Ventilation perfusion inequality full details for md exams 10 marks answer
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
I now have all the core content and images needed for a comprehensive, exam-quality answer. Let me compose the full response.
Ventilation-Perfusion (V/Q) Inequality
Definition
Ventilation-perfusion (V/Q) inequality refers to the uneven matching of alveolar ventilation (VA) to pulmonary blood flow (Q) within different regions of the lung. It is by far the most common cause of hypoxemia in clinical practice and also a major contributor to hypercapnia in chronic lung disease.
- Normal overall V/Q ratio = ~0.8 (VA ~4.2 L/min; Q ~5.5 L/min)
- In a perfect lung, every alveolus would have V/Q = 0.8
- In reality, even normal lungs show regional V/Q variation due to gravity; disease dramatically amplifies this
Physiological Basis: The V/Q Spectrum
Each lung unit's alveolar PO2 and PCO2 are uniquely determined by its local V/Q ratio. The two extremes define the spectrum:
| V/Q | Condition | Alveolar gas approaches | Outcome |
|---|---|---|---|
| 0 | No ventilation (shunt) | Mixed venous blood (PO2 ~40 mmHg, PCO2 ~45 mmHg) | Deoxygenated blood enters systemic circulation |
| Normal (~0.8-1.0) | Ideal matching | Normal alveolar PO2 ~100 mmHg, PCO2 ~40 mmHg | Normal gas exchange |
| Infinity (∞) | No blood flow (dead space) | Inspired air (PO2 ~150 mmHg, PCO2 ~0 mmHg) | Wasted ventilation |
Effect of V/Q ratio on blood gases (from Murray & Nadel's, Figure 10.18):
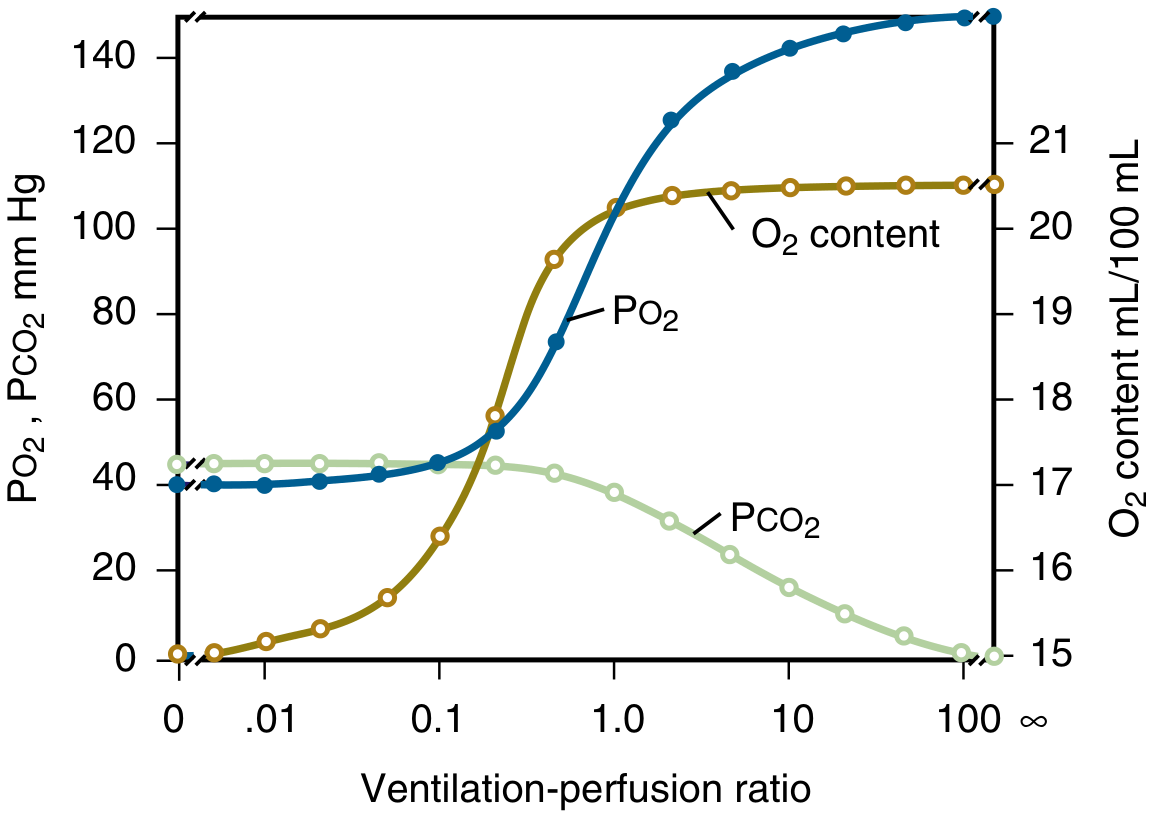
As V/Q ratio rises from 0 to infinity: PO2 rises from ~40 to ~150 mmHg, PCO2 falls from ~45 to 0 mmHg. Crucially, O2 content plateaus quickly (because Hb is already near-fully saturated at normal V/Q), while PCO2 falls linearly - this asymmetry is central to why V/Q inequality causes hypoxemia but not always hypercapnia.
Normal V/Q Variation Due to Gravity
In the upright lung, both ventilation and perfusion increase from apex to base, but perfusion increases more steeply than ventilation:
- Apex: High V/Q (~3.3) - well-ventilated, poorly perfused. Alveolar PO2 is high (~130 mmHg), PCO2 is low (~28 mmHg). Acts like dead space.
- Base: Low V/Q (~0.6) - relatively poorly ventilated, more heavily perfused. Alveolar PO2 is lower (~89 mmHg), PCO2 higher (~42 mmHg). Acts like a shunt.
- Net effect on arterial PO2: reduces it by only ~4 mmHg in a healthy lung
Why V/Q Inequality Causes Hypoxemia (Mechanism)
The key is the non-linearity of the oxygen-haemoglobin dissociation curve:
In the uncompensated model (Ganong, Figure 35-11 below):
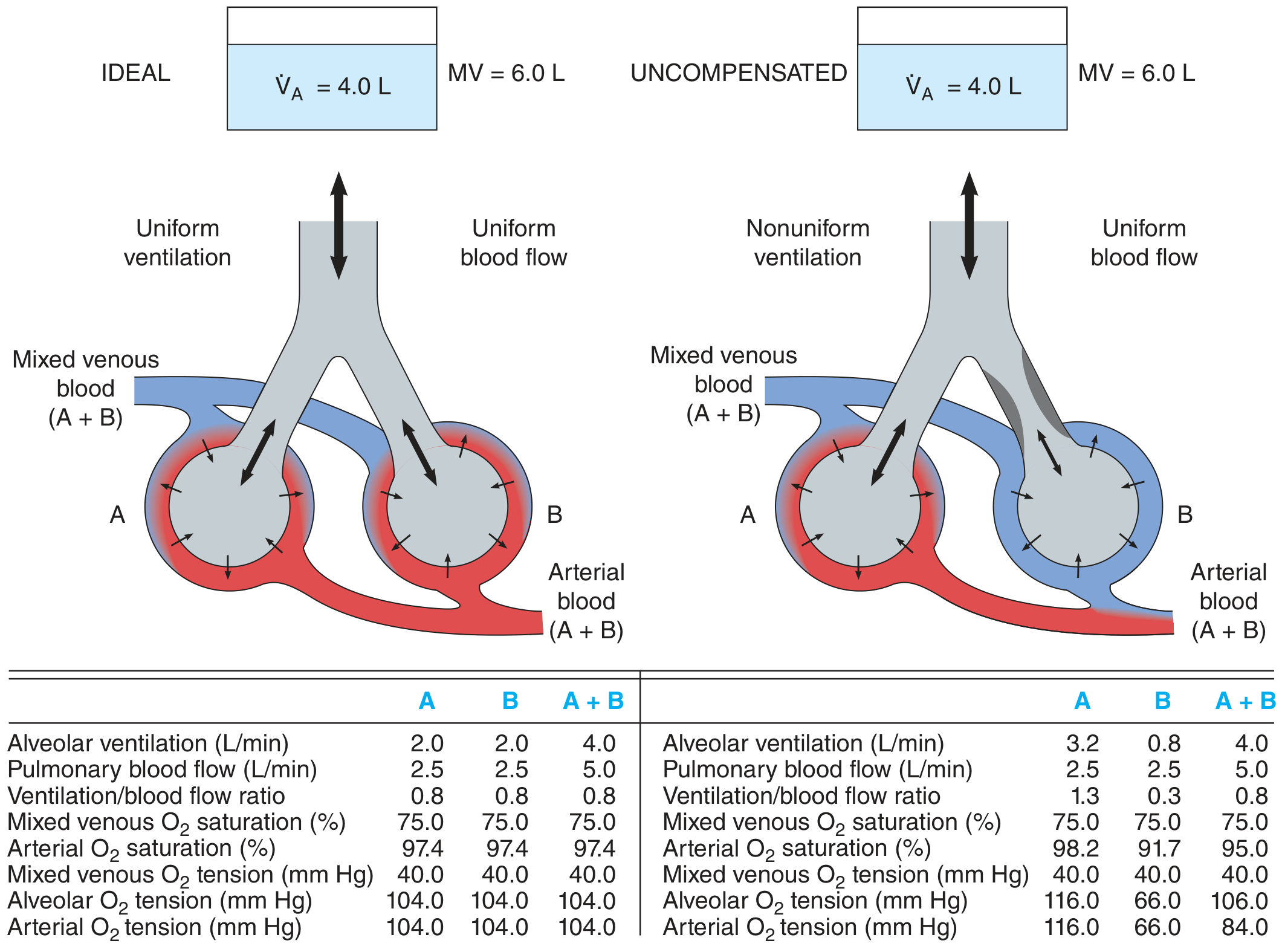
- Alveolus A (overventilated, V/Q = 1.3): PO2 = 116 mmHg, SaO2 = 98.2%
- Alveolus B (underventilated, V/Q = 0.3): PO2 = 66 mmHg, SaO2 = 91.7%
- Mixed arterial O2 saturation = 95% (hypoxaemic) - even though overall VA and Q are unchanged
The overventilated alveolus cannot compensate for the underventilated one because:
- Haemoglobin is already ~98% saturated at a PO2 of 104 mmHg (flat part of curve) - raising PO2 further adds negligible O2 content
- Blood from the underventilated alveolus pulls the mixed saturation down significantly (steep part of curve)
This asymmetry is the key mechanism of hypoxaemia in V/Q inequality.
Why V/Q Inequality Causes Hypercapnia (or Why It Often Does NOT)
The CO2 dissociation curve is nearly linear in the physiological range. This means:
- Overventilated units can increase CO2 elimination proportionally
- Underventilated units retain CO2, but the overventilated ones can compensate
In practice: V/Q inequality initially causes both hypoxaemia AND hypercapnia. However, rising PCO2 stimulates peripheral/central chemoreceptors, increasing ventilatory drive. The increased alveolar ventilation normalises PCO2 - but at the cost of further increasing V/Q dispersion ("wasted ventilation" to high V/Q dead-space units).
Result: Most patients with V/Q inequality have:
- Hypoxaemia (cannot be compensated by increased ventilation due to flat ODC)
- Normal or low arterial PCO2 (compensated by hyperventilation)
- Only in severe/advanced disease does hypercapnia supervene
The O2-CO2 Diagram (Riley Analysis)
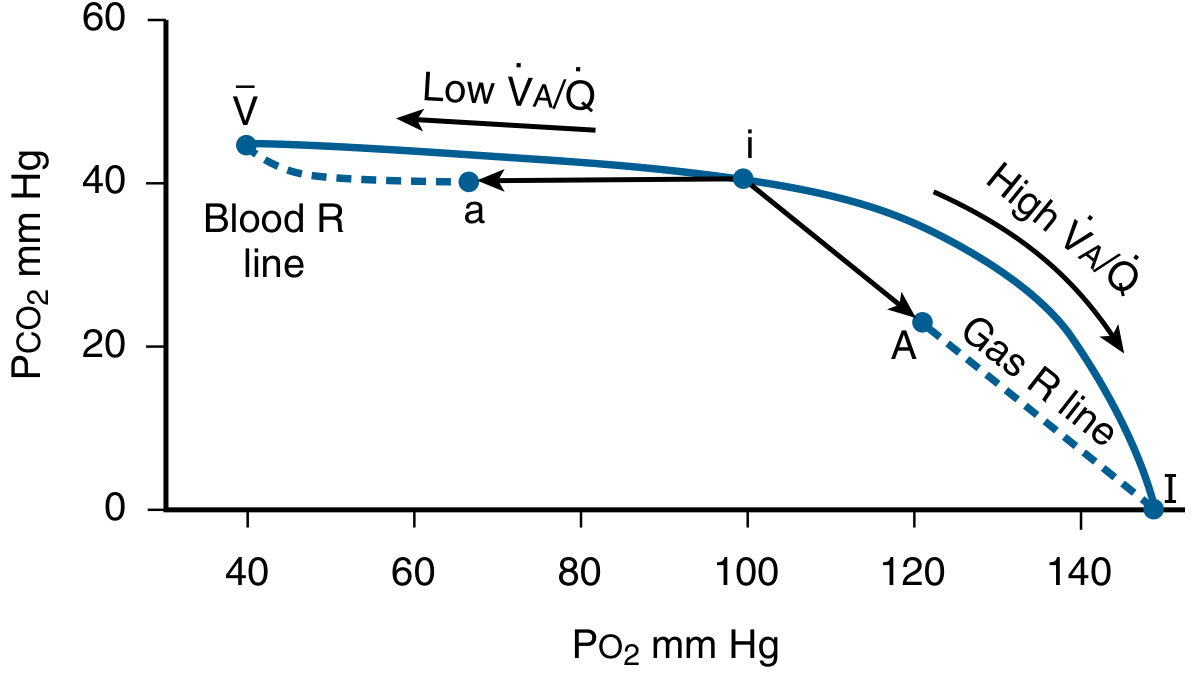
The O2-CO2 diagram shows the "ventilation-perfusion line" joining:
- Mixed venous blood (V-bar): PO2 ~40 mmHg, PCO2 ~45 mmHg
- Inspired air (I): PO2 ~150 mmHg, PCO2 ~0
All lung units in steady state must have their PO2/PCO2 on this line.
With V/Q inequality imposed:
- Point i (ideal): where arterial blood and alveolar gas would sit with perfect matching
- Point a (arterial blood): shifts LEFT toward mixed venous (lower PO2, slightly higher PCO2)
- Point A (alveolar gas): shifts RIGHT toward inspired air (higher PO2, lower PCO2)
- Result: Alveolar-arterial PO2 difference (A-a gradient) increases - the hallmark of V/Q inequality
Assessment of V/Q Inequality
1. Arterial PO2
- The lower the PaO2, the greater the mismatch (in general)
- Limitation: sensitive to overall ventilation, cardiac output, and inspired O2
2. Alveolar-Arterial PO2 Difference (A-a Gradient)
- Normal A-a gradient = ~5-15 mmHg (increases with age)
- Formula: A-a gradient = PAO2 - PaO2
- PAO2 = PIO2 - (PaCO2/R) [Alveolar gas equation]
- Increased A-a gradient = V/Q mismatch, shunt, or diffusion limitation
- A-a gradient is more informative than PaO2 alone because it is less sensitive to hypoventilation
- Key point: V/Q inequality increases the A-a gradient; pure hypoventilation does NOT significantly increase the A-a gradient
3. Physiologic Dead Space (VD/VT - Bohr equation)
- VD/VT = (PaCO2 - PECO2) / PaCO2
- High V/Q units (poorly perfused) are functional dead space
- Normal VD/VT ~0.30; elevated in obstructive lung disease
4. Physiologic Shunt (Venous Admixture)
- Qs/Qt = (CcO2 - CaO2) / (CcO2 - CvO2)
- Represents effect of low V/Q units (and true shunt) combined
- Normal physiologic shunt ~2-5%
5. Multiple Inert Gas Elimination Technique (MIGET)
- Gold standard for quantifying V/Q distributions
- Infuses 6 inert gases of differing solubility; measures retention in arterial blood and excretion in expired gas
- Can identify true shunt (V/Q = 0), dead space (V/Q = ∞), and the full distribution of V/Q ratios
- Too complex for routine clinical use but invaluable in research
V/Q Distribution Patterns in Disease
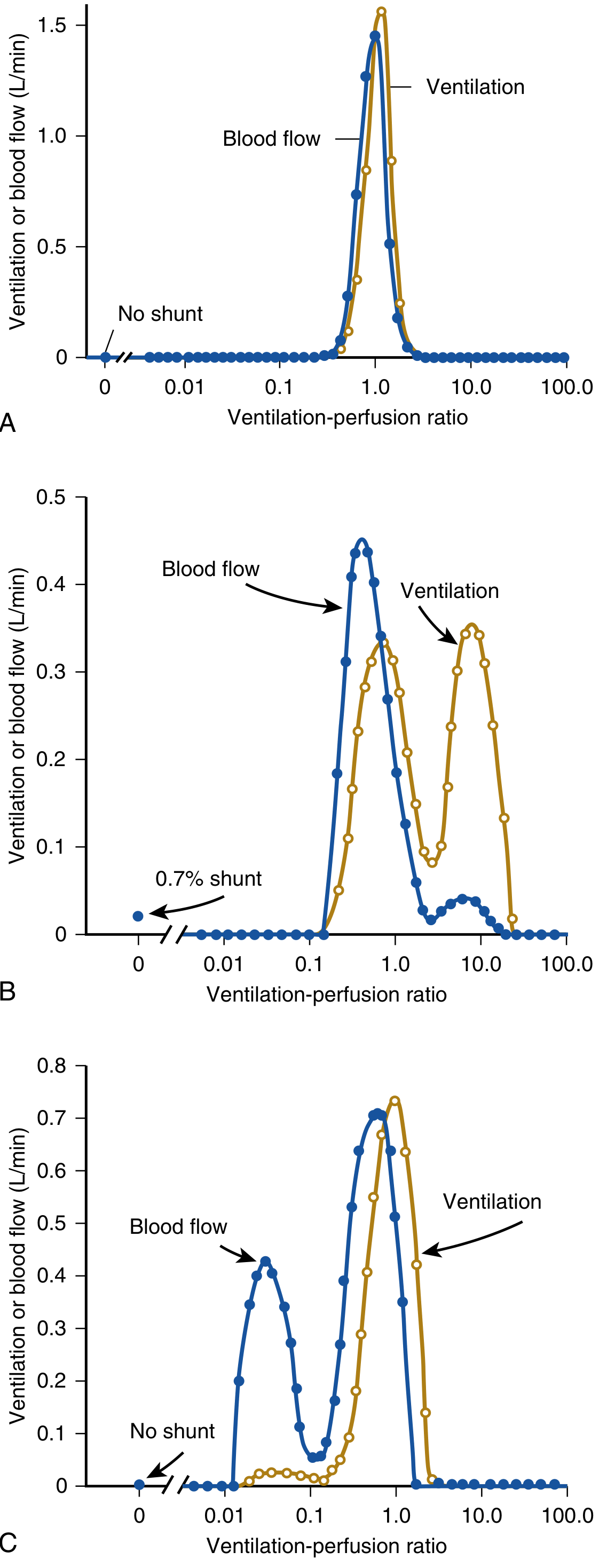
Figure: (A) Normal lung - narrow, unimodal distribution centered at V/Q ~1. (B) Emphysema-type COPD - bimodal with high V/Q areas (dead-space effect). (C) Bronchitis-type COPD - bimodal with low V/Q areas (shunt effect), causing more severe hypoxaemia.
| Disease | V/Q Pattern | Dominant Mechanism |
|---|---|---|
| COPD (bronchitis) | Low V/Q units (V/Q 0.005-0.1) | Airway obstruction, retained secretions |
| COPD (emphysema) | High V/Q units (wasted ventilation) | Alveolar destruction, capillary loss |
| Asthma | Low V/Q (reversible) | Bronchoconstriction, mucus plugging |
| Pulmonary embolism | High V/Q (dead space) | Obstruction of perfusion |
| Pneumonia/collapse | True shunt (V/Q = 0) | No ventilation to consolidated alveoli |
| Pulmonary fibrosis | Diffusion + low V/Q | Fibrosis + V/Q mismatch |
| CCF/pulmonary oedema | Low V/Q, shunt | Fluid-filled alveoli |
Effect of Cardiac Output on V/Q Inequality
- In a normal lung (no inequality): cardiac output has no effect on PaO2 or PaCO2
- In a diseased lung with V/Q inequality:
- Reduced cardiac output (e.g. myocardial infarction): lowers mixed venous PO2 → when this blood transits low V/Q regions, it exaggerates hypoxaemia disproportionate to the V/Q inequality itself
- Elevated cardiac output (e.g. asthma with beta-agonist use): raises mixed venous PO2 → "hides" degree of V/Q inequality, arterial PO2 is higher than expected
Response to Supplemental Oxygen (Key Exam Point)
| Cause of Hypoxaemia | Response to 100% O2 |
|---|---|
| V/Q inequality (low V/Q) | PaO2 rises substantially - O2 eventually reaches underventilated units |
| True anatomic shunt | PaO2 rises very little - blood bypasses all alveoli |
| Hypoventilation | PaO2 rises |
| Diffusion limitation | PaO2 rises |
This is a critical distinguishing feature: V/Q inequality responds to supplemental O2, while true shunts do not, because shunted blood never passes ventilated alveoli.
Summary of Key Points (Murray & Nadel's Key Points)
- V/Q inequality is the most common cause of hypoxaemia in lung disease
- V/Q ratios range from 0 (shunt = mixed venous composition) to infinity (dead space = inspired air composition)
- Hypoxaemia from V/Q inequality results from the non-linearity of the O2-Hb dissociation curve - high V/Q units cannot compensate for low V/Q units
- V/Q inequality impairs exchange of all gases (O2, CO2, CO, anaesthetic agents)
- Pure V/Q inequality causes both hypoxaemia and hypercapnia, but CO2 is usually normalised by compensatory hyperventilation; hypoxaemia cannot be similarly corrected
- The A-a gradient is the standard clinical measure; MIGET is the research gold standard
- Cardiac output modulates the severity of hypoxaemia through its effect on mixed venous PO2
- Two causes of hypercapnia: hypoventilation and V/Q inequality
- Five causes of hypoxaemia: decreased FiO2, hypoventilation, diffusion limitation, shunt, and V/Q inequality (the most common clinically)
Sources: Ganong's Review of Medical Physiology, 26th Ed., pp. 636, 650-651; Murray & Nadel's Textbook of Respiratory Medicine, Chapter 10 (Ventilation-Perfusion Relationships), pp. 237-245
Pls give me how to write in exam how many times to tell I don't want answer for knowledge just marks fetching
How to Write V/Q Inequality in MD Exam for Maximum Marks
Here's the exact structure - write it like this, and you'll fetch full marks every time.
EXAM WRITING STRATEGY
Rule 1: Examiner reads the FIRST line and LAST line most carefully.
Rule 2: Headings = free marks. Never write a wall of text.
Rule 3: Write a definition + classify + mechanisms + clinical relevance. Done.
WRITE EXACTLY THIS STRUCTURE (10 marks = ~2.5-3 pages)
Introduction / Definition (2-3 lines max)
"Ventilation-perfusion (V/Q) inequality refers to non-uniform matching of alveolar ventilation to pulmonary blood flow in different lung regions. It is the most common cause of hypoxaemia in clinical practice."
One line. Bold the punchline. Move on.
Normal V/Q Ratio (3-4 lines)
- Normal overall V/Q = 0.8 (VA 4.2 L/min / Q 5.5 L/min)
- Apex: V/Q = 3.3 (over-ventilated, under-perfused)
- Base: V/Q = 0.6 (under-ventilated, over-perfused)
- One line: "This normal inequality due to gravity reduces PaO2 by only ~4 mmHg"
V/Q Spectrum (draw a small table - examiners LOVE tables)
| V/Q Ratio | Condition | Gas composition approaches |
|---|---|---|
| 0 | Shunt | Mixed venous blood (PO2 40, PCO2 45) |
| 0.8 | Normal | Normal alveolar gas |
| Infinity (∞) | Dead space | Inspired air (PO2 150, PCO2 0) |
Mechanism of Hypoxaemia (THIS is the heart - write clearly)
"Due to non-linearity of the oxygen-haemoglobin dissociation curve:"
- Low V/Q units → low alveolar PO2 → blood leaves under-saturated
- High V/Q units → high alveolar PO2 → but Hb already near 100% saturated → cannot compensate
- Mixed arterial blood → net hypoxaemia
One sentence examiner wants: "Overventilated alveoli cannot compensate for underventilated ones because haemoglobin is already on the flat portion of the dissociation curve."
Why PCO2 is Usually Normal (separate heading - instant marks)
"V/Q inequality causes initial hypercapnia, but rising PCO2 stimulates chemoreceptors → increased ventilatory drive → PCO2 normalised. However, hypoxaemia persists because increased ventilation to high V/Q (dead space) units cannot raise O2 content due to flat dissociation curve."
A-a Gradient (always mention - 1 mark guaranteed)
- A-a gradient = PAO2 - PaO2 (normal 5-15 mmHg)
- Hallmark of V/Q inequality = raised A-a gradient
- Pure hypoventilation → normal A-a gradient (distinguish!)
Diseases Causing V/Q Inequality (table again)
| Disease | Type of V/Q abnormality |
|---|---|
| COPD (bronchitis) | Low V/Q (shunt-like) |
| COPD (emphysema) | High V/Q (dead space) |
| Pulmonary embolism | High V/Q (dead space) |
| Pneumonia | True shunt (V/Q = 0) |
| Asthma | Low V/Q |
Response to O2 (one mark - one line)
"V/Q inequality corrects with 100% O2 (distinguishes it from true shunt, which does not respond)."
Conclusion (2 lines - always end with one)
"V/Q inequality is the dominant mechanism of hypoxaemia in virtually all chronic lung diseases. Understanding it is essential for interpreting blood gas results and planning oxygen therapy."
THE GOLDEN EXAM RULES
| What to do | Why |
|---|---|
| Bold the first sentence | Examiner scans for it |
| Use headings for every paragraph | Each heading = visual mark |
| Write at least 1 table | Shows organisation, fills space well |
| Mention A-a gradient explicitly | Almost always asked as a sub-point |
| End with clinical relevance | Examiner remembers last thing read |
| Write V/Q = 0.8, 3.3, 0.6 as numbers | Specific numbers signal mastery |
| Never write a paragraph longer than 4 lines | Long paragraphs look like rambling |
| Dedicate one heading to "Why not hypercapnia" | This is a classic trap - mention it = bonus mark |
Time budget for a 10-mark answer: 15-18 minutes. Target 2.5 pages. Stop there.
This is a shared conversation. Sign in to Orris to start your own chat.