Parkinson's disease in detailed
Reading File
Finding Sources
Searching PubMed
"Parkinson disease"[MeSH Terms] AND treatment
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Loading Image
Reading File
I now have comprehensive, well-sourced information from multiple authoritative textbooks. Let me compile the full detailed answer.
Parkinson's Disease - Detailed Overview
1. Definition and Overview
Parkinson's disease (PD) is a progressive neurodegenerative disorder and the second most common neurodegenerative disease after Alzheimer's disease. It is the most common cause of parkinsonism - a clinical syndrome defined by four cardinal signs: tremor, rigidity, akinesia (bradykinesia), and postural disturbances. PD occurs in approximately 1 in 1,000 in the general population and in at least 1% of persons over age 65. Men are affected slightly more often than women (3:2 ratio). Prevalence is increasing as the world population ages - age-adjusted mortality from PD increased by 2.4% per year between 1999 and 2019. - Goldman-Cecil Medicine, p. 3960
2. Etiology and Risk Factors
Genetic Causes (~10% of cases)
| Gene / Mutation | Inheritance | Notes |
|---|---|---|
| α-synuclein (SNCA) gene mutations, duplications, triplications | Autosomal dominant | Chief constituent of Lewy bodies |
| LRRK2 (Leucine-rich repeat kinase 2) | Autosomal dominant | Most common cause of AD-inherited PD |
| Parkin | Autosomal recessive | Typically early-onset PD |
| DJ-1 | Autosomal recessive | Early onset |
| PINK1 | Autosomal recessive | Early onset |
| GBA (glucocerebrosidase) | Risk gene | Associated with higher rates of dementia, faster motor progression |
| PARK10 (chromosome 1) | Complex | Strongly associated with PD |
Environmental Factors
- Pesticide exposure (rotenone, paraquat)
- Heavy metal exposure
- Traumatic brain injury (severe enough for an ED visit)
- Neurotoxin MPTP (1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine): selectively destroys dopaminergic neurons in the substantia nigra pars compacta by being oxidized to MPP+, which inhibits Complex I of the mitochondrial electron transport chain. This has strongly implicated oxidative stress in PD pathogenesis.
Other proposed pathogenetic factors: mitochondrial dysfunction, protein misfolding and aggregation, excitotoxicity, inflammation, apoptotic cell death, and loss of trophic support. - Goldman-Cecil Medicine, p. 3960
3. Pathophysiology
The Dopamine-Acetylcholine Imbalance
The core mechanism involves destruction of dopaminergic neurons in the substantia nigra pars compacta, with consequent loss of dopamine in the neostriatum (especially the putamen).
- Normally, dopaminergic neurons project from the substantia nigra to the neostriatum (nigrostriatal pathway), providing tonic inhibitory dopaminergic input that suppresses excitatory cholinergic neurons.
- GABA-ergic neurons from the neostriatum project back to the substantia nigra providing reciprocal inhibition.
- In PD, about 60% of dopaminergic neurons degenerate before classic motor features develop.
- Loss of dopamine removes the inhibitory influence on cholinergic neurons, resulting in relative overactivity of acetylcholine in the neostriatum.
- This triggers abnormal signaling through basal ganglia circuits, ultimately increasing inhibitory output from the globus pallidus internus (GPi) and substantia nigra pars reticulata to the thalamus, impairing thalamocortical drive and motor facilitation.
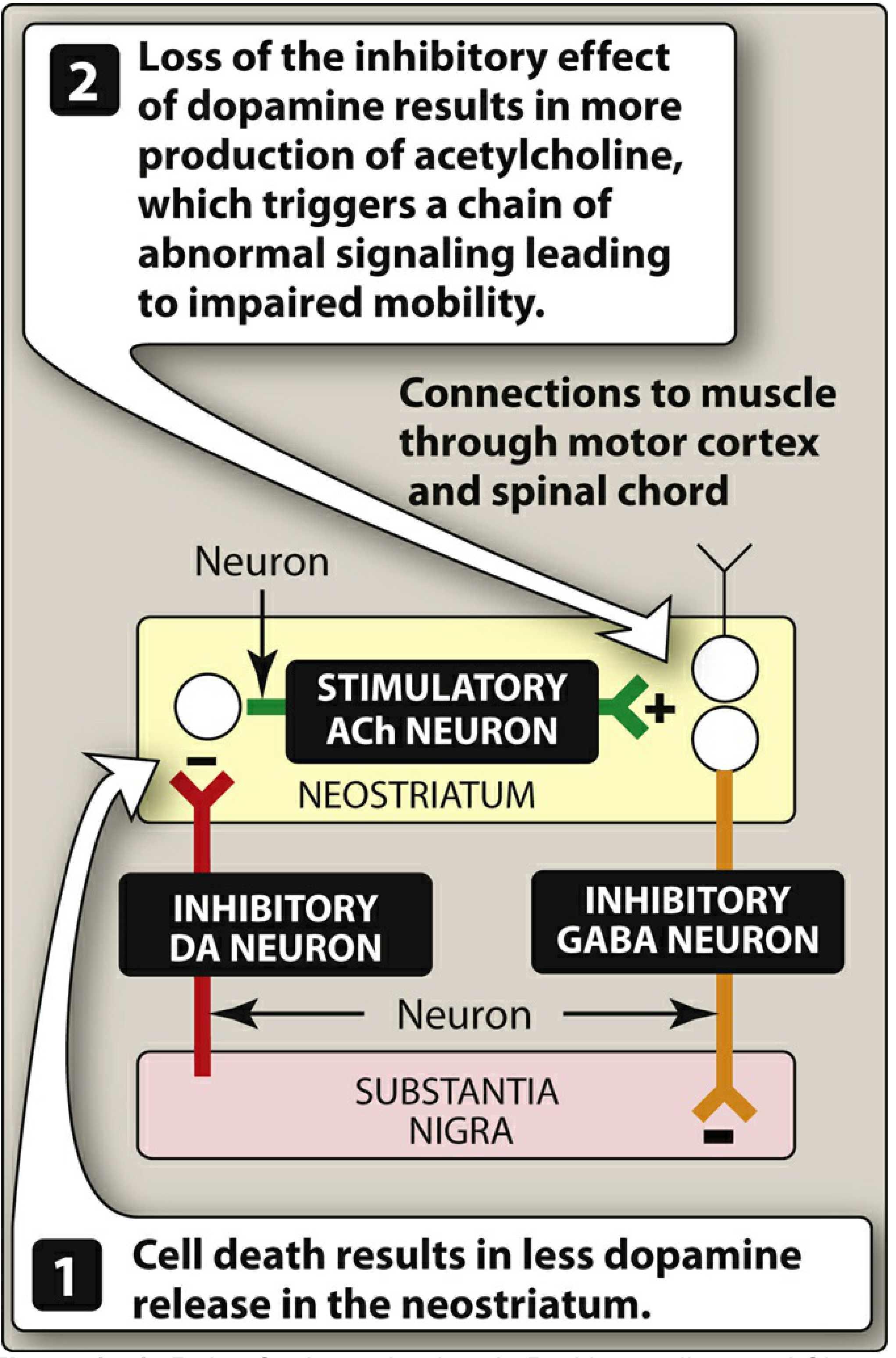
Figure: Role of substantia nigra in Parkinson's disease - Lippincott's Pharmacology
Treatment strategy is therefore aimed at:
- Restoring dopamine in the basal ganglia (dopaminergic drugs)
- Antagonizing excitatory cholinergic neurons (anticholinergic drugs)
Braak Staging - Disease Spread
PD likely begins in the lower brain stem and olfactory system (causing early anosmia), then progresses to the substantia nigra, and later involves cortical regions. Cell-to-cell transmission of toxic α-synuclein in a "permissive templating" (prion-like) fashion drives disease progression. - Goldman-Cecil Medicine, p. 3961
The Lewy Body
The hallmark pathologic inclusion is the Lewy body - a cytoplasmic inclusion in dopaminergic neurons composed predominantly of aggregated α-synuclein. Lewy bodies have a dense eosinophilic (pink) center with a lighter halo and are found in the cytoplasm of pigmented neurons in the substantia nigra.
4. Clinical Features
Prodromal / Premotor Phase
The disease begins years before motor symptoms appear, in the prodromal phase:
- REM sleep behavior disorder (RBD) - acting out dreams
- Olfactory dysfunction / anosmia - loss of smell
- Constipation (enteric nervous system involvement)
- Autonomic dysfunction
- Depression and anxiety
- Restless legs syndrome
Motor Symptoms (The Four Cardinal Signs)
Symptoms typically begin asymmetrically - one limb or one side. This asymmetry often persists into later stages.
1. Tremor
- Classic resting tremor at 4-6 Hz with characteristic "pill-rolling" quality
- Present at rest; diminishes or disappears with voluntary movement
- Accentuated by stress (e.g., mental calculations)
- Present in upper limbs while walking
- Occurs in only ~20% of patients initially but is virtually pathognomonic when present
- A higher-frequency (7-10 Hz) postural/kinetic tremor is also common
2. Rigidity
- Increased muscle tone on passive movement
- Cogwheel rigidity - when tremor is superimposed (ratchet-like catch)
- Lead pipe rigidity - uniform resistance without tremor
- Activated by contralateral limb movement
- Patients complain of stiffness
3. Akinesia / Bradykinesia
The most disabling feature. Includes:
- Hypomimia / masked facies - reduced facial expression, reptilian stare
- Hypophonia - soft, monotonous speech
- Sialorrhea (drooling) - impaired swallowing
- Micrographia - small handwriting
- Reduced arm swing while walking
- Shuffling gait with shortened stride
- Freezing of gait - sudden arrest of walking
- Difficulty arising from low chairs; difficulty turning in bed
- Tested clinically by finger tapping, fist opening/closing, wrist pronation/supination
4. Postural Disturbances
- Stooped posture (flexed trunk and limbs)
- Postural instability - impaired righting reflexes, falls
- Festination - involuntary propulsive acceleration
- Propulsion (forward) and retropulsion (backward)
- Assessed by the pull test (examiner pulls patient backward from the shoulders)
Non-Motor Symptoms (Later Stage)
| System | Manifestations |
|---|---|
| Autonomic | Orthostatic hypotension, urinary urgency/frequency, constipation, male erectile dysfunction, seborrhea |
| Neuropsychiatric | Depression, anxiety, apathy, visual hallucinations, paranoid psychosis, impulse control disorders |
| Cognitive | Mild cognitive impairment → dementia (in up to 80% over time) |
| Sleep | REM sleep behavior disorder, excessive daytime sleepiness, insomnia |
| Sensory | Pain, olfactory dysfunction, restless legs |
| Speech/Swallowing | Dysarthria, dysphagia (aspiration risk - found in 82% on objective testing) |
5. Diagnosis
PD is a clinical diagnosis. No definitive biomarker or test exists for sporadic PD.
Diagnostic Criteria (UK Brain Bank)
- Bradykinesia, plus at least one of: muscular rigidity, resting tremor (4-6 Hz), postural instability
- Exclusion criteria (features suggesting alternative diagnoses)
- Supportive criteria (asymmetric onset, sustained response to levodopa, rest tremor, progressive course)
Investigations
- Brain MRI - to exclude structural causes; usually normal in PD
- DaTSCAN (dopamine transporter SPECT scan) - shows reduced dopamine transporter uptake in the striatum; supports diagnosis but cannot distinguish PD from other synucleinopathies
- Genetic testing - appropriate for patients with family history, early onset, or clinical interest
- Assessment for prodromal features: olfactory testing, polysomnography for RBD
Red Flags Suggesting Alternative Diagnosis (Atypical Parkinsonism)
- Early falls, early dementia, early autonomic failure
- Rapid progression
- Poor or no response to levodopa
- Symmetric onset
- Cerebellar signs, vertical gaze palsy (suggests PSP)
- Prominent dysautonomia (suggests MSA)
6. Differential Diagnosis of Parkinsonism
| Category | Conditions |
|---|---|
| Parkinson disease | Sporadic (90%), genetic (10%) |
| Atypical parkinsonian syndromes ("Parkinson-plus") | Progressive supranuclear palsy (PSP), Multiple system atrophy (MSA), Corticobasal degeneration (CBD), Dementia with Lewy bodies (DLB) |
| Drug-induced | Antipsychotics (dopamine receptor blockers: haloperidol, phenothiazines), metoclopramide, reserpine |
| Toxic | MPTP, manganese, carbon monoxide |
| Vascular | Multi-infarct "vascular parkinsonism" |
| Metabolic | Wilson's disease (copper), manganism |
| Infectious | Post-encephalitic parkinsonism |
| Structural | Normal pressure hydrocephalus, brain tumors |
Goldman-Cecil Medicine, Table 378-1
7. Treatment
General Principles
Treatment is currently symptomatic - no disease-modifying therapy exists. Goals: maintain quality of life, functional independence, and minimize complications. All available drugs provide only temporary relief and do not arrest neuronal degeneration. - Lippincott Pharmacology
A. Levodopa + Carbidopa (First-line)
Mechanism:
- Levodopa is the metabolic precursor of dopamine. It crosses the blood-brain barrier (dopamine cannot), and surviving neurons in the substantia nigra convert it to dopamine.
- Carbidopa inhibits peripheral dopa-decarboxylase, preventing levodopa breakdown in peripheral tissues. This reduces the required levodopa dose by 4-5 fold and decreases peripheral side effects (nausea, cardiac arrhythmias, hypotension).
Efficacy:
- Most effective symptomatic treatment for PD
- Effective for bradykinesia, rigidity, and tremor
- In ~2/3 of patients, substantially reduces symptoms for first few years
- Even after 20+ years of disease, most classic motor features continue to respond
Complications with Long-Term Use:
- Wearing-off ("end-of-dose deterioration") - symptom return before next dose, typically within 2-5 years
- On-off fluctuations - unpredictable swings between mobile ("on") and immobile ("off") states
- Peak-dose dyskinesias - involuntary choreiform/athetoid movements at peak plasma levels
- Diphasic dyskinesias - at beginning and end of dose effect
- Off-period dystonia - painful foot/leg dystonia in the morning
- Psychiatric - vivid dreams, hallucinations, confusion, psychosis
Management of motor fluctuations:
- Increase dosing frequency
- Controlled-release levodopa formulations
- COMT inhibitors (entacapone, opicapone)
- MAO-B inhibitors
- Inhaled levodopa (works within 10 min for sudden "off" episodes)
- Continuous duodenal infusion (for advanced cases)
B. Dopamine Agonists
Drugs: Pramipexole, Ropinirole, Rotigotine (transdermal patch), Apomorphine (injectable/sublingual), Bromocriptine (ergot - less used now)
- Longer duration of action than levodopa
- Used as initial monotherapy in younger patients (<65 yrs, cognitively intact) to delay levodopa
- Added to levodopa for motor fluctuations
- Less dyskinesia than levodopa when used as initial therapy
Adverse effects: Nausea, orthostatic hypotension, excessive somnolence, hallucinations, confusion, impulse control disorders (compulsive gambling, hypersexuality, binge eating, excessive spending) - Lippincott Pharmacology
Bromocriptine (ergot): additional risks of pulmonary/retroperitoneal fibrosis, vasospasm
Rotigotine: once-daily transdermal patch providing stable drug levels over 24 hours
Apomorphine: used for acute "off" episode rescue in advanced PD
C. MAO-B Inhibitors
Drugs: Selegiline, Rasagiline, Safinamide
- Inhibit monoamine oxidase type B, reducing dopamine breakdown in the brain
- Used as early monotherapy for mild symptoms or added to levodopa to extend "on" time
- Selegiline is metabolized to amphetamine/methamphetamine metabolites (potential stimulant effects, insomnia)
D. COMT Inhibitors
Drugs: Entacapone, Opicapone, Tolcapone
- Inhibit catechol-O-methyltransferase, reducing peripheral degradation of levodopa
- Extend the duration of levodopa effect; reduce wearing-off
- Always used in combination with levodopa
- Tolcapone: rare hepatotoxicity - requires liver function monitoring
E. Amantadine
- Antiviral drug with weak antiparkinsonism properties
- Mechanisms: potentiates dopaminergic function, NMDA receptor antagonism (antidyskinetic effect), adenosine A2A receptor antagonism
- Useful for mild early symptoms and for reducing levodopa-induced dyskinesias
- Available in immediate-release and extended-release (Gocovri, Osmalex) formulations
- Side effects: livedo reticularis, peripheral edema, hallucinations, confusion, psychosis, insomnia, heart failure
- Do not stop abruptly - may cause confusional state, hyperpyrexia, acute worsening
F. Istradefylline
- Adenosine A2A receptor antagonist (caffeine analog)
- Reduces "off" periods when added to carbidopa-levodopa
- Oral: 20-40 mg daily
- Side effects: dyskinesias, hallucinations, impulsive behaviors
G. Anticholinergic Drugs
Drugs: Trihexyphenidyl, Benztropine
- Block muscarinic receptors; restore dopamine-ACh balance
- Improve tremor and rigidity but little effect on bradykinesia
- Primarily used in younger patients with tremor-predominant disease
- Side effects: dry mouth, urinary retention, constipation, blurred vision, confusion, memory impairment (avoid in elderly)
H. Surgical Treatment - Deep Brain Stimulation (DBS)
Indicated for patients with:
- Advanced PD with motor fluctuations/dyskinesias not adequately controlled by medication
- Good general health and cognitive function
- Age typically <75 years (for STN DBS)
Targets:
| Target | Advantages |
|---|---|
| STN (Subthalamic nucleus) | Larger benefit in "off" state; greater dopaminergic medication reduction; slightly higher neuropsychiatric risk |
| GPi (Globus pallidus internus) | Better dyskinesia suppression; better long-term flexibility; safer neuropsychiatric profile; preferred for "brittle" dyskinesias |
Both STN and GPi DBS show similar overall motor outcomes. DBS does not slow disease progression. - Bradley and Daroff's Neurology, p. 652
I. Other Physical and Supportive Therapies
- Physiotherapy - gait training, balance exercises, reducing fall risk
- Speech therapy - LSVT LOUD for hypophonia; swallowing management
- Occupational therapy - adaptive devices
- Dietary counseling - protein timing with levodopa (amino acids compete for absorption)
- rTMS - investigational; some evidence of modest motor improvement via modulation of motor cortex excitability and potential dopamine release
8. Disease Progression and Prognosis
- PD is slowly progressive over decades
- Motor complications (wearing off, dyskinesias) develop in ~50% of patients within 2-5 years of levodopa initiation
- Later-stage disease is characterized by treatment-resistant symptoms:
- Freezing of gait, postural instability, falls
- Cognitive decline and dementia
- Severe dysautonomia
- Dysphagia and aspiration pneumonia (leading cause of death)
- Dementia ultimately develops in a high proportion of patients over time
- Life expectancy is modestly reduced, mainly from aspiration pneumonia, falls, and immobility complications
9. Summary Table of Drug Classes
| Drug Class | Example(s) | Mechanism | Main Use |
|---|---|---|---|
| Levodopa/Carbidopa | Sinemet | Dopamine precursor + peripheral DDC inhibitor | First-line, most effective |
| Dopamine agonists | Pramipexole, Ropinirole, Rotigotine | D2/D3 receptor agonists | Early PD, adjunct therapy |
| MAO-B inhibitors | Rasagiline, Selegiline | Reduce dopamine breakdown | Early/adjunct therapy |
| COMT inhibitors | Entacapone, Opicapone | Reduce levodopa degradation | Reduce wearing-off |
| NMDA antagonist | Amantadine | Dopaminergic + anti-glutamate | Dyskinesias, mild symptoms |
| A2A antagonist | Istradefylline | Adenosine receptor block | Adjunct to reduce "off" time |
| Anticholinergics | Trihexyphenidyl | Muscarinic blockade | Tremor (young patients) |
| DBS | STN or GPi | Basal ganglia neuromodulation | Advanced PD with motor complications |
Recent Evidence (2024-2026)
Recent meta-analyses have highlighted:
- GBA1 gene variants and their genotype-phenotype relationships as important risk stratifiers (PMID: 39927608, Movement Disorders, 2025)
- Gut microbiome alterations are consistently associated with PD, supporting the gut-brain axis hypothesis (PMID: 40335465, Nature Communications, 2025)
- Investigations into natural compounds and novel targets continue, though no disease-modifying therapy has yet been established
Note: The field of PD is rapidly evolving. For the latest treatment guidelines (e.g., from the MDS or AAN), consulting current guidelines is recommended as evidence continues to accumulate.
Primary sources: Goldman-Cecil Medicine 22E, Lippincott Illustrated Reviews: Pharmacology, Bradley and Daroff's Neurology in Clinical Practice, Katzung's Basic and Clinical Pharmacology 16E, Neuroanatomy through Clinical Cases 3E
This is a shared conversation. Sign in to Orris to start your own chat.