Anatomy of lateral geniculate body and visual cortex
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive material from multiple textbooks. Let me compose the full answer.
Anatomy of the Lateral Geniculate Body (LGN) and Visual Cortex
1. The Lateral Geniculate Body (Nucleus)
Location and Gross Anatomy
The lateral geniculate body (lateral geniculate nucleus, LGN) is a thalamic nucleus located at the dorsal end of the thalamus, in the posterior part of the ventral aspect of the thalami. It lies in the roof of the perimesencephalic cistern (cisterna ambiens), just medial to the hippocampal gyrus of the temporal lobe.
On midsection, the LGN is shaped like Napoleon's hat, with its concave aspect (hilus) facing inferoposteromedially, and has a characteristic deep brown color with visible white matter stripes (striae). The geniculate neurons are as numerous as the fibers in the optic tract.
The LGN receives the optic tract anteriorly and gives rise to the optic radiation, which lies in close association with the posterior limb of the internal capsule. Surrounding structures include:
- Superomedially: pulvinar of the thalamus
- Dorsomedially: auditory radiations from the medial geniculate body (on their way to Heschl's gyrus)
- Dorsolaterally: covered by the optic radiations
The shape explains the name: geniculate from the Latin geniculatus meaning "like a little knee." In three dimensions, the six layers are arranged like stacked pancakes bent around the optic tract like a knee joint.
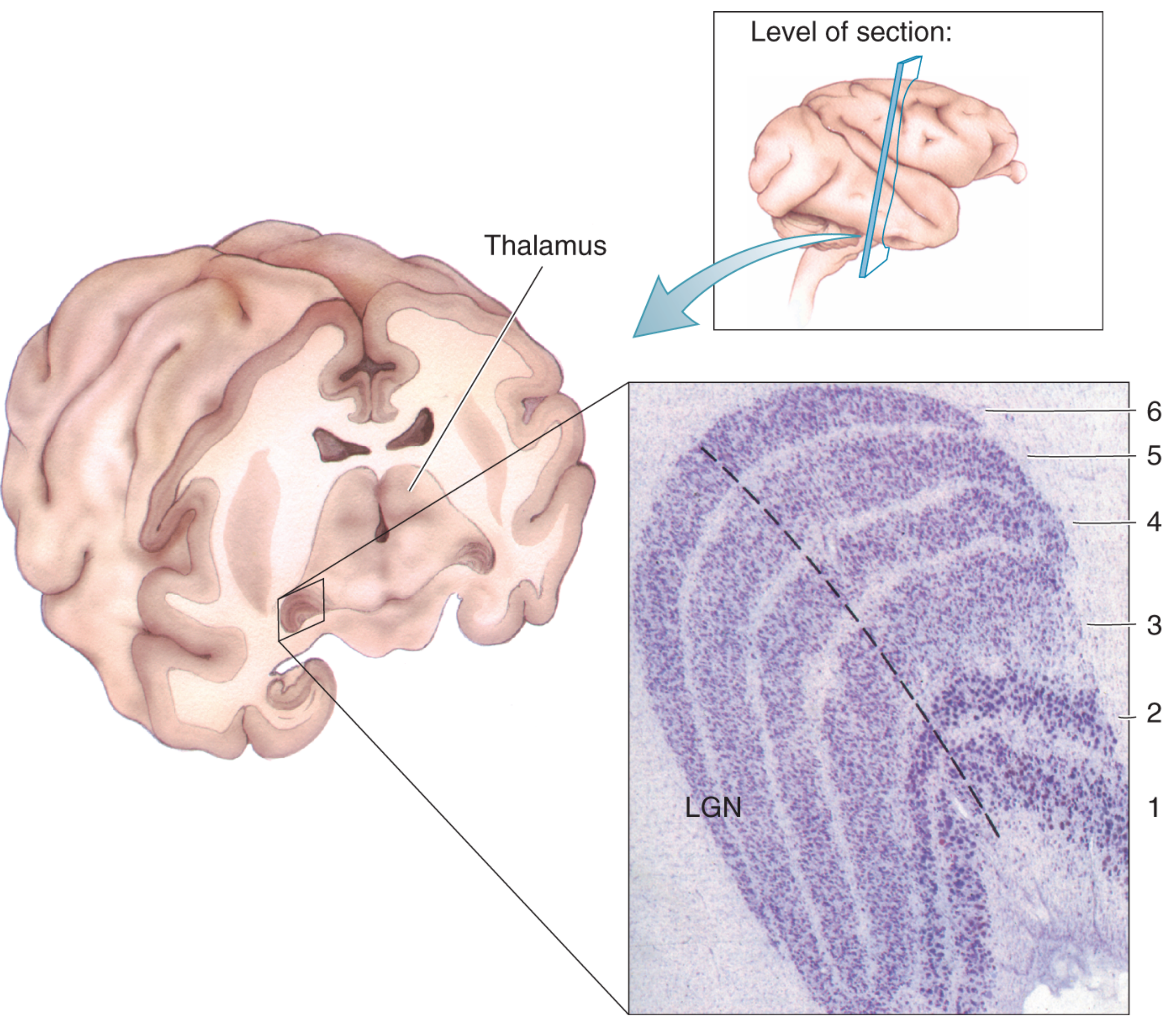
Six-Layer Organization
The LGN is divided into six laminae (layers I-VI), numbered from the hilus:
| Layer | Cell Type | Eye Input |
|---|---|---|
| I | Magnocellular (large) | Contralateral (nasal half of opposite retina) |
| II | Magnocellular (large) | Ipsilateral (temporal half of same retina) |
| III | Parvocellular (small-medium) | Ipsilateral |
| IV | Parvocellular (small-medium) | Contralateral |
| V | Parvocellular (small-medium) | Ipsilateral |
| VI | Parvocellular (small-medium) | Contralateral |
Mnemonic: Layers 1, 4, 6 = contralateral eye; Layers 2, 3, 5 = ipsilateral eye.
The six laminae are clearly distinguished at the center of the LGN (macular representation), but only 1-2 layers are present in the peripheral part receiving input from the peripheral retina.
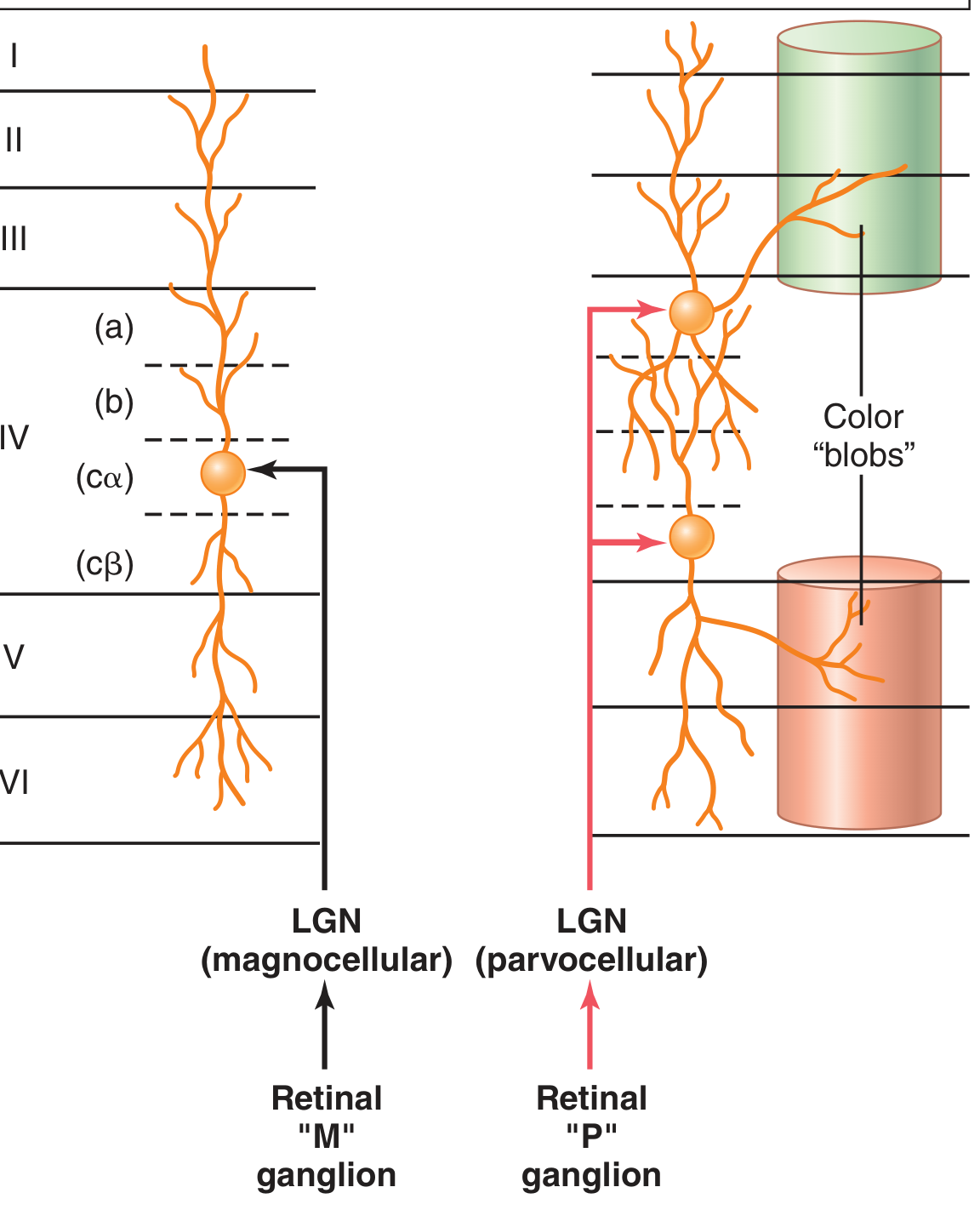
Three Cell Populations
1. Magnocellular layers (layers 1 and 2)
- Large neurons receiving input from M-type retinal ganglion cells
- Rapidly conducting pathway
- Color blind - transmit only black-and-white information
- Poor spatial resolution (few M ganglion cells, wide dendritic spread)
- Project primarily to layer 4Cα of V1
2. Parvocellular layers (layers 3-6)
- Small to medium neurons receiving input from P-type retinal ganglion cells
- Moderate conduction velocity
- Transmit color and accurate point-to-point spatial information
- Project primarily to layer 4Cβ of V1
3. Koniocellular layers (thin layers between principal layers)
- Small "dust-like" neurons
- Located between the principal layers
- Receive input from nonM-nonP (bistratified) ganglion cells
- Project primarily to layers 2 and 3 of V1 (the cytochrome oxidase "blobs")
Functions of the LGN
-
Relay function: Precise point-to-point transmission of visual information from optic tract to visual cortex via the optic radiation, maintaining high spatial fidelity throughout.
-
Gating function: Controls how much signal is allowed to pass to the cortex. Gating control arrives from:
- Corticofugal fibers returning from primary visual cortex back to the LGN
- Reticular areas of the mesencephalon Both sources are inhibitory and can selectively suppress transmission, helping highlight relevant visual information.
Optic Radiation (Geniculocalcarine Tract)
Three bundles arise from the LGN:
- (a) Upper bundle - from medial LGN, corresponding to superior retina; courses through deep parietal white matter and ends in the superior lip of the calcarine fissure
- (b) Central bundle - from medial LGN, serving the macular region; travels through posterotemporal and occipital white matter and ends in the posterior calcarine fissure on both lips
- (c) Lower bundle (Meyer's loop) - from the lateral LGN, corresponding to inferior retina; sweeps anteriorly into the temporal lobe before turning posteriorly to end in the inferior lip of the calcarine fissure
The fibers sweep around the lateral aspect of the posterior lateral ventricles, forming the external sagittal stratum.
2. Primary Visual Cortex (V1)
Location
Primary visual cortex is:
- Brodmann's area 17 in the occipital lobe
- Also called V1, striate cortex, or Visual Area I
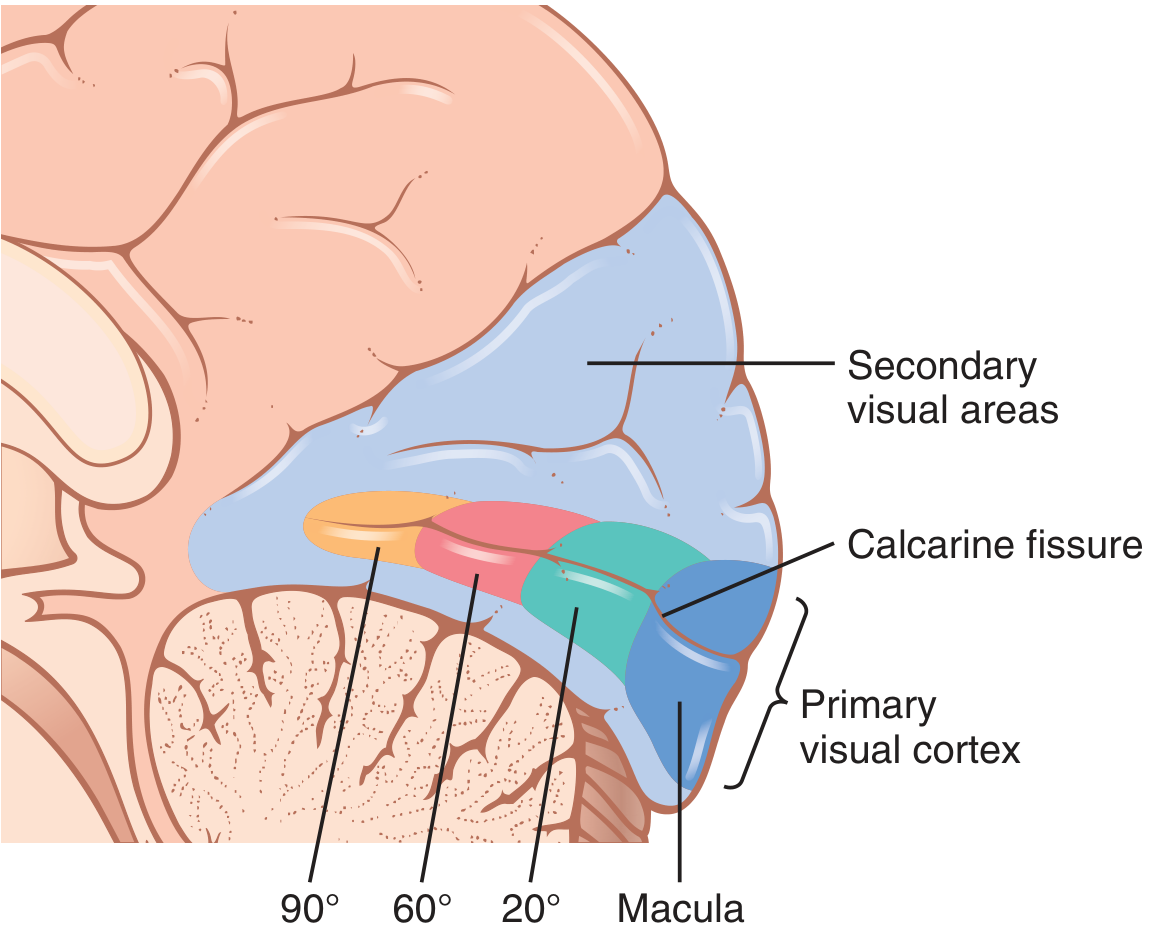
- Located along the superior and inferior lips of the calcarine fissure on the medial aspect of the occipital lobe
- Extends approximately 1 cm around the posterolateral aspect of the occipital pole onto the lateral convexity
Why "Striate Cortex"?
On cross section, a white matter band called the stria of Gennari (line of Gennari) is visible to the naked eye. This corresponds to a thick band of myelinated axons and granular cells in layer IV (devoid of pyramidal cells), reflecting the density of thalamocortical inputs.
Retinotopic Organization
The entire visual cortex is retinotopically organized - neighboring retinal cells project to neighboring cortical locations, creating a map of visual space. Key features:
- Macular (foveal) representation: Located at the posterior pole of the calcarine cortex (occipital pole). The fovea has several hundred times more cortical representation per retinal area than peripheral retina.
- Magnification factor: Central 10-15 degrees of vision occupies 50-60% of total V1 surface area
- Superior retina → superior lip of calcarine fissure
- Inferior retina → inferior lip of calcarine fissure
- Peripheral retina → anterior calcarine fissure (near junction with parietooccipital fissure)
- Each occipital lobe receives projections from the nasal half of the opposite eye and temporal half of the ipsilateral retina (i.e., both eyes representing the same contralateral hemifield)
Six-Layer Structure of V1
Like all neocortex, V1 has six layers, but with specializations:
| Layer | Characteristics | Input/Output |
|---|---|---|
| I | Molecular layer; few cells | Sparse input |
| II | External granular | Outputs to other cortical areas |
| III | External pyramidal | Long-range cortico-cortical outputs (to V2, MT, IT); horizontal connections |
| IVa | Internal granular | Receives parvocellular LGN input |
| IVb | "Line of Gennari" (stria) | Connections |
| IVCα | Dense granular | Receives magnocellular LGN input |
| IVCβ | Dense granular | Receives parvocellular LGN input |
| V | Internal pyramidal | Outputs to superior colliculus, pulvinar |
| VI | Multiform | Feedback to LGN |
The two streams remain segregated in layer 4C: magnocellular → 4Cα, parvocellular → 4Cβ. Koniocellular LGN axons synapse in layers 2 and 3 (at the cytochrome oxidase blobs).
Inputs and Outputs of V1
- Main input: LGN via optic radiation → primarily layer 4C
- Intracortical connections: Radial (perpendicular) connections from layer 4 maintain retinotopy across layers; horizontal connections within layer 3 span different retinotopic locations
- Outputs from V1:
- Layers 2/3 → higher visual areas (V2, V4, MT) via cortico-cortical connections
- Layer 5 → superior colliculus, pulvinar, pons
- Layer 6 → feedback to LGN (corticofugal)
Ocular Dominance Columns
Within layer 4C, input from the right eye and left eye remain in separate ocular dominance columns, arranged as alternating zebra-stripe-like bands running perpendicular to the cortical surface. This segregation established in the LGN is maintained through to V1. Each ~1 mm-wide column responds predominantly to stimulation of one eye.
Cytochrome Oxidase Blobs
Scattered through layers 2 and 3 are regularly spaced peg-like regions of high cytochrome oxidase activity called blobs. These receive input from koniocellular LGN neurons and contain neurons specialized for processing color information.
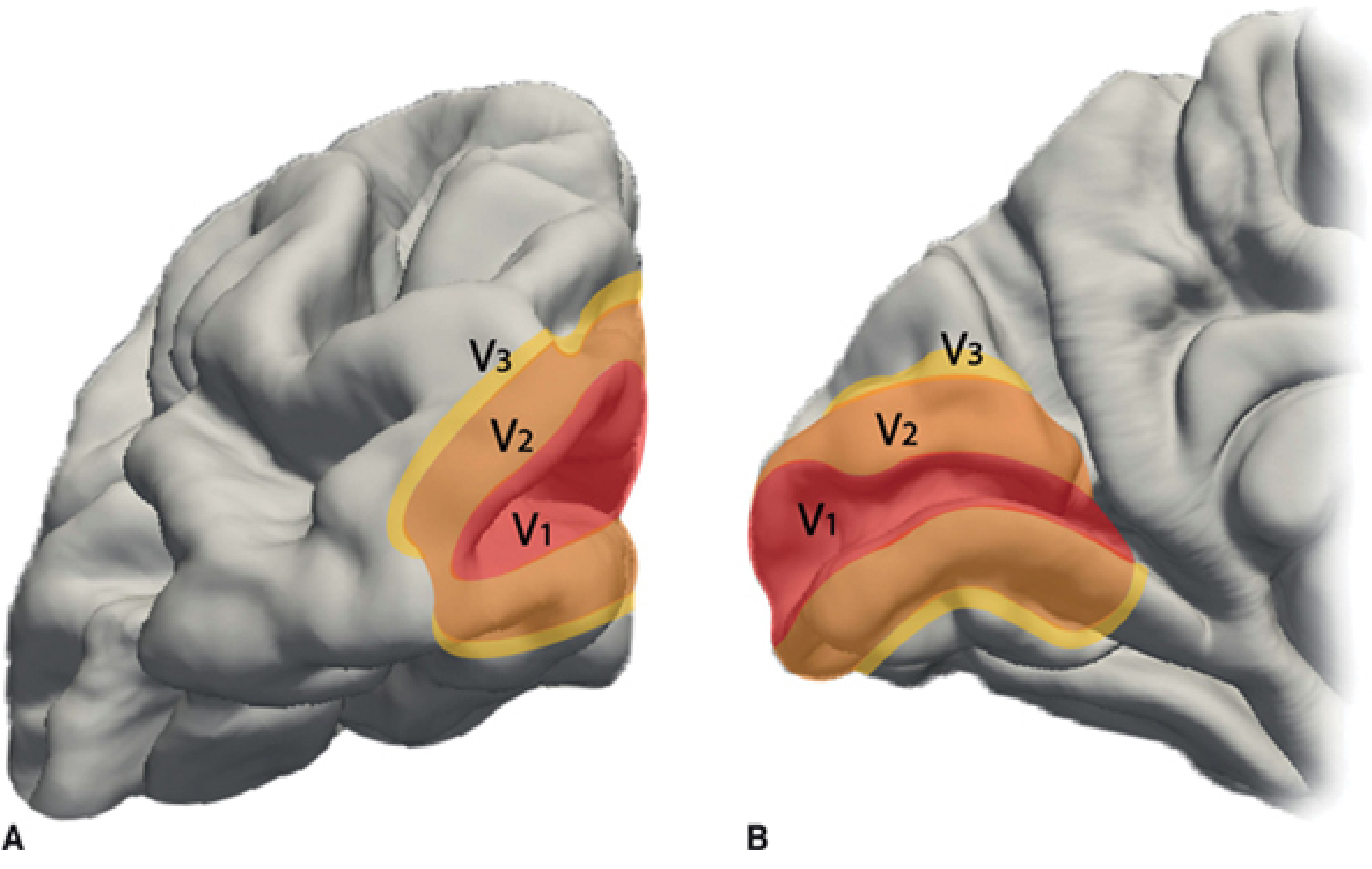
3. Beyond Primary Visual Cortex
Secondary visual areas surround V1 and process specific attributes of the visual scene:
| Area | Location | Function |
|---|---|---|
| V2 (Brodmann area 18) | Immediately surrounds V1 | First relay from V1; surrounds V1 like a border |
| V3 | Adjacent to V2 | Dynamic form |
| V4 | Ventral temporal lobe | Color processing |
| V5/MT | Posterior parietal/temporal junction | Motion detection |
| IT (Inferior Temporal) | Inferotemporal cortex | Object recognition, faces |
These areas form two major processing streams:
- Ventral stream ("what pathway"): V1 → V2 → V4 → IT - object identity, color, detail
- Dorsal stream ("where pathway"): V1 → V2 → V3 → MT → posterior parietal - spatial location, motion
Clinical Correlations
| Lesion Location | Visual Field Defect |
|---|---|
| Optic nerve | Monocular blindness (ipsilateral) |
| Optic chiasm (midline) | Bitemporal hemianopia |
| Optic tract | Contralateral homonymous hemianopia |
| LGN | Contralateral homonymous hemianopia |
| Meyer's loop (temporal lobe) | Contralateral superior quadrantanopia ("pie in the sky") |
| Parietal optic radiation | Contralateral inferior quadrantanopia |
| Calcarine cortex (V1) | Contralateral homonymous hemianopia (macular sparing often present due to dual blood supply) |
| V4 damage | Achromatopsia (loss of color perception) |
| V5/MT damage | Akinetopsia (inability to perceive motion) |
Sources: Neuroscience: Exploring the Brain, 5th Ed. | Localization in Clinical Neurology, 8e | Guyton & Hall Textbook of Medical Physiology | Costanzo Physiology, 7th Ed.
Keratometry
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Finding Sources
Finding Sources
Finding Sources
Reading File
Loading Image
Reading File
Loading Image
I now have all the material needed for a complete answer. Here it is:
Keratometry
Definition and Principle
Keratometry is the measurement of the radius of curvature of the anterior corneal surface, which is then converted into dioptric corneal power. It determines the curvature in the two principal meridians of the cornea - the steepest and the flattest - and expresses results either in:
- Millimetres of radius of curvature (mm), or
- Dioptres (D) of refractive power
The relationship between radius (r) and corneal power (K) is derived from the lensmaker's formula using an assumed keratometric refractive index (n = 1.3375 conventionally, representing a composite of the anterior corneal surface and the posterior corneal curvature in a simplified model):
K (D) = (n - 1) / r = 0.3375 / r(m)
A normal cornea has K readings of approximately 43-45 D (radius ~7.5-7.8 mm) and regular astigmatism means the two principal meridians are perpendicular to each other.
Instruments
1. Manual Keratometer (e.g., Javal-Schiotz, Bausch & Lomb)
The manual keratometer uses the cornea as a convex mirror. It projects a known-size object (the mire) onto the cornea and measures the size of the reflected image. Because image size depends on the radius of curvature, the corneal curvature can be calculated.
- The Javal-Schiotz keratometer is a two-position instrument using two separate mires and rotating the instrument to measure each principal meridian.
- The Bausch & Lomb keratometer uses a single position with doubling prisms to measure both meridians simultaneously.
- Only a small central zone (~3-4 mm) of the cornea is sampled - the so-called "keratometric zone."
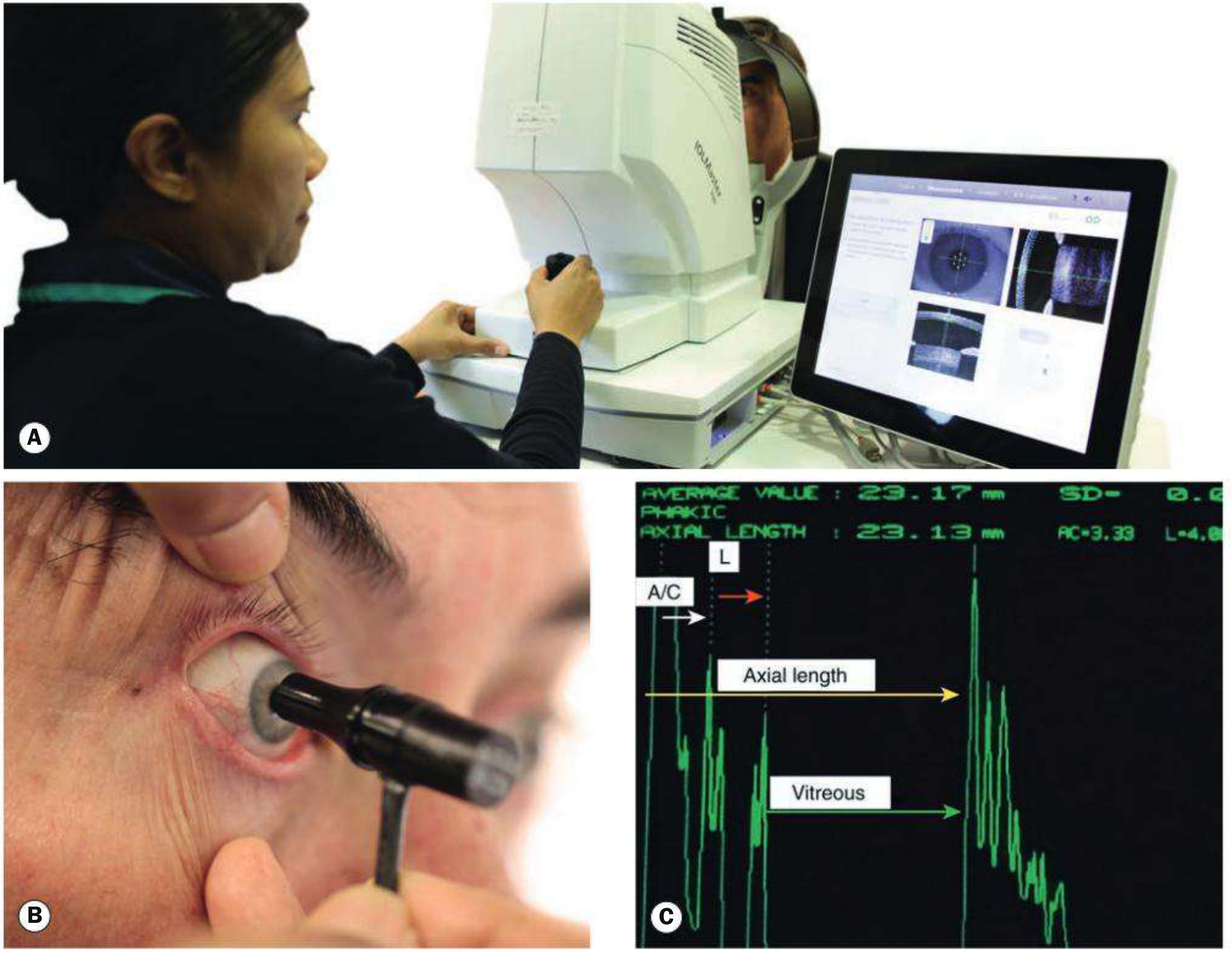
2. Automated Keratometers / Biometers
Modern devices (e.g., IOLMaster, Lenstar) combine partial coherence interferometry (optical coherence biometry) with automated keratometry. They:
- Use two coaxial partially coherent low-energy laser beams to produce an interference pattern
- Simultaneously measure axial length, anterior chamber depth, corneal white-to-white distance, and keratometry
- Provide high reproducibility with less operator skill required
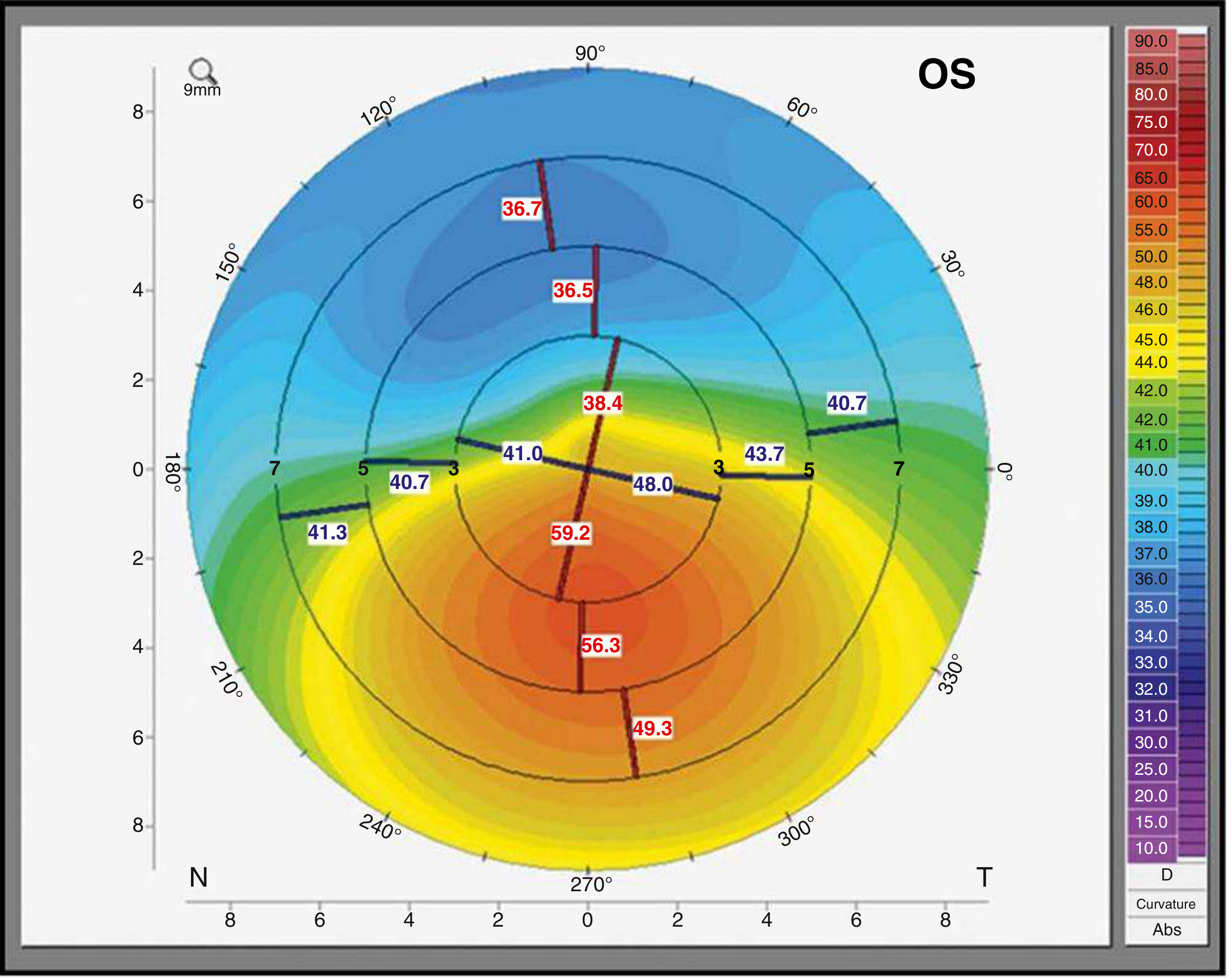
3. Corneal Topography (Videokeratography)
Computerized corneal topography extends keratometry to measure the entire corneal surface rather than just the central 3 mm zone. Techniques include:
- Placido disc analysis: Projects concentric rings onto the anterior corneal surface and analyzes the reflected image. Provides information on anterior corneal power and regularity. Simulated K readings (SimK) can be generated.
- Rasterstereography: Projects a grid pattern rather than rings.
- Results are displayed as color-coded maps (warm colors = steeper/higher power; cool colors = flatter/lower power).
4. Corneal Tomography
Corneal tomography goes further than topography by providing 3D reconstruction of the cornea:
- Rotating Scheimpflug photography (e.g., Pentacam): Images both anterior and posterior corneal surfaces plus corneal thickness throughout. Particularly useful for posterior corneal elevation mapping.
- Scanning slit (e.g., Orbscan): Similarly images the entire corneal profile.
- Anterior segment OCT: High-resolution cross-sectional imaging of cornea and anterior segment.
What Keratometry Measures
| Parameter | What it tells you |
|---|---|
| K1 (flat K) | Flattest corneal meridian (lower dioptre value) and its axis |
| K2 (steep K) | Steepest corneal meridian (higher dioptre value), 90° to K1 in regular astigmatism |
| Average K | Mean of K1 and K2; used in IOL power formulae |
| Corneal astigmatism | Difference between K1 and K2 |
| Axis of astigmatism | Direction of the principal meridians |
Normal average K ≈ 43-44 D. Steep readings (>47-48 D) suggest keratoconus; flat readings (<41 D) may suggest post-refractive surgery changes.
Clinical Applications
1. IOL Power Calculation (Biometry)
Keratometry is one of the two essential parameters for intraocular lens (IOL) power calculation (the other being axial length):
IOL Power = f(K readings, axial length, desired refraction, lens constants)
Commonly used formulae include:
- SRK-T, Holladay 1 & 2, Hoffer Q, Haigis - each incorporating K and axial length
- For short eyes (AL < 22 mm): Hoffer Q, Haigis, Hill-RBF, and Kane formulae are preferred
- For long eyes (AL > 26 mm): BU II, Holladay, Haigis (optimized), and Kane formulae perform better
- Postoperative refraction is within 1.0 D of predicted outcome in ~90% of patients and within 0.5 D in two-thirds
Confounders of keratometry accuracy for IOL calculation:
- Contact lens-induced corneal distortion (remove soft CLs ≥ 1 week; rigid gas-permeable CLs ≥ 6 weeks before biometry)
- Previous corneal refractive surgery (LASIK/PRK alter the anterior corneal curvature, invalidating standard formulae - special adjustment methods such as the refractive history method or Haigis-L formula must be used)
- Irregular corneal surface
- Poor patient fixation
2. Refractive Surgery Screening and Planning
Before LASIK or any corneal refractive surgery:
- Keratometry and topography are performed to exclude keratoconus and forme fruste keratoconus
- Contact lens-induced distortion must be allowed to resolve: soft CLs discontinued for ≥2 weeks, rigid gas-permeable CLs for ≥3 weeks (some surgeons recommend 1 week per year of wear)
- Post-ablation keratometry helps assess the achieved correction
3. Keratoconus Diagnosis and Monitoring
- Keratometry readings in keratoconus are characteristically steep (>47 D or higher)
- The keratometer mires appear irregular and distorted rather than the usual clean circular reflections
- Corneal topography is far more sensitive than keratometry alone, showing:
- Inferior steepening
- Asymmetric bow-tie pattern evolving to displaced steep cone
- Progressive increase in K values over serial measurements
4. Contact Lens Fitting
Keratometry K readings guide the base curve selection for rigid contact lenses. The back optic zone radius of the lens is typically fitted slightly flatter than the flat K reading.
5. Astigmatism Management
Keratometry quantifies corneal astigmatism - the difference between the two principal meridian curvatures. This guides:
- Toric IOL selection (to neutralize corneal astigmatism at cataract surgery)
- Limbal relaxing incisions
- Toric contact lens prescription
6. Cataract Surgery - Unexplained Refractive Surprise
When unexpected post-cataract refractive error occurs, keratometry should be repeated to check for:
- Undiagnosed keratoconus (steep K readings)
- Undiagnosed previous laser refractive surgery (abnormally flat K values)
- Corneal thickness should also be measured
Limitations of Keratometry
| Limitation | Explanation |
|---|---|
| Small sampling zone | Standard keratometry measures only the central ~3-4 mm, missing peripheral and paracentral irregularities |
| Assumes spherical surface | Does not detect irregular astigmatism or corneal ectasia accurately |
| Assumes posterior corneal curvature | Uses a fixed keratometric index - does not directly measure the posterior corneal surface (which contributes ~20% of total corneal power) |
| Post-refractive surgery inaccuracy | Ablation changes the corneal shape in a way that invalidates the standard keratometric index assumption |
| Contact lens warpage | Can mimic keratoconus on topography until lenses are discontinued |
Summary Table
| Feature | Standard Keratometry | Corneal Topography | Corneal Tomography |
|---|---|---|---|
| Instrument | Javal-Schiotz / autokeratometer | Placido disc systems | Scheimpflug / OCT |
| Coverage | Central ~3 mm | Entire anterior surface | Anterior + posterior surfaces |
| Output | K1, K2, axis | Color maps, SimK, Ks | Full pachymetry map, elevation maps |
| Best use | IOL biometry, CL fitting | KC screening, refractive surgery | KC diagnosis, post-surgery evaluation |
Sources: Kanski's Clinical Ophthalmology: A Systematic Approach, 10th Ed. | The Wills Eye Manual, Office and Emergency Room Diagnosis and Treatment of Eye Disease
This is a shared conversation. Sign in to Orris to start your own chat.