portal hypertension
Reading File
Finding Sources
Searching PubMed
"portal hypertension"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Loading Image
I now have comprehensive material to write a thorough answer. Here is a complete, structured review of portal hypertension.
Portal Hypertension
Definition
Portal hypertension is defined as elevation of the hepatic venous pressure gradient (HVPG) above 5 mmHg (normal: 1–5 mmHg). Clinically significant portal hypertension (CSPH) is defined as HVPG ≥ 10 mmHg, at which point the risk of decompensation (variceal bleeding, ascites, hepatic encephalopathy) rises substantially. Varices generally form once HVPG exceeds 12 mmHg.
The HVPG is measured as:
HVPG = Wedged Hepatic Venous Pressure (WHVP) − Free Hepatic Venous Pressure (FHVP)
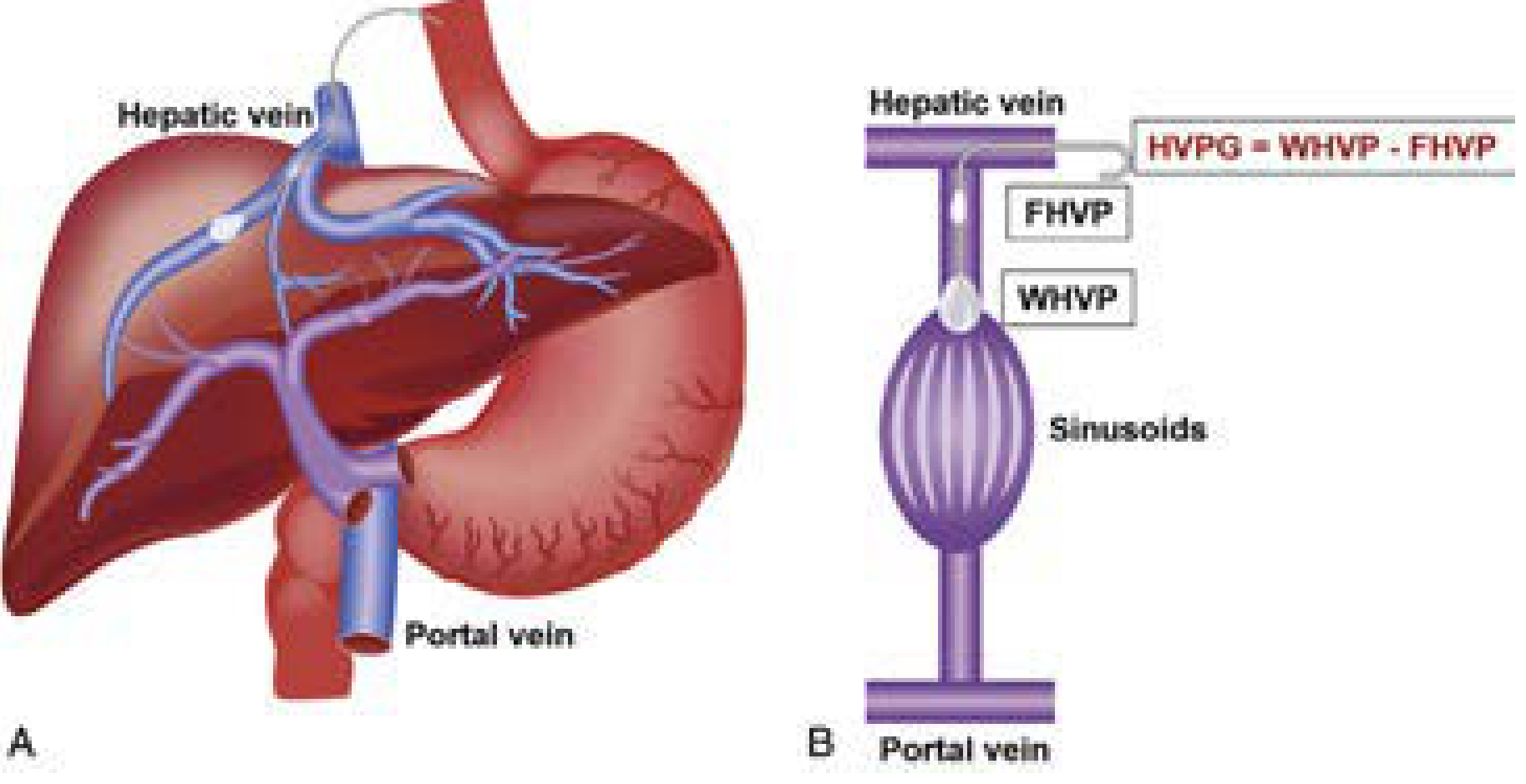
HVPG measurement. A: Transjugular balloon catheter placement. B: WHVP reflects sinusoidal/portal pressure; FHVP reflects systemic venous pressure. — Current Surgical Therapy 14e
Causes / Classification
Causes are classified by anatomical location relative to the hepatic sinusoids:
| Category | Subcategory | Examples |
|---|---|---|
| Prehepatic | — | Portal vein thrombosis, splenic vein thrombosis, massive splenomegaly (Banti's syndrome) |
| Intrahepatic | Presinusoidal | Schistosomiasis, congenital hepatic fibrosis |
| Sinusoidal | Cirrhosis (alcohol, viral hepatitis, NASH/NAFLD) — >95% of cases | |
| Postsinusoidal | Hepatic sinusoidal obstruction (venoocclusive disease) | |
| Posthepatic | — | Budd-Chiari syndrome, IVC webs, constrictive pericarditis, severe right heart failure |
In North America, cirrhosis is the dominant cause (~90% of cases). Worldwide, schistosomiasis, Budd-Chiari, and portal vein thrombosis are more frequent non-cirrhotic etiologies. — Harrison's Principles of Internal Medicine 22E; Current Surgical Therapy 14e
Pathophysiology
Two simultaneous hemodynamic processes drive portal hypertension:
1. Increased Intrahepatic Resistance
Progressive collagen deposition and nodule formation from chronic liver injury distorts sinusoidal architecture, raising mechanical resistance to portal flow. Additionally:
- Activated hepatic stellate cells (HSCs) contract, increasing dynamic vascular tone
- Nitric oxide (NO) production from eNOS is paradoxically reduced in the intrahepatic circulation of cirrhotic livers, promoting vasoconstriction — even as NO is overproduced systemically
2. Increased Splanchnic Blood Flow
Portal hypertension triggers release of vasodilator mediators (NO, prostacyclin, substance P) into the splanchnic circulation, causing arterial vasodilatation. This reduces effective arterial blood volume, which in turn activates:
- Renin-angiotensin-aldosterone system (RAAS)
- Sympathetic nervous system (SNS)
- Vasopressin
The result is sodium and water retention → expanded blood volume → hyperdynamic circulation → further increased portal inflow — a vicious cycle.
At advanced stages, bacterial translocation from the gut generates PAMPs/DAMPs → innate immune activation → systemic inflammation → further circulatory dysfunction.
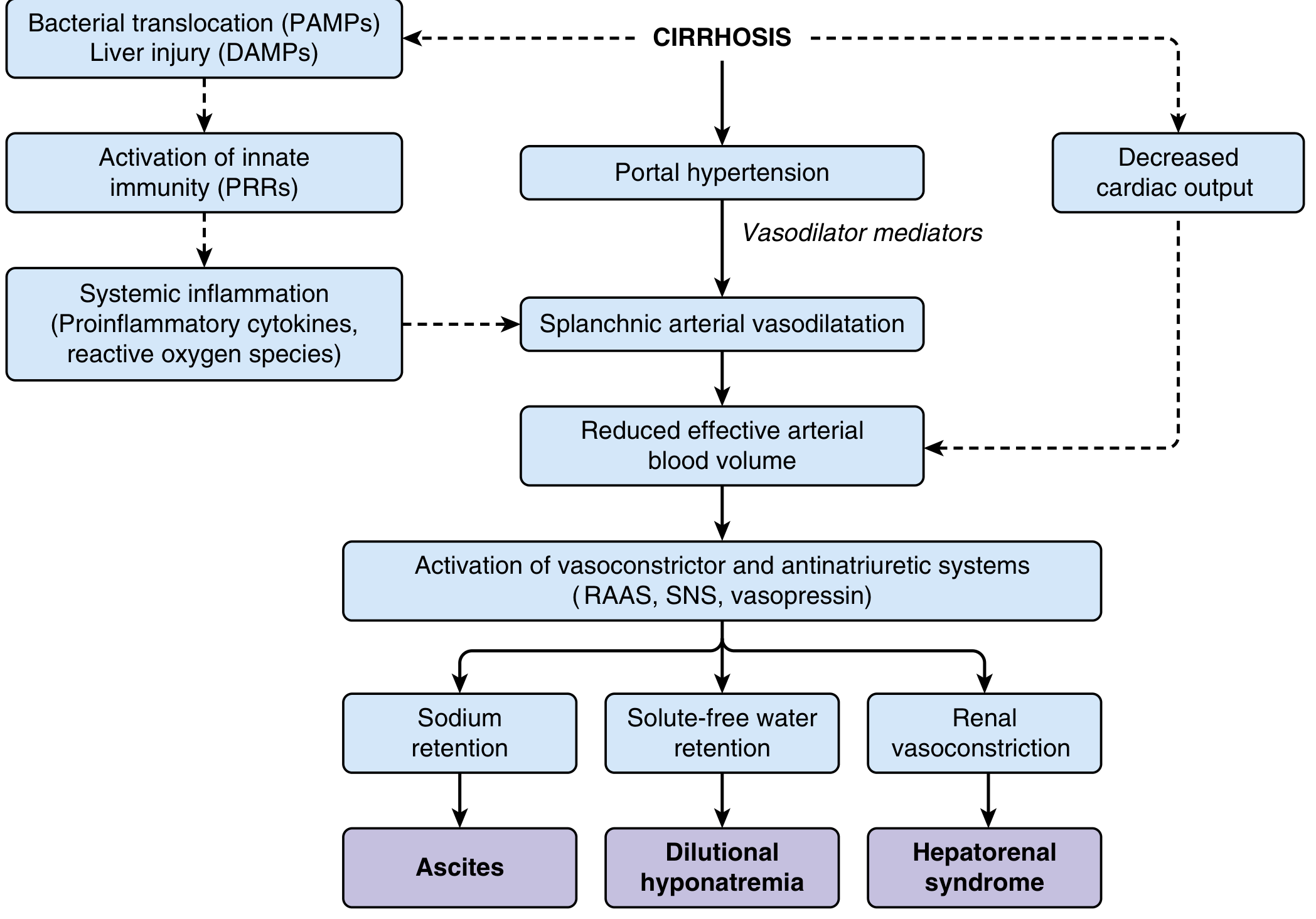
Pathophysiology of circulatory dysfunction in cirrhosis. Splanchnic vasodilatation reduces effective arterial volume, activating RAAS/SNS/vasopressin — leading to ascites, dilutional hyponatremia, and hepatorenal syndrome. — Sleisenger & Fordtran's GI and Liver Disease
Portosystemic Collaterals
As portal pressure rises, blood bypasses the liver through pre-existing anastomoses with systemic veins. Clinically important sites:
| Site | Clinical Manifestation |
|---|---|
| Lower esophagus / gastric fundus | Esophageal/gastric varices → hemorrhage |
| Periumbilical (falciform ligament) | Caput medusae |
| Rectum | Hemorrhoids (anorectal varices) |
| Retroperitoneum | Retroperitoneal collaterals |
50% of cirrhotic patients develop gastroesophageal varices; ~1/3 will bleed within the first year of diagnosis. — Current Surgical Therapy 14e
Complications
1. Variceal Hemorrhage — the most immediately life-threatening complication. Mortality ranges from 5% (Child-Pugh A) to 68% (Child-Pugh C).
2. Ascites — due to splanchnic vasodilation → reduced effective circulating volume → RAAS activation → renal Na⁺ retention. Starling forces shift fluid into the peritoneal cavity.
3. Hepatic Encephalopathy — portal blood bypasses the liver through collaterals; toxins (especially NH₃) escape hepatic clearance and cross the blood-brain barrier.
4. Hypersplenism — splenomegaly from splenic venous congestion → thrombocytopenia, leukopenia, anemia.
5. Hepatorenal Syndrome (HRS) — renal vasoconstriction from RAAS/SNS activation in the setting of effective hypovolemia.
6. Dilutional Hyponatremia — solute-free water retention from vasopressin activation.
7. Other: Hepatic hydrothorax, hepatopulmonary syndrome, portopulmonary hypertension, spontaneous bacterial peritonitis (SBP), hepatocellular carcinoma. — Sleisenger & Fordtran's
Diagnosis
- HVPG measurement (transjugular): gold standard; invasive
- Non-invasive alternatives:
- Liver stiffness (transient elastography/FibroScan): most validated; overestimated postprandially, with hepatic inflammation, cholestasis, or right heart failure
- Platelet count, spleen diameter (platelet/spleen ratio)
- Serum markers (FIB-4, APRI, FibroTest)
- Liver biopsy: gold standard for cirrhosis staging, but has sampling error and procedural risk
- Endoscopy: screens for varices; all patients with new cirrhosis/portal hypertension should undergo upper endoscopy at diagnosis and every 6–12 months — Sleisenger & Fordtran's; Current Surgical Therapy 14e
Management
Goal Hierarchy
- Treat reversible underlying cause (e.g., antiviral therapy for HCV/HBV, alcohol abstinence)
- Prevent/treat complications
- Bridge to or achieve liver transplantation (gold standard for cirrhotic portal hypertension)
Medical Management
| Drug | Mechanism | Use |
|---|---|---|
| Non-selective β-blockers (propranolol, nadolol, carvedilol) | Reduce cardiac output (β₁) + splanchnic vasoconstriction (β₂) → lower portal inflow | Primary & secondary prophylaxis of variceal bleeding |
| Diuretics (spironolactone ± furosemide) | Counter RAAS-driven Na⁺ retention | Ascites management |
| Vasopressin analogues (terlipressin, octreotide) | Splanchnic vasoconstriction | Acute variceal hemorrhage |
A ≥20% reduction in HVPG (or to <12 mmHg) with β-blockers correlates with reduced bleeding risk.
Endoscopic Management
- Esophageal variceal ligation (EVL): preferred over sclerotherapy for acute variceal bleeding and secondary prophylaxis
- Sclerotherapy: injection of sclerosing agents; higher complication rate (perforation, stricture, infection)
Interventional / Surgical Management
TIPS (Transjugular Intrahepatic Portosystemic Shunt):
- Catheter placed via jugular vein; stent connects a hepatic vein branch to a portal vein branch
- Effectively reduces portal pressure; has largely replaced surgical shunting
- Risk: hepatic encephalopathy (shunts blood away from liver), stent stenosis
Surgical Shunts (reserved for TIPS failures or select patients):
| Shunt Type | Description | Notes |
|---|---|---|
| Portacaval shunt (non-selective) | Portal vein → IVC | High encephalopathy risk; poor overall mortality benefit |
| Distal splenorenal shunt (Warren shunt) | Distal splenic vein → left renal vein | Selective; >90% efficacy; lower encephalopathy vs non-selective; contraindicated with massive ascites |
| Rex shunt (meso-left portal bypass) | SMV → intrahepatic left portal vein | Mainly pediatric extrahepatic portal vein obstruction |
The Warren shunt is the preferred selective shunt — it decompresses gastroesophageal varices while preserving mesenteric portal perfusion of the liver, thereby reducing hepatic encephalopathy rates.
Liver Transplantation: the only definitive cure for cirrhotic portal hypertension; addresses both the hemodynamics and the underlying liver disease.
Prognosis
- Compensated cirrhosis (HVPG 5–10 mmHg): can be asymptomatic for ≥10 years
- Once CSPH (HVPG ≥10 mmHg) develops → high decompensation risk
- After first decompensation: median survival <2 years without transplantation — Harrison's 22E
Sources:
- Harrison's Principles of Internal Medicine 22E, Ch. 355
- Sleisenger & Fordtran's Gastrointestinal and Liver Disease, Chs. 74 & 93
- Current Surgical Therapy 14e, "Portal Hypertension: Role of Shunting Procedures"
- Medical Physiology (Boron & Boulpaep)
This is a shared conversation. Sign in to Orris to start your own chat.