Status epileptic us mx make a note from llatest guidelines , refer srilankan ones too
Reading File
Finding Sources
Searching PubMed
"status epilepticus" AND management
Searching the Web
Sri Lanka status epilepticus management guidelines 2023 2024
Reading File
Reading File
Reading Article
PMID: 38606469
Reading Article
PMID: 35333156
Reading File
Reading Web Page
https://www.ilae.org/journals/epigraph/epigraph-vol-24-issue…
Loading Image
I now have comprehensive information to compile a thorough clinical note. Let me compile the full note.
Status Epilepticus (SE) - Clinical Management Note
Compiled from: Tintinalli's Emergency Medicine, Rosen's Emergency Medicine, ICS UK 2025 Guidance, Vignatelli et al. Epilepsia 2024, Cruickshank et al. Health Technol Assess 2022, and ILAE Sri Lanka context (Wanigasinghe, 2022)
Definition and Time-Based Framework
Status epilepticus is defined as:
- A single seizure >= 5 minutes in duration, OR
- Two or more seizures without recovery of consciousness between them
Why 5 minutes matters: After 5 minutes, seizures are less likely to terminate spontaneously, less responsive to anti-seizure medications (ASMs), and more likely to cause neuronal injury. After 20 minutes, systemic complications emerge - hypotension, hypoxia, metabolic acidosis, hyperthermia, hypoglycemia, cardiac dysrhythmias, and pulmonary edema.
Operational time phases (ILAE/international guidelines):
| Phase | Time | Definition |
|---|---|---|
| Early SE | 5-30 min | Treat urgently |
| Established SE | 30-60 min | Requires 2nd-line ASM |
| Refractory SE (RSE) | >30-60 min despite 1st + 2nd line | Requires anaesthetic infusion |
| Super-refractory SE (SRSE) | RSE persisting >24h despite anaesthesia | Specialist management |
Common Causes (Etiologies to Screen For)
- Subtherapeutic ASM levels (most common in known epilepsy)
- Acute stroke / CVT
- CNS infection (meningitis, encephalitis - screen and treat empirically early)
- Metabolic derangements (hypoglycemia, hyponatremia, hypocalcemia, hypomagnesemia)
- Alcohol or drug intoxication / withdrawal
- Anoxia / hypoxia
- Autoimmune encephalitis (NMDAR, LGI1, CASPR2, etc.) - consider in NORSE/FIRES
- Trauma, tumour, posterior reversible encephalopathy syndrome (PRES)
- Eclampsia (in pregnant women - treat as emergency; do not withhold treatment)
Non-Convulsive SE (NCSE)
Often underdiagnosed. Suspect when:
- Prolonged postictal period after a generalised seizure
- Subtle motor signs: twitching, blinking, eye deviation
- Fluctuating or unexplained altered mental status / stupor / confusion
Diagnosis requires EEG. Admit EEG if patient remains unconscious without visible seizures.
Initial Stabilisation (0-5 min)
Simultaneous with drug treatment:
- Airway - positioning, suction available; nasopharyngeal airway if needed (avoid oropharyngeal - may induce vomiting); prepare for intubation
- Breathing - O2 by mask; bag-valve-mask if ventilation inadequate
- Circulation - large-bore IV access; IV normal saline (NOT glucose-containing fluids - phenytoin incompatible); cardiac monitor, pulse oximetry, end-tidal CO2
- Glucose - bedside BGL immediately; give IV dextrose if hypoglycaemic (give thiamine 100 mg IV first if alcoholism/malnutrition suspected)
- Temperature - monitor continuously; treat hyperthermia with antipyretics and cooling
- Labs: electrolytes, glucose, Ca, Mg, lactate, LFTs, RFTs, CBC, ABG, toxicology screen, ASM levels (if known epileptic), pregnancy test if applicable
Treatment Protocol (Time-Staged)
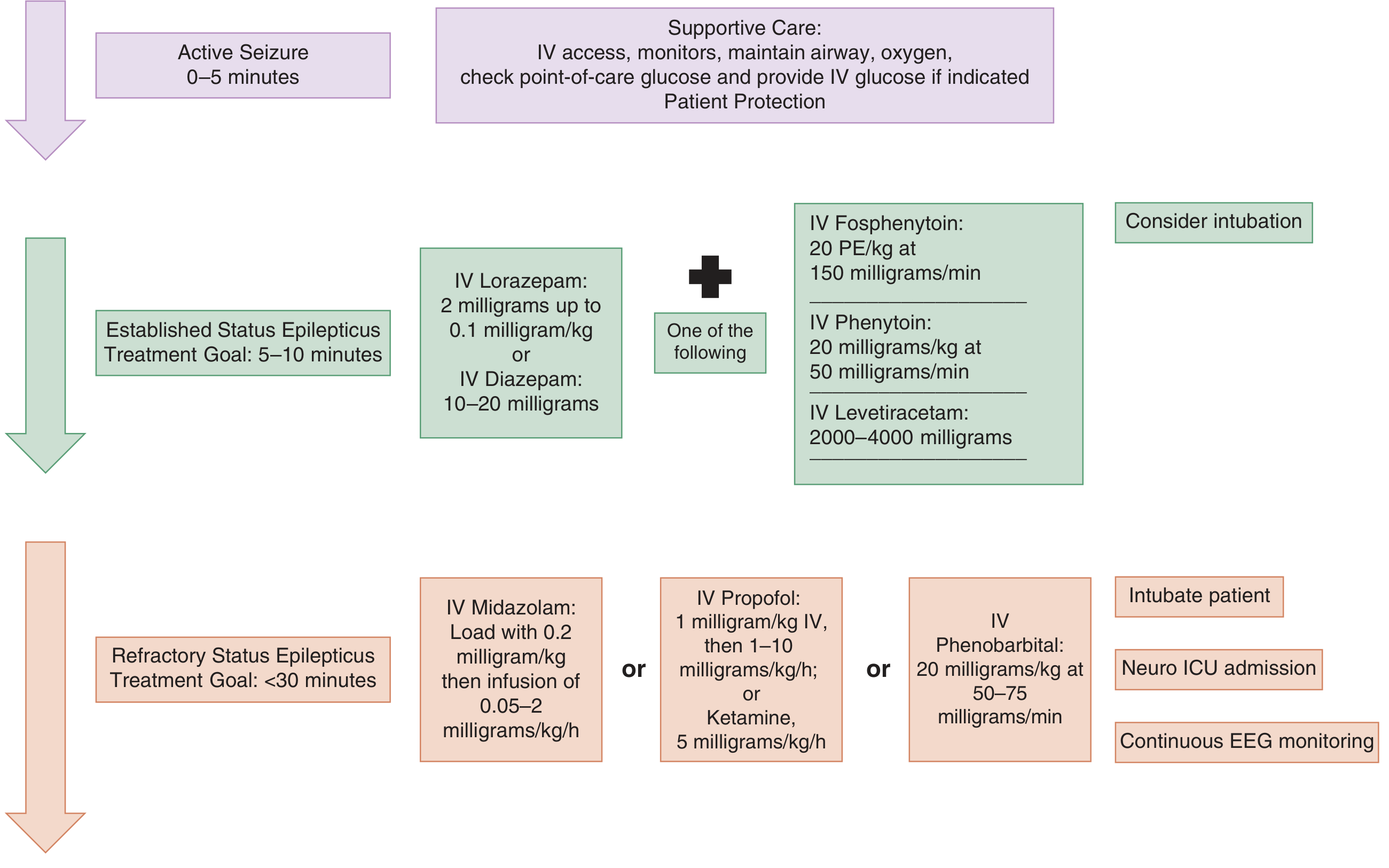
Phase 1 - First-Line: Benzodiazepines (0-10 min)
Benzodiazepines terminate seizures in approximately 70% of cases. Delays beyond 10 minutes are associated with higher mortality, longer seizure duration, and more complications.
| Drug | Route | Dose | Notes |
|---|---|---|---|
| Lorazepam | IV | 0.1 mg/kg (up to 4 mg/dose); repeat once after 5 min | Preferred if IV access established |
| Diazepam | IV | 10-20 mg (0.15-0.25 mg/kg) | Repeat after 5 min if ongoing |
| Midazolam | IM | 10 mg (>40 kg); 5 mg (13-40 kg) | Non-inferior to IV lorazepam - use when no IV access |
| Midazolam | Buccal/IN | 0.2-0.5 mg/kg | Prehospital / community; preferred non-IV route |
| Diazepam | Rectal | 0.5 mg/kg | Less preferred; use only if no other route available |
- Repeat benzodiazepine after 5 minutes if seizure persists
- Give second dose if needed; after two doses, proceed to Phase 2
Watch for: Respiratory depression, hypotension (risk increases with repeated doses)
Phase 2 - Second-Line ASMs (10-30 min)
If seizure persists after two benzodiazepine doses, load with ONE of the following:
| Drug | Dose | Rate | Notes |
|---|---|---|---|
| Levetiracetam (LEV) | 60 mg/kg IV (max 4500 mg) | Over 10 min | No cardiac/hepatic monitoring required; evidence equivalent to phenytoin; fewer adverse events |
| Sodium Valproate (VPA) | 40 mg/kg IV (max 3000 mg) | Over 10 min | Contraindicated: liver disease, thrombocytopenia, possible metabolic disease, pregnancy (teratogenic) |
| Fosphenytoin | 20 PE/kg IV at 150 mg PE/min | - | Preferred over phenytoin; IM-compatible, less cardiotoxic, faster infusion |
| Phenytoin | 20 mg/kg IV at max 50 mg/min | Slow infusion | Cardiac monitoring mandatory; hypotension and arrhythmia risk; not IM-compatible; NOT in glucose solutions |
| Phenobarbital | 20 mg/kg IV at 50-75 mg/min | - | Still effective; available in many settings; sedation risk |
Note on evidence (Vignatelli et al., Epilepsia 2024 [PMID 38606469]): A systematic review of 15 international CPGs found broad consensus on first-line benzodiazepines and third-line anaesthetics, but less agreement on second-line agents. LEV, VPA, and fosphenytoin are all acceptable; no single agent is clearly superior.
ESETT trial evidence: No significant difference in efficacy or safety between LEV, fosphenytoin, and VPA in established SE.
If seizure persists after the first second-line agent, a second second-line agent may be tried before moving to Phase 3.
Phase 3 - Refractory SE: Continuous Anaesthetic Infusion (>30-60 min)
Indications: Seizures persisting despite 2 adequate benzodiazepine doses + 1-2 second-line ASMs.
Requires: intubation + continuous EEG monitoring + ICU admission
| Drug | Loading dose | Infusion | Notes |
|---|---|---|---|
| Midazolam | 0.2 mg/kg IV | 0.05-2 mg/kg/h | First choice; titrate to seizure control |
| Propofol | 1-2 mg/kg IV | 1-10 mg/kg/h | Monitor for PRIS (Propofol Infusion Syndrome) - ECG daily; CK + triglycerides if dose >4 mg/kg/h; avoid prolonged high doses, especially in children |
| Ketamine | 1-2 mg/kg IV | 0.5-7 mg/kg/h | NMDA antagonist; useful in refractory SE; may have neuroprotective properties; growing evidence (Chiriboga et al., Epilepsia 2024 [PMID 38881333] - systematic review in paediatric SE) |
| Thiopentone (Thiopental) | - | Titrate to burst suppression | Deep barbiturate coma; last resort; prolonged sedation |
| Phenobarbital | 20 mg/kg IV | - | Alternative if above unavailable |
EEG target: Burst suppression pattern (or seizure freedom for at least 24-48h before tapering).
Tapering: Taper over ~6h under EEG monitoring. If seizures recur during taper, extend anaesthesia and reassess. Do NOT perform routine daily sedation holds in SE.
Super-Refractory SE (SRSE) - Persisting >24h
Consult neurology/regional neurosciences centre. Consider:
- Alternative anaesthetic agent (switch, e.g., midazolam to propofol or vice versa; add thiopentone for 48h)
- Inhalational anaesthesia (isoflurane via ICU ventilator)
- Additional ASMs: lacosamide IV (200-400 mg loading), phenobarbital, topiramate (via NGT), carbamazepine (NGT)
- Magnesium infusion - aim serum Mg 1.0-1.5 mmol/L (especially in eclampsia)
- Ketogenic diet (via NGT) - strong evidence in SRSE; recommended in 7 of 15 international CPGs
- Immunotherapy (if autoimmune aetiology suspected or confirmed):
- First-line: methylprednisolone 1 g/day x3 days + IVIG + plasma exchange
- Second-line: rituximab, cyclophosphamide
- Consider tocilizumab (anti-IL6), anakinra (IL-1RA), bortezomib (NMDAR encephalitis)
- Vagus nerve stimulation (VNS) - in selected cases
- Surgery - if focal structural lesion identified
- Electroconvulsive therapy (ECT) - occasionally used
ICU / Supportive Care Bundle
Based on ICS UK 2025 guidance (PMC12062632):
- Airway (A): Secure if GCS impaired or ongoing RSE
- Breathing (B): Ventilatory management; avoid hypoxia/hypercapnia
- Circulation (C): Target MAP; correct haemodynamic instability
- Disability (D): No routine daily sedation holds; taper as above; target blood glucose 8-12 mmol/L
- GI (E): Early enteral nutrition within 48h
- Infection (F): Treat meningitis/encephalitis empirically (ceftriaxone + aciclovir) while awaiting CSF; don't delay antibiotics for LP if signs of raised ICP
- Monitoring: Continuous EEG (cEEG) is standard for RSE/SRSE or unexplained unconsciousness; daily ECG when propofol used
Investigations to guide aetiology:
- CT/MRI brain (r/o structural cause, PRES, CVT, HSV encephalitis)
- LP (meningitis, encephalitis, autoimmune) - store CSF for future analysis
- EEG - diagnostic in NCSE and monitoring in RSE/SRSE
- ASM levels, autoimmune antibody panel (serum + CSF), paraneoplastic screen
- CK if rhabdomyolysis suspected (prolonged SE or post-ictal)
Long-Term ASM Management
- Continue all pre-existing ASMs at full dose - reverse any recent reductions
- Start or optimize a maintenance ASM once SE is controlled
- Address the underlying aetiology
- Plan neurology follow-up
Special Populations
Pregnancy / Eclampsia
- Treat SE immediately - no teratogenic risk justifies withholding life-saving treatment
- Magnesium sulphate is first-line for eclamptic SE
- Avoid valproate (teratogenic, especially first trimester)
- Lamotrigine and levetiracetam - lowest malformation risk if maintenance ASM needed
- Monitor and increase ASM doses during pregnancy (clearance increases significantly)
Paediatric SE
- Same staged protocol; weight-based dosing
- Buccal midazolam and rectal diazepam are practical pre-hospital options
- Ketamine increasingly supported by evidence (systematic review 2024)
- Febrile SE: most self-limiting; treat as per protocol if >5 min
Sri Lanka Context (ILAE, 2022 - Prof. Jithangi Wanigasinghe, University of Colombo)
Sri Lanka operates within a national health system with staged referral (primary → secondary → tertiary), but faces resource limitations relevant to SE management:
Available first-line:
- Diazepam IV/rectal - available in all hospitals (primary care and above)
- Midazolam IV - available at some hospitals but inconsistently; buccal/IM formulation NOT routinely available; IV-only
Available second-line:
- Phenytoin - generally available
- Phenobarbital - not always reliably available (supply issues)
What is NOT routinely available in Sri Lanka:
- Fosphenytoin (not widely stocked)
- Levetiracetam IV
- Sodium valproate IV
- Lacosamide IV
- Continuous EEG (cEEG) monitoring
RSE challenges:
- ICU access is very limited - most RSE managed in general wards
- IV midazolam infusions given in non-ICU settings (high-risk)
- High mortality in RSE due to limited escalation options
- Anaesthetic agents available if patient reaches ICU, but access is often delayed
Paramedic system:
- National ambulance service exists but paramedics do not administer medications - retrieval and basic life support only
- No pre-hospital drug treatment
Practical Adapted Protocol for Sri Lanka / Resource-Limited Settings
| Phase | Preferred Drug | Alternative |
|---|---|---|
| First-line | Diazepam IV 10-20 mg (or rectal 0.5 mg/kg if no access) | Midazolam IV 10 mg if available |
| Second-line | Phenytoin IV 20 mg/kg at max 50 mg/min (with cardiac monitoring) | Phenobarbital IV 20 mg/kg if phenytoin unavailable |
| RSE | IV midazolam infusion 0.05-0.2 mg/kg/h (ICU preferred; often in general ward) | Phenobarbital infusion; anaesthetic agents if ICU reached |
| SRSE | Seek tertiary neurology referral urgently | Ketogenic diet (NGT); immunotherapy if autoimmune suspected |
Key advocacy points (ILAE recommendation):
- Every hospital where a patient may present should stock at least first- and second-line medications reliably
- Midazolam buccal formulation should be made available at primary care level
- Phenobarbital supply chain must be maintained
- Clinical staff at all levels need training in early recognition and treatment - delays beyond 10 minutes significantly worsen outcomes
Key References
- Vignatelli L et al. Clinical practice guidelines on the management of status epilepticus in adults: A systematic review. Epilepsia 2024. [PMID 38606469] - 15 CPGs reviewed; broad agreement on benzodiazepines and anaesthetics; less consensus on second-line agents
- Cruickshank M et al. Pre-hospital and emergency department treatment of convulsive status epilepticus in adults: evidence synthesis. Health Technol Assess 2022. [PMID 35333156] - IM midazolam non-inferior to IV lorazepam; both superior to placebo
- Chiriboga N et al. Systematic review and meta-analysis of ketamine in paediatric status epilepticus. Epilepsia 2024. [PMID 38881333]
- ICS UK / Intensive Care Society. Guidance for the Acute Management of Status Epilepticus in Adult Patients. 2025. [PMC12062632] - Endorsed by Royal College of Emergency Medicine and Society for Acute Medicine
- Wanigasinghe J (University of Colombo). Sri Lanka perspective. ILAE Epigraph Vol.24 Issue 2, 2022 - Addressing SE in low-resource regions
- Tintinalli's Emergency Medicine, 9e - Chapter 171
- Rosen's Emergency Medicine, 9e - Chapter 169
Bottom line for clinical practice:
Start treatment at 5 minutes. Do not wait for 30 minutes. Benzodiazepines first - IM midazolam is as good as IV lorazepam and should be given immediately if no IV access. Move to second-line at 10-20 minutes if seizure persists. Move to anaesthetic infusion + intubation + ICU at 30-60 minutes. In Sri Lanka and resource-limited settings, use what is available - diazepam and phenytoin/phenobarbital remain effective; early escalation and ICU referral is the primary bottleneck to address.
This is a shared conversation. Sign in to Orris to start your own chat.