence surgical fitness
- Frail or elderly patients with continued bleeding should proceed to surgery earlier, not later
- If liver disease is present, encephalopathy risk is real - consider early intubation
Sources: Bailey and Love's Short Practice of Surgery 28th Ed, pp. 1187-1188 & 1225-1226 | Long & Gottlieb, Am J Emerg Med 2024, PMID 38723362 | Shung & Laine, Aliment Pharmacol Ther 2024, PMID 38517201 | Toro Tole et al., J Gastrointest Surg 2024, PMID 38446116
This is a shared conversation. Sign in to Orris to start your own chat.