Bilirubin
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
I now have all the content needed for a comprehensive answer. Here is a full, textbook-grounded overview of bilirubin.
Bilirubin
Bilirubin is the orange-yellow tetrapyrrole pigment produced from the breakdown of heme. It is the principal end product of heme catabolism and serves as a useful clinical marker of hepatic, biliary, and hemolytic disease.
1. Chemistry and Structure
Bilirubin (discovered by Virchow in 1849 as "hematoidin") is a linear tetrapyrrolic molecule. Its structure was established by X-ray crystallography. Rather than the flat, linear shape initially proposed in 1942, unconjugated bilirubin adopts a ridge-tile (folded) configuration stabilized by six intramolecular hydrogen bonds between its two carboxylic acid side chains and the nitrogen atoms of the pyrrole rings. This internal hydrogen bonding:
- Masks the polar propionic acid groups
- Makes unconjugated bilirubin water-insoluble (and fat-soluble)
- Enables binding to albumin for plasma transport
When exposed to light (~450 nm), the Z,Z configuration converts to E-containing isomers that cannot form the same internal hydrogen bonds and are therefore more water-soluble - the basis of phototherapy in neonatal jaundice.
2. Production - Catabolism of Heme
- Human adults destroy ~200 billion erythrocytes/day, turning over ~6 g of hemoglobin and producing 250-350 mg of bilirubin per day.
- ~80-85% comes from senescent RBC hemoglobin degradation; the remainder from ineffective erythropoiesis and turnover of other hemoproteins (myoglobin, cytochromes).
- Degradation occurs primarily in reticuloendothelial cells of the liver, spleen, and bone marrow.
Steps:
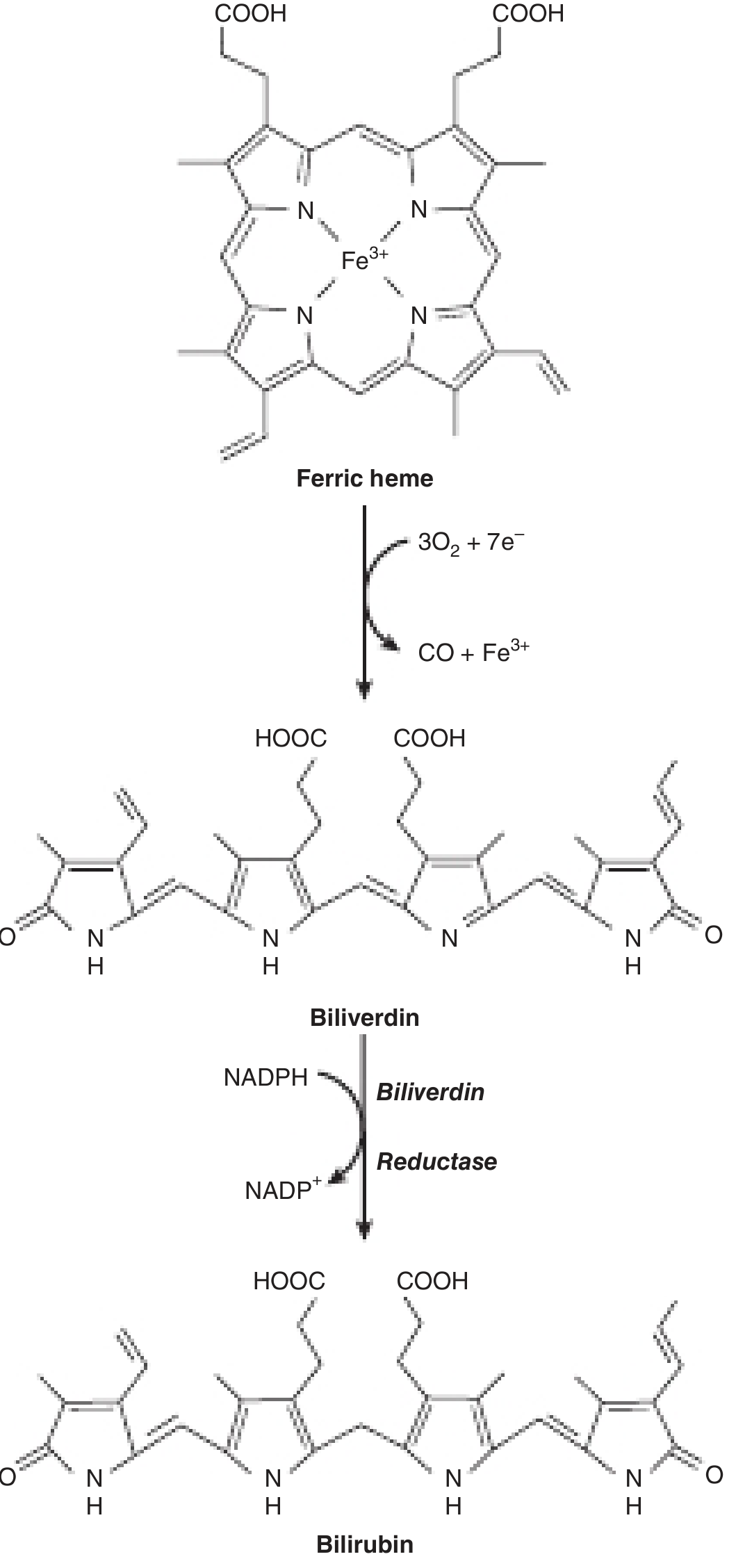
- Heme oxygenase (microsomal, substrate-inducible) cleaves the alpha-methylene bridge of the porphyrin ring:
Fe³⁺-Heme + 3O₂ + 7e⁻ → biliverdin + CO + Fe³⁺
- Consumes 3 mol O₂ and 7 electrons (from NADH/NADPH-cytochrome P450 reductase)
- Releases CO (clinically measurable as a marker of hemolysis) and Fe³⁺ (recycled)
- Birds and amphibians stop here and excrete biliverdin directly
- Biliverdin reductase reduces the central methylene bridge:
Biliverdin + NADPH + H⁺ → bilirubin + NADP⁺
This conversion of heme to bilirubin can be seen visually as a bruise (hematoma) transitions from purple → yellow.
3. Plasma Transport to the Liver
Unconjugated bilirubin is sparingly water-soluble and must be bound to serum albumin for transport:
- Albumin has both high-affinity and low-affinity binding sites
- The high-affinity site can bind ~25 mg bilirubin per 100 mL plasma
- Drugs (e.g., sulfonamides, certain antibiotics) can displace bilirubin from albumin - clinically dangerous in neonates as it allows free bilirubin to cross the blood-brain barrier
4. Hepatic Processing
Transfer from blood to bile involves four steps:
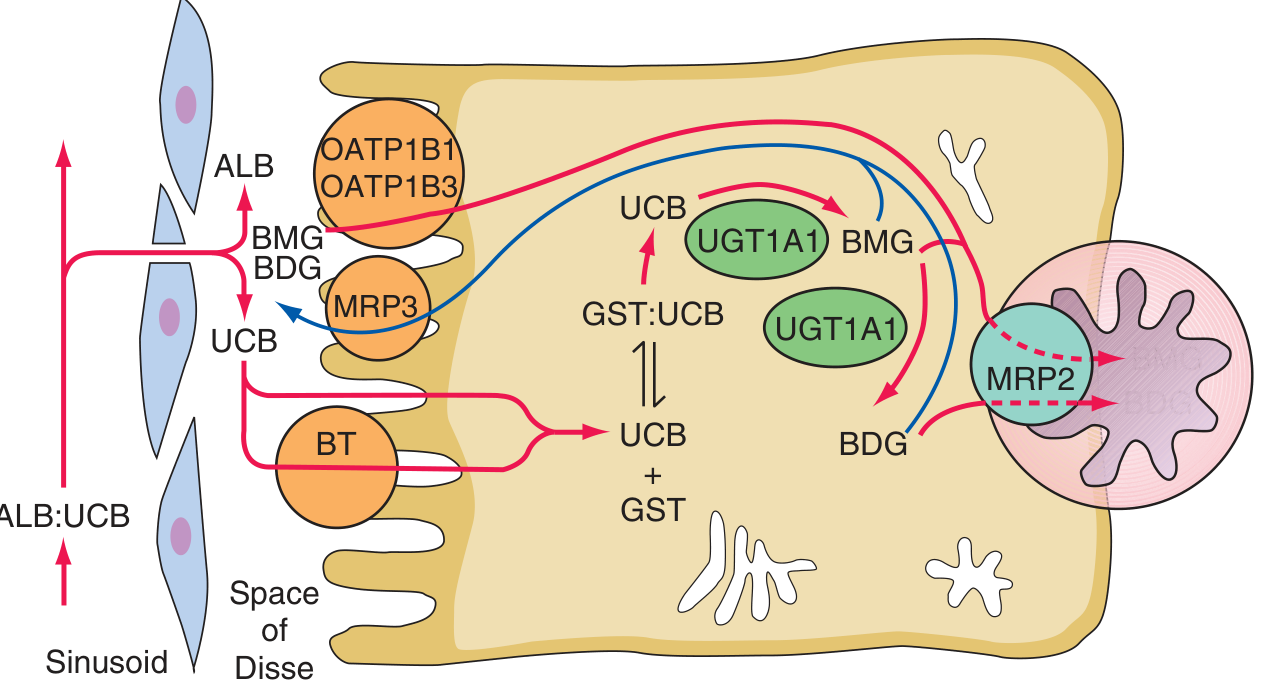
Step 1 - Hepatocellular Uptake
- Bilirubin is dissociated from albumin and taken up at the sinusoidal surface via a large-capacity, saturable facilitated transport system (transporters OATP1B1 and OATP1B3)
- Uptake is NOT the rate-limiting step
Step 2 - Intracellular Binding
- Once inside the hepatocyte, bilirubin binds to cytosolic glutathione-S-transferases (ligandins) which prevent it from refluxing back into the bloodstream and keep it in solution
Step 3 - Conjugation (rate-determining step for clearance)
- UDP-glucuronosyltransferase 1A1 (UGT1A1) in the endoplasmic reticulum catalyzes conjugation with glucuronic acid:
- Bilirubin + UDP-glucuronate → bilirubin monoglucuronide + UDP
- Bilirubin monoglucuronide + UDP-glucuronate → bilirubin diglucuronide + UDP
- Conjugation makes bilirubin water-soluble and excretable
- In normal bile, bilirubin diglucuronide predominates; in obstructive jaundice, monoglucuronide predominates in plasma
- Phenobarbital induces UGT1A1 activity
Step 4 - Canalicular Secretion (rate-limiting step)
- Conjugated bilirubin is actively excreted into bile by MRP2 (multidrug resistance-associated protein 2, a.k.a. MOAT), an ATP-binding cassette transporter on the bile canalicular membrane
- A portion of conjugated bilirubin is also exported back into portal blood by MRP3 and re-taken up by adjacent hepatocytes via OATP1B1/1B3 (hepatic cycling)
5. Gut Metabolism and Enterohepatic Circulation
- Conjugated bilirubin enters the duodenum in bile and passes down the GI tract without mucosal reabsorption
- Gut bacteria reduce conjugated bilirubin to urobilinogen (colorless, water-soluble)
- Urobilinogen undergoes enterohepatic cycling: most is reabsorbed, cleared by the liver, and re-excreted in bile; a small amount reaches systemic circulation and is excreted by the kidneys (urinary urobilinogen)
- Urobilinogen oxidized in the colon becomes stercobilin (gives feces its brown color)
- Conjugated bilirubin cannot be reabsorbed; unconjugated bilirubin that reaches the gut (as in severe unconjugated hyperbilirubinemia, e.g., Crigler-Najjar type I) can be partly reabsorbed, amplifying hyperbilirubinemia
6. Renal Excretion
| Form | Renal Excretion |
|---|---|
| Unconjugated bilirubin | NOT excreted - too tightly albumin-bound for glomerular filtration; no tubular secretion |
| Conjugated bilirubin | Readily filtered at the glomerulus; appears in urine ("bilirubinuria") in hepatic/biliary disease |
Bilirubinuria (dark, tea-colored urine) always indicates conjugated hyperbilirubinemia and implies liver or biliary pathology.
7. Lab Measurement - Direct vs. Indirect Bilirubin
The diazo reaction (Ehrlich 1883, van den Bergh 1916) is the basis of clinical measurement:
- Direct bilirubin: conjugated bilirubin - reacts rapidly with diazo reagent without an accelerator
- Indirect bilirubin: unconjugated - requires ethanol as accelerator; calculated as total minus direct
Four fractions identified by HPLC:
- Alpha (α): unconjugated bilirubin
- Beta (β): bilirubin monoglucuronide
- Gamma (γ): bilirubin diglucuronide
- Delta (δ): bilirubin covalently bound to albumin (appears in prolonged conjugated hyperbilirubinemia; long half-life explains persisting jaundice after biliary obstruction is relieved)
Normal serum total bilirubin: < 1.0-1.2 mg/dL (< ~17-21 μmol/L)
8. Clinical Significance - Jaundice and Hyperbilirubinemia
Jaundice (icterus): yellowish discoloration of skin, sclerae, and mucous membranes due to tissue deposition of bilirubin.
- Scleral icterus is detectable at serum bilirubin ≥ 3 mg/dL (51 μmol/L) - sclerae have high elastin content with strong bilirubin affinity
- Prolonged jaundice can appear greenish (oxidation of bilirubin → biliverdin)
Differential Diagnosis by Bilirubin Fraction
Unconjugated (indirect) hyperbilirubinemia - causes:
| Mechanism | Examples |
|---|---|
| Increased production | Hemolysis, ineffective erythropoiesis, hematoma resorption, thalassemia |
| Decreased uptake | Heart failure, drugs (rifampicin) |
| Decreased conjugation | Gilbert syndrome, Crigler-Najjar I & II, physiologic neonatal jaundice |
Note: Hemolysis alone cannot raise bilirubin above ~4 mg/dL (68 μmol/L) with normal liver function - higher values imply concomitant hepatic dysfunction.
Conjugated (direct) hyperbilirubinemia - causes:
- Hepatocellular disease (hepatitis, cirrhosis)
- Cholestasis (intrahepatic or extrahepatic biliary obstruction)
- Hereditary: Dubin-Johnson syndrome, Rotor syndrome
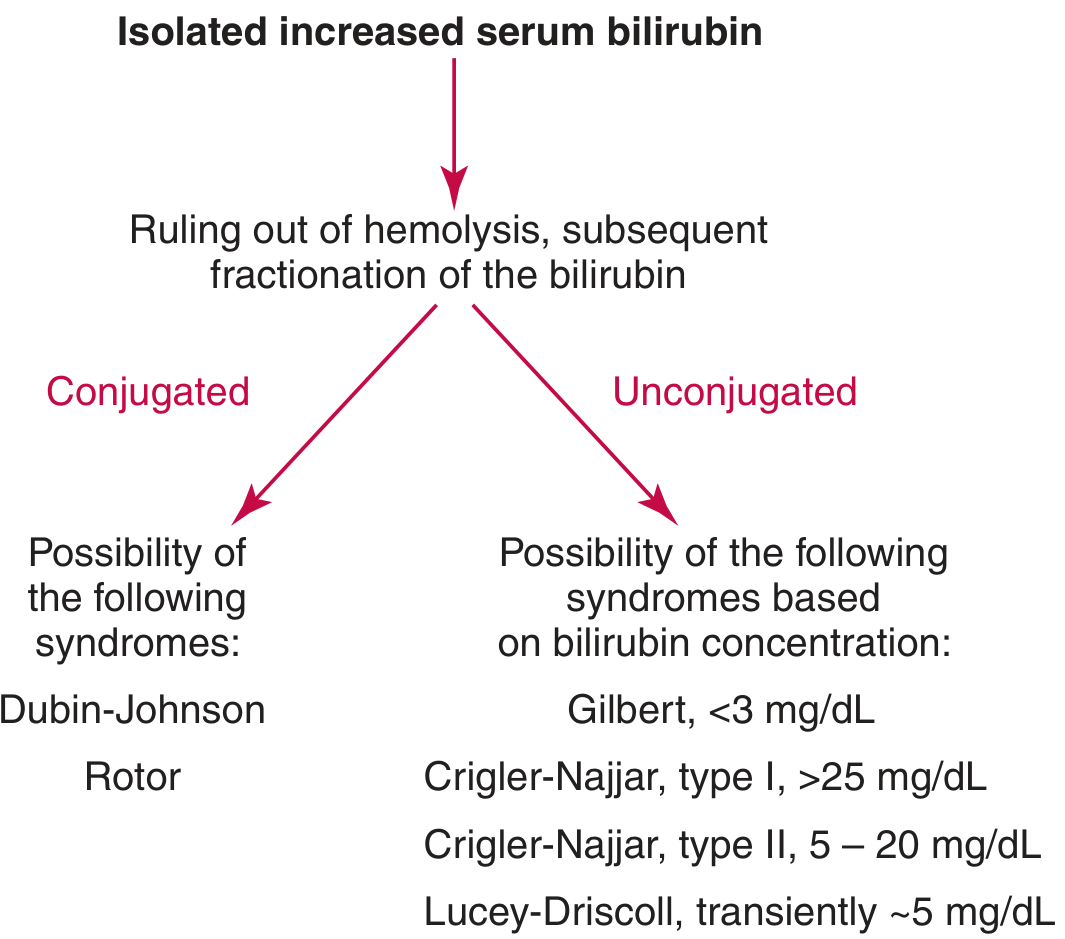
9. Hereditary Disorders of Bilirubin Metabolism
| Disorder | Defect | Bilirubin Type | Bilirubin Level | Key Feature |
|---|---|---|---|---|
| Gilbert syndrome | Mild UGT1A1 reduction (~30% activity) | Unconjugated | < 3 mg/dL | Benign; triggered by fasting/stress; most common (~5-10% population) |
| Crigler-Najjar type I | Complete absence of UGT1A1 | Unconjugated | 20-45 mg/dL (340-765 μmol/L) | Requires 10-12 hrs/day phototherapy; fatal without liver transplant; no response to phenobarbital |
| Crigler-Najjar type II (Arias) | Severely reduced UGT1A1 | Unconjugated | 5-20 mg/dL | Responds to phenobarbital; generally benign |
| Dubin-Johnson syndrome | Defect in MRP2 (canalicular excretion) | Conjugated | Mild | Liver appears black (melanin-like pigment); benign |
| Rotor syndrome | Defect in OATP1B1/1B3 (hepatic uptake of conjugated bilirubin) | Conjugated | Mild | No liver pigment; benign |
10. Neonatal Jaundice and Kernicterus
Neonatal (physiologic) jaundice reflects:
- Increased RBC turnover (fetal Hb replacement)
- Immature UGT1A1 conjugating capacity
- Increased enterohepatic circulation (low gut bacteria; beta-glucuronidase in meconium deconjugates bilirubin)
At serum unconjugated bilirubin > 340 μmol/L (20 mg/dL), bilirubin crosses the immature blood-brain barrier and deposits in the basal ganglia and brainstem → kernicterus (bilirubin encephalopathy), causing neurologic deficits or death.
Treatment:
- Phototherapy (450 nm blue light): converts Z,Z bilirubin to more water-soluble E-isomers, which are excreted directly in bile without requiring conjugation
- Exchange transfusion for severe cases
Sources:
- Harper's Illustrated Biochemistry, 32nd Ed, Chapter 31 (Catabolism of Heme - Produces Bilirubin)
- Harrison's Principles of Internal Medicine, 22nd Ed (2025), Chapter 52 (Jaundice) and Chapter 349 (The Hyperbilirubinemias)
- Tietz Textbook of Laboratory Medicine, 7th Ed, Chapter 51 (Clinical Significance of Bilirubin)
This is a shared conversation. Sign in to Orris to start your own chat.