Open heart surgery
Reading File
Asking for Preferences
Finding Sources
Searching the Web
cardiopulmonary bypass mechanism components medical student overview
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Excellent - I have rich, comprehensive content. Now I have everything needed for a thorough, well-structured answer. Let me compile it.
Cardiopulmonary Bypass (CPB) - A Medical Student Guide
What is CPB?
Cardiopulmonary bypass is a technique that temporarily takes over the functions of both the heart (circulation) and the lungs (gas exchange), allowing surgeons to operate on a still, bloodless heart. It is the defining technology of open heart surgery.
The core principle: venous blood is diverted away from the right heart, oxygenated and CO2-removed by a machine, then returned to the patient's arterial system - bypassing the heart and lungs entirely.
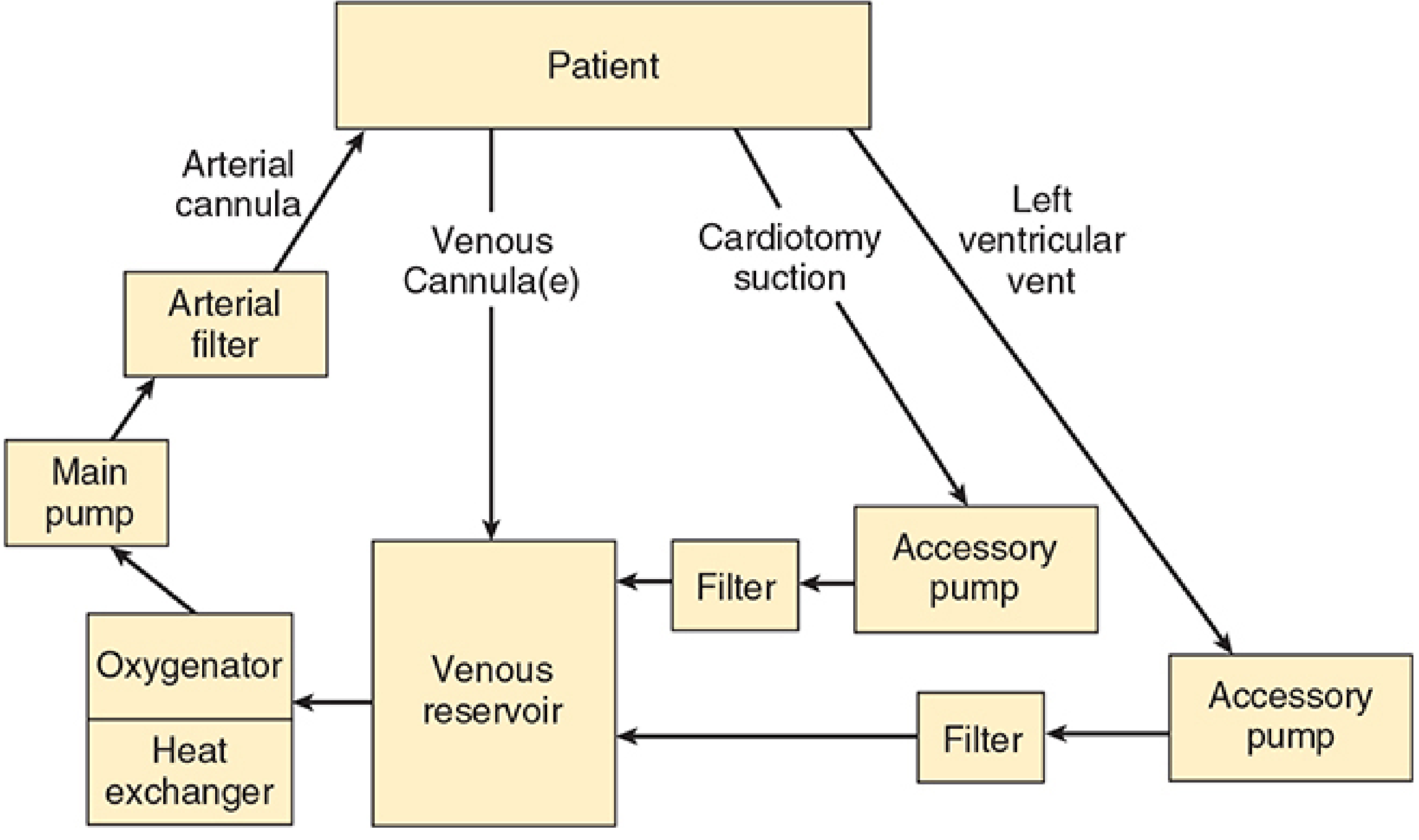
FIGURE: Basic design of a cardiopulmonary bypass machine (Morgan & Mikhail's Clinical Anesthesiology, 7e)
The CPB Circuit - 6 Core Components
| Component | Function |
|---|---|
| Venous cannula(e) | Drain blood from the right atrium/vena cava by gravity siphonage |
| Venous reservoir | Collects deoxygenated blood; acts as a buffer |
| Oxygenator | Gas exchange - adds O2, removes CO2 via a thin silicone membrane (modern "membrane oxygenator") |
| Heat exchanger | Cools or warms blood by water conduction; contains a bubble trap for rewarming |
| Main pump | Propels blood back to the patient (roller or centrifugal type) |
| Arterial filter | 20-40 µm mesh removes microemboli and debris before blood re-enters the patient |
Blood is returned via an arterial cannula placed in the ascending aorta (or femoral artery when the aorta is inaccessible).
Pump Types
- Roller pump: positive displacement; compresses tubing to produce near-continuous, nonpulsatile flow. Flow is directly proportional to RPM. Risk: if the reservoir empties, it will pump air into the patient.
- Centrifugal pump: spinning cones generate centrifugal force. Flow is pressure-sensitive and must be monitored with a flowmeter. Will not pump air (safer in that respect) but won't produce a defined volume per revolution.
Circuit Priming
Before use, the circuit is primed with 1200-1800 mL of fluid (adults), typically lactated Ringer's solution ± colloid, mannitol, heparin, and bicarbonate. This causes hemodilution at CPB onset, dropping hematocrit to ~22-27% in adults. Blood is added to the prime for neonates/infants and severely anemic adults to prevent dangerous hemodilution. - Morgan & Mikhail's Clinical Anesthesiology, 7e
How CPB is Established - Step by Step
- Sternotomy: vertical midline incision splitting the sternum exposes the heart and great vessels.
- Heparinization: systemic heparin is given (usually 300-400 units/kg) to prevent clotting in the circuit. The activated clotting time (ACT) must be > 480 seconds before bypass.
- Cannulation: venous cannula(e) placed in right atrium or vena cavae; arterial cannula placed in ascending aorta.
- Bypass initiated: venous blood drains by gravity into reservoir; the pump circulates it through the oxygenator and back to the aorta.
- Aortic cross-clamp: the ascending aorta is clamped, isolating the heart from the circulation.
- Cardioplegia: cardioplegic solution delivered to arrest the heart (see below).
- Surgery performed on a still, decompressed, blood-free heart.
- Weaning: the cross-clamp is removed, the heart resumes beating, bypass flow is gradually reduced as cardiac function returns.
- Decannulation + protamine: heparin is reversed with protamine sulfate after bypass ends.
Cardioplegia - Myocardial Protection
Cardioplegia is a chemical solution delivered into the coronary arteries (antegrade, via the aortic root) or coronary sinus (retrograde) to:
- Arrest the heart in diastole (high-potassium solution depolarizes cells and stops electrical activity)
- Reduce myocardial oxygen demand to near zero
- Protect cardiomyocytes from ischemic injury during the cross-clamp period
It is delivered cold (4°C) to provide additional metabolic protection via hypothermia. Topical ice-slush may also be used around the heart. - Pye's Surgical Handicraft, 22nd ed.
Hypothermia During CPB
Systemic cooling is routinely used to reduce metabolic demands during the ischemic period:
- Mild hypothermia: 32-35°C - minor protection
- Moderate hypothermia: 25-32°C - standard for most adult cardiac surgery
- Deep hypothermia with circulatory arrest (DHCA): 15-20°C - used for complex congenital repairs or aortic arch surgery; allows up to 60 minutes of complete circulatory arrest
Physiological Consequences of CPB
CPB produces distinctly nonphysiological conditions:
| Parameter | During CPB |
|---|---|
| Blood flow | Nonpulsatile (vs. normal pulsatile flow) |
| Mean arterial pressure | Usually 50-80 mmHg (below normal) |
| Hematocrit | Drops ~22-27% due to priming hemodilution |
| Systemic inflammatory response | Activated by blood-artificial surface contact |
Systemic Inflammatory Response
Contact of blood with the non-endothelial surfaces of the CPB circuit activates five plasma protein systems:
- Contact/kallikrein system
- Intrinsic coagulation pathway
- Extrinsic coagulation pathway
- Complement system
- Fibrinolytic pathway
This whole-body inflammatory response is responsible for many of CPB's postoperative complications. - TeachMeSurgery / Bailey & Love's
Complications of CPB
| Complication | Mechanism |
|---|---|
| Neurological injury (stroke, cognitive dysfunction) | Microemboli (air, fat, debris), hypoperfusion |
| Coagulopathy / bleeding | Dilution of clotting factors, platelet consumption, fibrinolysis |
| Acute kidney injury | Nonpulsatile flow, hemolysis, microemboli, inflammatory mediators |
| Pulmonary dysfunction | Inflammatory response, atelectasis, surfactant loss |
| Myocardial dysfunction | Ischemia-reperfusion injury, incomplete cardioprotection |
| Hemolysis | Mechanical trauma from roller pumps, cardiotomy suction |
| Air embolism | Reservoir runs dry (roller pump), inadequate de-airing |
Pharmacokinetic Effects on Drugs During CPB
CPB significantly alters drug pharmacokinetics - relevant for anesthetic management:
-
Increased volume of distribution: hemodilution expands the distribution volume for most drugs
-
Decreased plasma proteins: altered free drug fractions (e.g., fentanyl's unbound fraction rises at CPB onset)
-
Hypothermia: reduces enzymatic drug metabolism (e.g., remifentanil clearance falls ~6.4% per degree below 37°C)
-
Sequestration: some drugs bind to CPB circuit components
-
Miller's Anesthesia, 10e
Key Personnel
Operating the CPB machine requires a certified perfusionist - a specialist who manages pump flows, gas exchange, temperature, hematocrit, and anticoagulation in real-time. Optimal outcomes require close communication between the surgeon, anesthesiologist, and perfusionist throughout the case.
Quick Summary Table
| Step | Key Action | Key Drug/Device |
|---|---|---|
| Pre-bypass | Anticoagulation | Heparin (ACT > 480 s) |
| Cannulation | Establish venous/arterial access | Venous + arterial cannulae |
| Bypass | Heart-lung machine takes over | CPB circuit |
| Arrest | Electrically silence the heart | Cardioplegia (high-K+, cold) |
| Protection | Reduce metabolic demand | Hypothermia, cardioplegia |
| Wean | Restore cardiac function | Gradual reduction in pump flow |
| Reversal | Restore normal coagulation | Protamine sulfate |
This is a shared conversation. Sign in to Orris to start your own chat.