Blood pressure in detail
Reading File
Finding Sources
Finding Sources
Searching PubMed
"blood pressure" AND "regulation"
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Reading File
Reading File
Loading Image
Now I have rich content from both Robbins Pathology and Katzung's Pharmacology. Let me compile a comprehensive, well-structured answer.
Blood Pressure - A Detailed Overview
1. Definition and Basic Formula
Blood pressure (BP) is the force exerted by circulating blood on the walls of blood vessels. It is governed by the hydraulic equation:
BP = Cardiac Output (CO) × Peripheral Vascular Resistance (PVR)
Both components are regulated through multiple overlapping neural, humoral, and local mechanisms to maintain pressure within the narrow range needed for adequate organ perfusion.
- Robbins & Kumar Basic Pathology, p. 309
- Katzung's Basic and Clinical Pharmacology, 16th Ed., p. 268
2. Normal Values
| Blood Pressure Category | Systolic (mmHg) | Diastolic (mmHg) |
|---|---|---|
| Low | 70-90 | 40-60 |
| Normal | 90-120 | 60-80 |
| Elevated | 120-129 | <80 |
| Hypertension Stage I | 130-139 | 80-90 |
| Hypertension Stage II | >140 | >90 |
| Malignant HTN | >180 | >120 |
Starting at 115/75 mmHg, cardiovascular disease risk doubles with each increment of 20/10 mmHg throughout the blood pressure range. - Katzung's, p. 268
3. Components of Blood Pressure
A. Cardiac Output
Cardiac output = stroke volume × heart rate.
- Stroke volume is primarily determined by filling pressure, which depends on sodium homeostasis and blood volume.
- Heart rate and contractility are controlled by α- and β-adrenergic systems.
- Blood volume is influenced by sodium, mineralocorticoids, and atrial natriuretic peptide (ANP).
B. Peripheral Vascular Resistance
Regulated mainly at the arteriole level by a balance of:
Vasoconstrictors:
- Angiotensin II
- Catecholamines (via α-adrenergic receptors)
- Endothelin-1
- Thromboxane, leukotrienes
Vasodilators:
- Nitric oxide (NO)
- Prostaglandins
- Kinins
- β-adrenergic stimulation
4. Regulatory Mechanisms
Here is the master diagram summarizing all factors governing blood pressure:
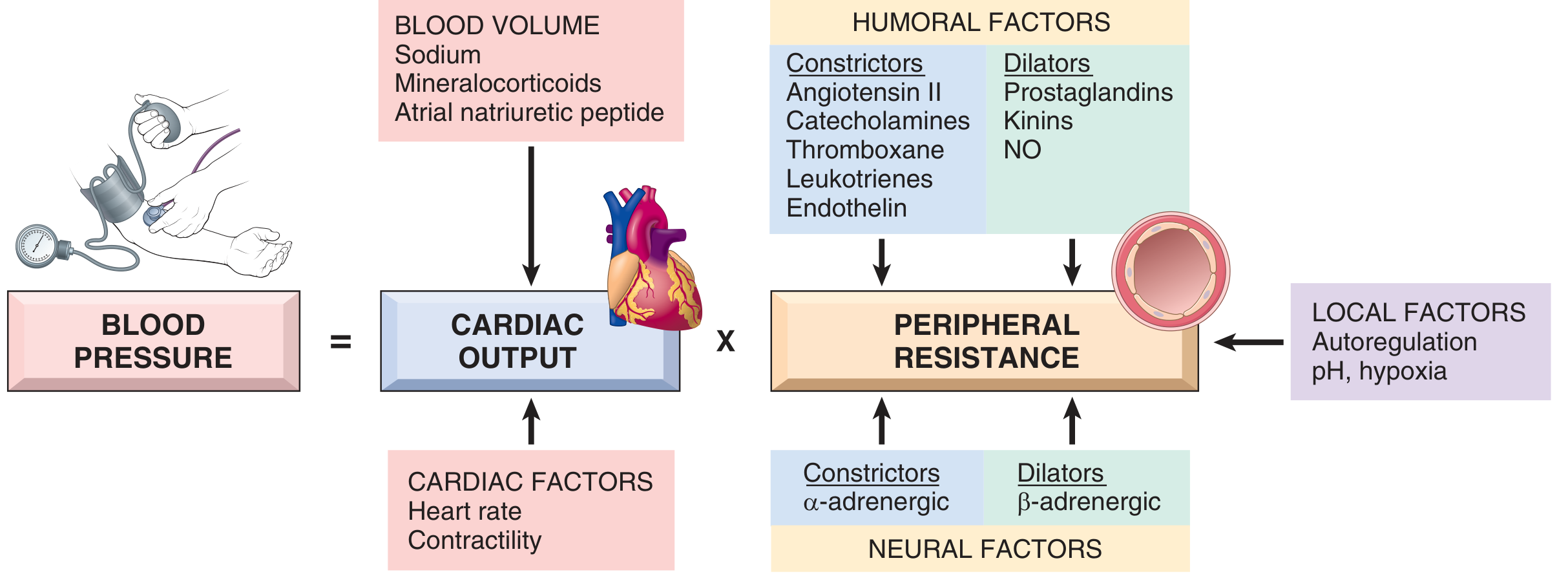
Fig. 8.2 - Blood Pressure Regulation. (Robbins & Kumar Basic Pathology)
The four anatomic control sites coordinated by the CNS are shown below:
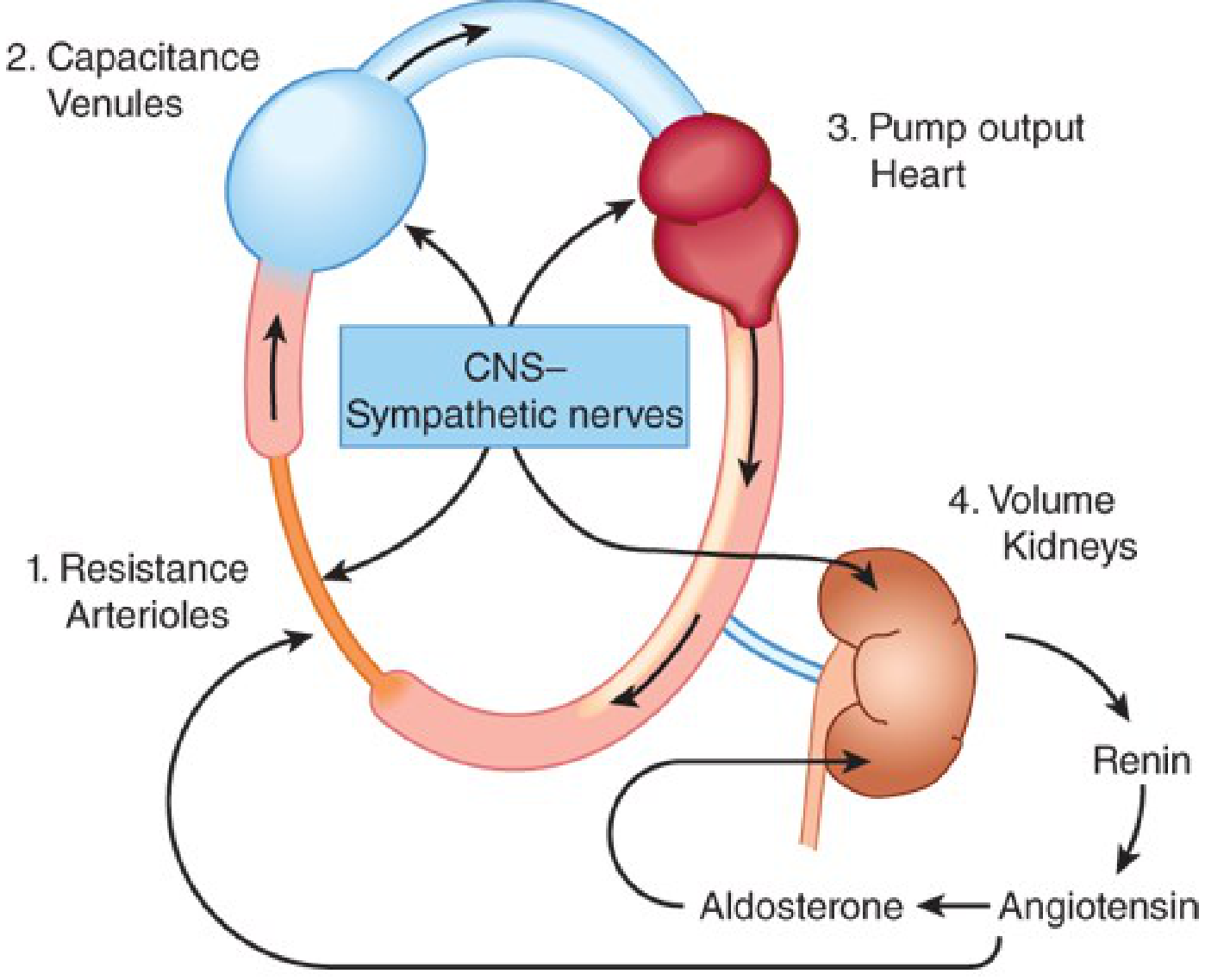
Fig. 11-1 - Anatomic sites of blood pressure control (Katzung's Pharmacology)
A. The Renin-Angiotensin-Aldosterone System (RAAS)
This is the primary long-term BP regulator:
- Renin - released by renal juxtaglomerular cells when renal perfusion pressure falls or sodium is low
- Renin cleaves angiotensinogen → Angiotensin I
- ACE (on vascular endothelium) converts it → Angiotensin II
- Angiotensin II acts by:
- Directly constricting arteriolar smooth muscle (↑ PVR)
- Stimulating aldosterone secretion from the adrenal cortex
- Increasing tubular sodium resorption directly
- Aldosterone increases Na+ (and water) resorption in the distal tubule → ↑ blood volume → ↑ CO
B. Baroreflex (Short-term, rapid regulation)
Carotid baroreceptors sense arterial wall stretch. When BP falls:
- Reduced baroreceptor firing → reduced inhibition of the medullary vasomotor center
- Increased sympathetic outflow → vasoconstriction (↑ PVR) + increased heart rate/contractility (↑ CO)
- This restores BP within seconds
When BP rises, the opposite occurs. In hypertensive patients, this baroreflex is reset to a higher set point. - Katzung's, p. 270
C. Renal Volume Control (Long-term)
- Reduced renal perfusion → salt and water retention → expanded blood volume → ↑ CO
- The kidney controls BP by regulating intravascular volume over days to weeks
- Vasopressin (ADH) from the posterior pituitary also contributes by regulating water reabsorption
D. Natriuretic Peptides (Counter-regulatory)
- ANP (from atria) and BNP (from ventricles) are released in response to volume expansion / elevated filling pressures
- They inhibit sodium resorption in distal renal tubules → natriuresis and diuresis
- They also cause systemic vasodilation
- Net effect: reduce blood volume and BP
E. Local Autoregulation
- Resistance vessels respond to increased blood flow with vasoconstriction to protect against hyperperfusion
- Tissue pH and hypoxia fine-tune local blood flow to match metabolic demands
5. Measurement
Blood pressure is expressed as systolic/diastolic in mmHg, measured via sphygmomanometry. Key points:
- Two readings are taken; the average is used
- "White coat hypertension" (elevated in office, normal at home) should be confirmed with ambulatory BP monitoring (ABPM) or home readings
- Hypertension is asymptomatic until end-organ damage is imminent - Katzung's, p. 268
6. Hypertension
Classification by Cause
| Type | Frequency | Examples |
|---|---|---|
| Primary (essential/idiopathic) | 90-95% | Multifactorial; no identifiable cause |
| Secondary | 5-10% | Renal artery stenosis, primary aldosteronism, pheochromocytoma, Cushing's, coarctation of aorta, obstructive sleep apnea |
Primary hypertension arises from a combination of: genetic factors, psychological stress, high dietary sodium, low potassium/calcium, alcohol consumption, obesity, and physical inactivity. - Robbins Pathology, p. 310
Risk Stratification
Additional risk factors that worsen prognosis at any BP level:
- Smoking (including secondhand)
- Diabetes mellitus
- Metabolic syndrome (obesity, dyslipidemia)
- Physical inactivity
- End-organ damage at diagnosis
- Family history of cardiovascular disease
- African American ethnicity (higher prevalence + severity)
- Male sex (premenopausal women are relatively protected)
Malignant Hypertension
- Systolic >180 mmHg or diastolic >120 mmHg
- Rapidly rising; leads to death within 1-2 years if untreated
- Associated with renal failure, retinal hemorrhages, papilledema
- Most commonly superimposed on pre-existing primary hypertension
7. Consequences of Hypertension
Without treatment, approximately:
- 50% of hypertensive patients die of ischemic heart disease or congestive heart failure
- 33% die of stroke
- Others develop aortic dissection, renal failure, multifocal dementia
Target organs damaged by sustained hypertension:
- Heart - left ventricular hypertrophy, heart failure
- Brain - stroke, hypertensive encephalopathy, vascular dementia
- Kidneys - nephrosclerosis, renal failure
- Eyes - retinopathy, retinal hemorrhages
- Arteries - accelerated atherosclerosis, aortic dissection
8. Antihypertensive Drug Classes
All antihypertensive drugs work by interfering with normal BP regulatory mechanisms at one or more of the four anatomic control sites:
- Diuretics - deplete sodium, reduce blood volume (e.g., hydrochlorothiazide, furosemide)
- RAAS blockers - ACE inhibitors, ARBs, direct renin inhibitors; reduce angiotensin II effect → vasodilation + reduced aldosterone
- Direct vasodilators - relax vascular smooth muscle (e.g., hydralazine, minoxidil)
- Sympathoplegic agents - reduce sympathetic outflow; subdivided by site of action:
- Central acting (e.g., clonidine, methyldopa)
- Ganglionic blockers
- β-blockers (reduce HR and CO)
- α-blockers (reduce PVR)
- Combined α/β blockers (e.g., labetalol)
- Calcium channel blockers - reduce vascular smooth muscle contraction
- Katzung's, p. 271
Sources:
- Robbins & Kumar Basic Pathology (Robbins Pathology), pp. 309-311
- Katzung's Basic and Clinical Pharmacology, 16th Ed., pp. 268-271
This is a shared conversation. Sign in to Orris to start your own chat.