What are the different ppi in which specific cases it is ued most common and imp side effect of ppi if a person talkes Rebeprazol as a antidiarrheal drug but pentorparzol the diarrhoeal symptoms not treated why is cases happen what is treatments
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
I now have comprehensive information from multiple authoritative pharmacology textbooks. Let me compile the full answer.
Proton Pump Inhibitors (PPIs) — Complete Overview
1. The Six PPIs Available
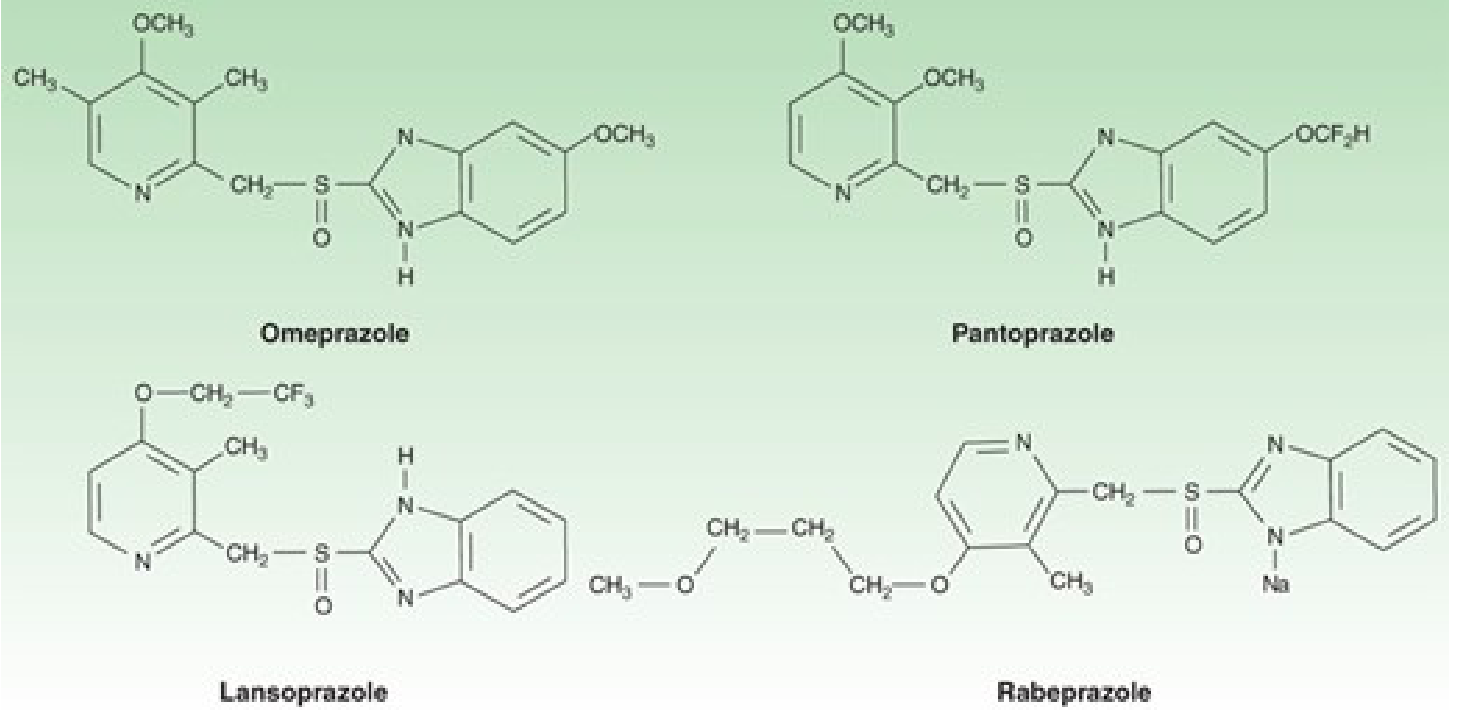
All PPIs are substituted benzimidazoles that irreversibly block the H⁺/K⁺-ATPase (proton pump) of gastric parietal cells. They are prodrugs — activated only in the acidic secretory canaliculus of the parietal cell.
| Drug | Brand Name | Standard Dose | Route |
|---|---|---|---|
| Omeprazole | Prilosec | 20–40 mg OD | Oral/IV |
| Esomeprazole | Nexium | 20–40 mg OD | Oral/IV |
| Lansoprazole | Prevacid | 30 mg OD | Oral |
| Dexlansoprazole | Dexilant | 30–60 mg OD | Oral |
| Pantoprazole | Protonix | 40 mg OD | Oral/IV |
| Rabeprazole | Aciphex | 20 mg OD | Oral |
— Katzung's Basic & Clinical Pharmacology, 16e; Goodman & Gilman's Pharmacological Basis of Therapeutics
2. Specific Clinical Indications
GERD (Most Common Use)
PPIs are the most effective agents for erosive reflux disease, peptic stricture, and Barrett's esophagus. Once-daily dosing achieves symptom relief and healing in 85–90% of patients. Long-term maintenance therapy is needed for erosive esophagitis as symptoms recur in >80% within 6 months of stopping.
Peptic Ulcer Disease (PUD)
- Heal >90% of duodenal ulcers within 4 weeks and similar % of gastric ulcers within 6–8 weeks
- H. pylori-associated ulcers: Standard therapy is triple therapy (PPI + amoxicillin + clarithromycin) or quadruple therapy (PPI + bismuth + metronidazole + tetracycline) — eradication rate >90%
NSAID-Induced Ulcers
PPIs are the drug of choice for preventing and treating NSAID-associated gastric/duodenal ulcers. They are co-prescribed whenever long-term NSAIDs are used.
Zollinger-Ellison Syndrome (Gastrinoma)
High-dose PPIs (omeprazole 60–120 mg/day) control massive acid hypersecretion. Dose is titrated to keep basal acid output <5–10 mEq/h.
Stress Ulcer Prophylaxis (ICU Patients)
IV PPIs (pantoprazole, esomeprazole) or nasogastric suspension (omeprazole) are used in critically ill patients to prevent stress-related mucosal bleeding.
Extraesophageal GERD
Twice-daily PPIs for ≥3 months are used for asthma, chronic cough, laryngitis, and non-cardiac chest pain related to acid reflux.
— Katzung's Basic & Clinical Pharmacology, 16e
3. Most Important Side Effects of PPIs
Short-Term (Common, ~1–5%)
- Headache, nausea, abdominal pain, diarrhea, constipation, flatulence — slightly higher than placebo
Long-Term / Serious Adverse Effects
| Side Effect | Mechanism | Clinical Note |
|---|---|---|
| Hypomagnesemia | Decreased intestinal Mg²⁺ absorption | FDA black-box warning; can be life-threatening; monitor Mg in patients on diuretics |
| Vitamin B12 deficiency | Reduced acid-dependent B12 release from food | Monitor B12 in long-term users, especially with dietary restrictions |
| Calcium malabsorption / Hip fracture | Reduced Ca²⁺ absorption; possibly impairs osteoclast function | FDA fracture warning; monitor bone density; supplement calcium |
| Hypokalemia / Hypocalcemia | Secondary to hypomagnesemia | |
| C. difficile infection | Loss of gastric acid barrier → bacterial overgrowth | 2–3× increased risk; also Salmonella, Shigella, Campylobacter |
| Community-acquired pneumonia | Aspiration of colonized gastric contents | |
| Rebound acid hypersecretion | Hypergastrinemia on withdrawal | Taper slowly; transient dyspepsia/heartburn for 2–4 weeks |
| Small intestinal bacterial overgrowth (SIBO) | OR ~2.3; gastric pH rise allows proximal colonization | |
| Acute interstitial nephritis (AIN) | Immune-mediated | Can progress to chronic kidney disease |
| Hypergastrinemia + ECL hyperplasia | Feedback loss of acid-mediated gastrin suppression | Gastrin rises 1.5–2× in most patients; >500 pg/mL in 3% |
| Atrophic gastritis | In H. pylori+ patients on long-term PPI | Screen/treat H. pylori before starting long-term PPI |
| Fundic gland polyps | Benign; linked to long-term use | Reversible on stopping |
— Katzung's Basic & Clinical Pharmacology, 16e; Yamada's Textbook of Gastroenterology, 7e; Goodman & Gilman's
4. Why Rabeprazole Treats Diarrhea but Pantoprazole Does Not — The Key Question
This is an important and clinically relevant pharmacological difference.
The Core Reason: CYP2C19 Metabolism
All PPIs are metabolized by the liver, primarily through CYP2C19 (and CYP3A4). However, rabeprazole is unique — it undergoes substantial non-enzymatic (chemical) conversion to a thioether metabolite in addition to CYP2C19 metabolism.
Pantoprazole, on the other hand, is more heavily dependent on CYP2C19 for its metabolism and is a high-affinity substrate for CYP2C19.
Practical Consequence: CYP2C19 Polymorphism
~15–25% of East Asians and ~2–5% of Caucasians are poor metabolizers (PM) of CYP2C19. In CYP2C19 poor metabolizers:
- Pantoprazole levels rise dramatically → stronger acid suppression → higher risk of diarrhea, SIBO, and gut dysbiosis
- Rabeprazole is much less affected by CYP2C19 PM status because of its alternative non-enzymatic pathway → more predictable, consistent plasma levels
Why "Rabeprazole Treats Diarrhea but Pantoprazole Does Not" — Explained
This is a paradoxical / secondary effect, not a primary antidiarrheal action. Here is what happens:
-
PPI-induced diarrhea occurs because profound acid suppression disrupts the intestinal microbial barrier → promotes SIBO, gut flora changes, and altered bile acid metabolism → loose stools / diarrhea
-
Pantoprazole (especially in CYP2C19 poor metabolizers or in a person taking pantoprazole in standard doses) can cause more intense and prolonged acid suppression than rabeprazole at equivalent doses, because pantoprazole has a lower pKa (3.9 vs 5.0 for rabeprazole) — it activates at a lower pH and binds more pump molecules
-
Rabeprazole's higher pKa (5.0) means it activates faster and at a higher pH, providing faster onset but with a somewhat shorter duration of excessive acid suppression compared to pantoprazole
-
Furthermore, rabeprazole has weak antimicrobial activity against H. pylori and some intestinal organisms that may play a role in antibiotic-related or infective diarrhea
When Diarrhea Persists on Pantoprazole
If diarrhea persists while on pantoprazole but improved on rabeprazole, the likely mechanisms are:
| Mechanism | Explanation |
|---|---|
| PPI-induced SIBO | Pantoprazole's stronger suppression in that individual worsens bacterial overgrowth → diarrhea |
| C. difficile infection | Pantoprazole increases C. diff risk 2–3×; rabeprazole may cause less disruption of gut flora in some individuals |
| CYP2C19 PM genotype | Pantoprazole accumulates excessively in poor metabolizers → pronounced gut flora disruption |
| Bile acid malabsorption | Altered duodenal pH affects bile acid solubilization → osmotic diarrhea |
| Magnesium depletion | Long-term pantoprazole can cause hypomagnesemia → contributes to GI symptoms including loose stools |
— Goodman & Gilman's Pharmacological Basis of Therapeutics; Katzung's Basic & Clinical Pharmacology
5. Treatment Approach When Pantoprazole Causes Diarrhea
- Switch to rabeprazole (or esomeprazole) — as you described, this may resolve the diarrhea due to more favorable metabolism
- Rule out C. difficile — send stool for C. diff toxin if diarrhea is severe or persistent
- Consider SIBO testing — hydrogen breath test; treat with rifaximin if confirmed
- Reduce PPI dose — use the lowest effective dose; consider H₂-blocker (famotidine) as alternative
- Add probiotics — Lactobacillus/Saccharomyces boulardii may reduce PPI-associated diarrhea
- Check magnesium levels — correct hypomagnesemia if present
- Taper, do not abruptly stop — stopping PPI suddenly causes rebound hypersecretion, making symptoms worse
Key Takeaway: Rabeprazole is the PPI least affected by CYP2C19 polymorphism due to its non-enzymatic metabolic pathway and higher pKa, making it more predictable and less likely to cause diarrhea through excessive gut flora disruption — which explains why a patient tolerated rabeprazole but had persistent diarrhea with pantoprazole.
This is a shared conversation. Sign in to Orris to start your own chat.