I now have comprehensive content from Robbins Pathology and Sleisenger & Fordtran. I have enough to write a thorough, well-structured answer covering all hepatitis topics from the user's list. Let me now compile the complete answer.
HEPATITIS - Complete Study Guide
Sources: Robbins & Kumar Pathologic Basis of Disease; Sleisenger and Fordtran's Gastrointestinal and Liver Disease; Goldman-Cecil Medicine; Yamada's Textbook of Gastroenterology
OVERVIEW: What is Hepatitis?
Hepatitis means inflammation of the liver. It can be caused by viruses (A, B, C, D, E), alcohol, drugs/toxins, autoimmune disease, or metabolic conditions. The five classic hepatotropic viruses (HAV, HBV, HCV, HDV, HEV) are the most important clinically. Understanding hepatitis is the foundation for understanding liver cirrhosis, portal hypertension, and all their downstream complications.
PART 1: ACUTE HEPATITIS
Definition
Acute hepatitis = liver inflammation lasting < 6 months. It can be asymptomatic or present with a full symptomatic illness.
Clinicopathologic Phases (applies to all hepatotropic viruses)
Symptomatic acute hepatitis goes through four phases:
- Incubation period - virus replicates silently; duration varies by virus (see table below)
- Preicteric (prodromal) phase - malaise, anorexia, nausea, vomiting, right upper quadrant discomfort, flu-like symptoms; serum transaminases (ALT, AST) begin to rise
- Icteric phase - jaundice appears (bilirubin rises), dark urine (conjugated bilirubin), pale stools, pruritus; ALT peaks here
- Convalescence - symptoms resolve, jaundice fades, enzymes normalize
Possible Outcomes of Acute Hepatitis
- Acute asymptomatic infection with recovery (subclinical - only detected by serology)
- Acute symptomatic infection with recovery (most common for HAV, HBV)
- Fulminant (acute) hepatic failure - massive hepatocyte necrosis, encephalopathy, coagulopathy (rare but life-threatening)
- Chronic hepatitis - inflammation persisting > 6 months (only HBV, HCV, HDV, HEV can do this)
- Asymptomatic carrier state (mainly HBV)
Lab Findings in Acute Hepatitis
| Test | Finding |
|---|
| ALT, AST | Markedly elevated (often >10x upper limit of normal) |
| Bilirubin | Elevated (conjugated + unconjugated) |
| ALP | Mildly elevated |
| PT/INR | Prolonged in severe disease (hepatocyte synthetic failure) |
| Albumin | Low in severe/prolonged disease |
Clinical pearl: ALT > AST in viral hepatitis. AST:ALT > 2:1 suggests alcoholic hepatitis.
PART 2: HEPATITIS A (HAV)
Virus Properties
- Small, nonenveloped, positive-strand RNA picornavirus (genus Hepatovirus)
- 27 nm icosahedral capsid
- Receptor on hepatocytes: HAVcr-1 (TIM-1)
- Not cytopathic - liver injury is caused by cytotoxic T lymphocytes and NK cells
Epidemiology
- Accounts for ~25% of clinically evident acute hepatitis worldwide
- Transmission: fecal-oral route - contaminated water, food (especially raw shellfish - oysters, mussels, clams), close personal contact
- Endemic in countries with poor hygiene and sanitation
- No chronic carrier state, no chronic hepatitis
- HAV shed in stool 2-3 weeks before and 1 week after onset of jaundice (maximum infectivity before jaundice)
- Blood-borne transmission is rare (transient viremia)
- Maternal-fetal transmission does NOT occur
Incubation Period
2-6 weeks
Clinical Features
- Nonspecific symptoms: fatigue, loss of appetite, nausea, RUQ pain
- Jaundice develops; most recover within 3 months, all by 6 months
- Acute liver failure (ALF): 0.1% to 0.3% - especially in those with underlying chronic liver disease
- Uncommon complications: prolonged cholestasis, relapse within 6 months
- Extrahepatic: rash, arthralgia, leukocytoclastic vasculitis, glomerulonephritis, cryoglobulinemia
Serology
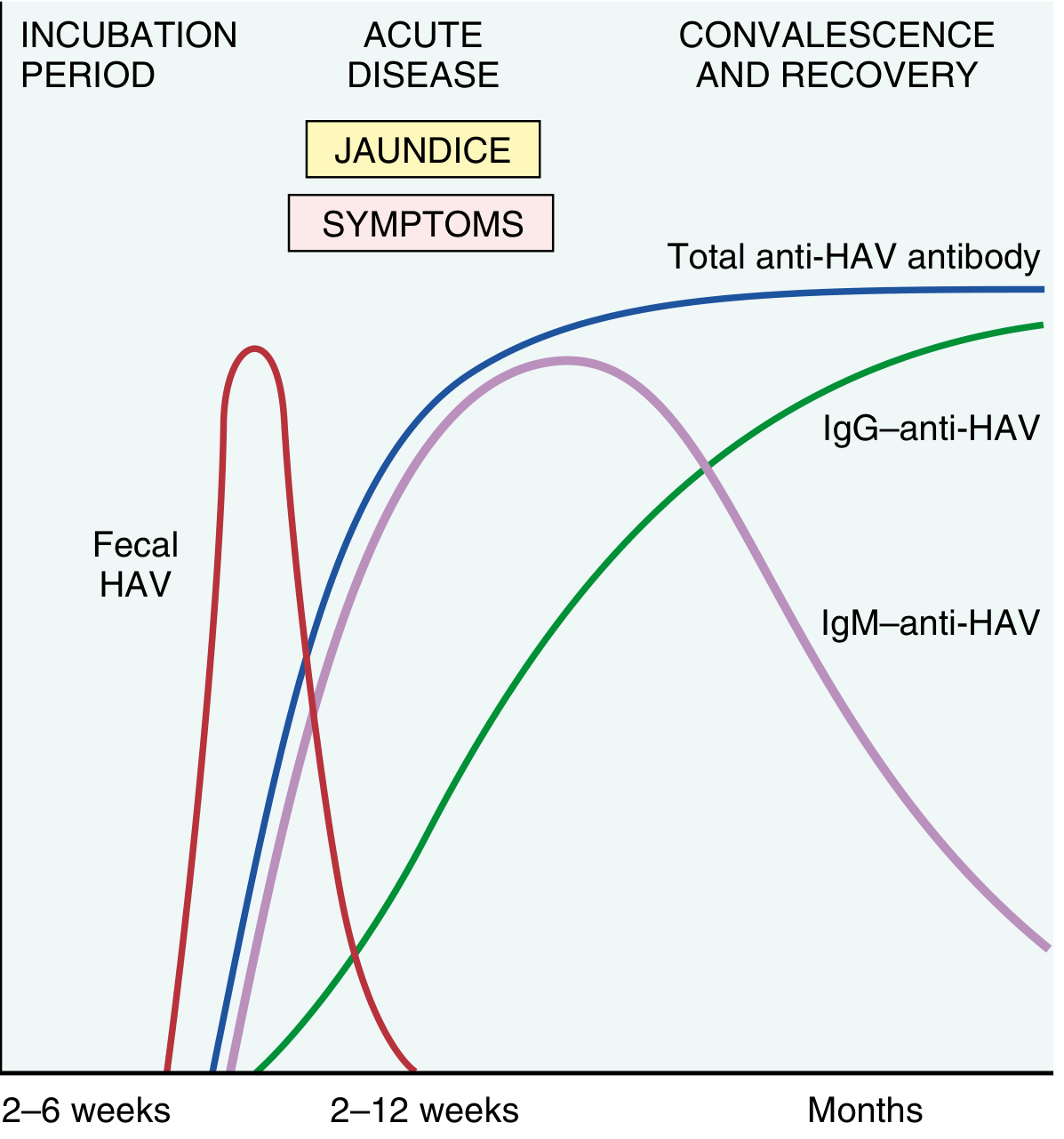
Fig. 18.9 from Robbins: Temporal changes in serologic markers in acute HAV infection
| Marker | Meaning |
|---|
| IgM anti-HAV | Appears at symptom onset; persists 3-6 months - diagnostic of acute infection |
| IgG anti-HAV | Appears during recovery; persists for years - lifelong immunity |
| Fecal HAV | Peak just before and at symptom onset |
Prevention
- HAV vaccine - highly effective
- Passive immunoglobulin for post-exposure prophylaxis
PART 3: HEPATITIS B (HBV)
Virus Properties
- Hepadnaviridae family
- Partially double-stranded circular DNA virus (only DNA hepatitis virus)
- The mature virion (Dane particle) has:
- Outer surface envelope: lipid + viral proteins
- Inner core: nucleocapsid (HBcAg), viral polymerase, viral DNA
Key HBV Antigens
| Antigen | What it is |
|---|
| HBsAg (surface Ag) | Viral envelope glycoproteins (large, middle, small); large HBsAg with complete virions; small HBsAg released in huge excess by infected hepatocytes (noninfectious particles) |
| HBcAg (core Ag) | Nucleocapsid protein; NOT detectable in serum (intracellular); longer transcript = HBeAg |
| HBeAg (e antigen) | Soluble secreted form of pre-core/core protein; marker of active viral replication and high infectivity |
| HBV DNA | Direct measure of viral replication |
Epidemiology
- 254 million people living with chronic HBV globally (WHO 2022); 1.2 million new infections/year; 1.1 million deaths/year
- Highest prevalence (>8%) in Africa, Asia, Western Pacific rim
- Transmission:
- Parenteral: blood transfusion (now rare due to screening), IV drug use
- Sexual transmission (most common in developed countries among young adults)
- Perinatal/vertical - dominant route in high-prevalence regions (accounts for 90% of cases in endemic areas)
- Horizontal: minor skin breaks, close bodily contact in children
Outcomes Based on Age of Acquisition
This is the most important concept for HBV:
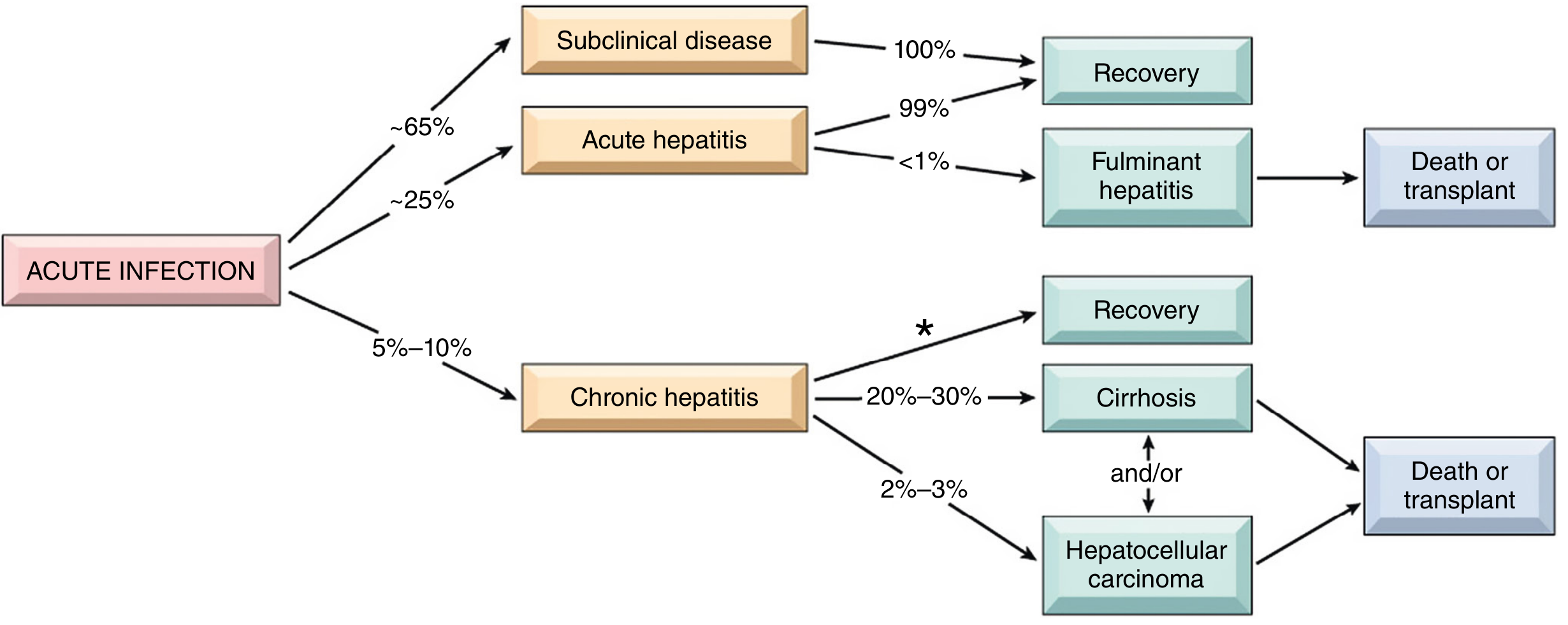
Fig. 18.10 from Robbins: Potential outcomes of HBV infection in adults
| Age at infection | Risk of chronic infection |
|---|
| Perinatal | 90-95% (immunologic tolerance) |
| First 5 years of life | ~30% |
| Adults (intact immune system) | 2-5% |
Incubation Period
4 weeks - 6 months (mean ~75 days)
Acute Hepatitis B
- Two-thirds: asymptomatic / subclinical (never recognized)
- One-third: symptomatic acute hepatitis (mild to moderate)
- Fulminant hepatic failure: ~1%; spontaneous survival rate only ~20% (liver transplant gives 50-60%)
- HBV accounts for 7% of all ALF cases
- Rapid viral elimination may cause HBsAg to clear before presentation - in these cases, diagnose by IgM anti-HBc
Chronic Hepatitis B
Definition: HBsAg positive for > 6 months
Natural history phases (key exam topic):
- Immune tolerant phase - high viral replication (HBeAg+, high HBV DNA), normal/near-normal ALT, minimal liver damage; common in perinatally infected persons
- Immune active (HBeAg-positive) phase - immune system attacks infected hepatocytes; elevated ALT, active necroinflammation, progressive fibrosis
- Inactive carrier phase - HBeAg seroconversion to anti-HBe; low HBV DNA, normal ALT, reduced inflammation; low but not zero risk of HCC
- HBeAg-negative chronic hepatitis B - reactivation with HBeAg-negative mutants; elevated ALT, elevated HBV DNA (but often lower), ongoing liver damage
Complications of chronic HBV:
- Cirrhosis develops in 20-30% of untreated active disease
- Annual risk of decompensation in HBV cirrhosis: 5-8%
- Annual risk of HCC: 2-4% in cirrhosis
- HCC can occur even WITHOUT cirrhosis (unique to HBV)
HBV Serologic Interpretation
| HBsAg | Anti-HBs | IgM Anti-HBc | IgG Anti-HBc | HBeAg | Interpretation |
|---|
| + | - | + | - | +/- | Acute HBV infection |
| - | - | + | + | - | Window period (HBsAg cleared, anti-HBs not yet appeared) |
| - | + | - | + | - | Past infection, recovered (immune) |
| - | + | - | - | - | Vaccinated (vaccine-induced immunity) |
| + | - | - | + | + | Chronic HBV, high replication |
| + | - | - | + | - | Chronic HBV, low replication / inactive carrier |
Window period: When HBsAg has disappeared but anti-HBs not yet detectable. The only positive marker is IgG anti-HBc. IgM anti-HBc distinguishes acute infection in this setting.
Treatment of HBV
- Goal: suppress HBV DNA, prevent progression to cirrhosis/HCC
- First-line antivirals: Tenofovir (TDF or TAF) or Entecavir - high potency, low resistance
- Pegylated interferon-alpha (Peg-IFN) - finite course but more side effects
- Indications: active disease (elevated ALT + elevated HBV DNA + significant fibrosis)
- Antiviral therapy does not eradicate cccDNA (functional cure rare; eradication currently impossible)
HBV Vaccination
- 3-dose recombinant vaccine; highly effective
- Universal infant vaccination has drastically reduced transmission
HCC Screening in Chronic HBV (Box 79.2, Sleisenger)
Screen with ultrasound ± AFP every 6 months in:
- African American carriers > 20 years
- Asian female carriers > 50 years
- Asian male carriers > 40 years
- Family history of HCC
- Any HBV cirrhosis
- Coinfection with HDV, HCV, or HIV
- Persistent active infection (high HBV DNA + ongoing liver injury)
PART 4: HEPATITIS C (HCV)
Virus Properties
- Flaviviridae family
- Enveloped, positive-strand RNA virus, single-stranded
- Life cycle entirely cytoplasmic (no nuclear integration) - this is why cure is possible
- 6 major genotypes (1-6); genotype 1 most common in Western countries
Epidemiology
- ~80 million infected worldwide
- Transmitted predominantly parenterally: IV drug use (most common in developed world), blood transfusions (now screened), needlestick injuries, tattoos
- Sexual transmission possible but less efficient than HBV
- Perinatal transmission: ~5-6% (increases with HIV co-infection)
- Increasing among women of childbearing age (opioid epidemic)
Incubation
2-26 weeks (mean ~7 weeks)
Acute Hepatitis C
- Mostly asymptomatic (60-70%)
- Symptomatic: mild jaundice, fatigue, nausea
- Spontaneous clearance occurs in 20-30% within 6 months
- The remaining 70-80% progress to chronic infection
- ALF is very rare with acute HCV
Chronic Hepatitis C
- Most patients asymptomatic until advanced fibrosis develops
- Symptoms: fatigue, vague abdominal pain, depression, arthralgias, paresthesias, myalgias
- ALT fluctuates; may be normal in ~20% at any given time
- ~20% progress to cirrhosis over 20 years (faster in men, with alcohol use, with HIV co-infection)
- HCC risk: primarily occurs in cirrhotics; 1-4% per year in HCV cirrhosis
Extrahepatic Manifestations of HCV
A distinctive feature - due to HCV-driven immune complex and lymphoproliferative disease:
- Mixed cryoglobulinemia (Types 2 and 3) - most characteristic; 19-50% have cryoglobulins, 5-10% have clinical symptoms
- Presents as: fatigue, arthralgia, purpura (palpable), Raynaud phenomenon, vasculitis, peripheral neuropathy, nephropathy
- Low complement (C4), positive rheumatoid factor, cryoglobulins
- Glomerulonephritis - especially membranoproliferative GN, membranous nephropathy
- Lichen planus
- Porphyria cutanea tarda
- Non-Hodgkin lymphoma (B-cell)
- Sicca syndrome
Diagnosis of HCV
- Anti-HCV antibody (ELISA) - screening test; detectable 4-10 weeks after infection
- HCV RNA by PCR - confirmatory; appears earlier (1-2 weeks after infection); used to monitor treatment
- HCV genotyping - guides treatment choice and duration
Treatment of HCV - Direct-Acting Antivirals (DAAs)
The revolution in HCV treatment:
- Direct-Acting Antivirals (DAAs) target HCV NS3/4A protease, NS5A replication complex, NS5B polymerase
- IFN-based regimens are no longer recommended
- Sustained Virologic Response (SVR) = undetectable HCV RNA 12-24 weeks after completing treatment
- SVR rates >95% with modern IFN-free DAA regimens; >99% of SVR patients are cured
- Key regimens: Sofosbuvir/ledipasvir, Sofosbuvir/velpatasvir, Glecaprevir/pibrentasvir
- Treatment also recommended for extrahepatic manifestations (cryoglobulinemia)
Unlike HBV, HCV can be cured because it does not integrate into the host genome
PART 5: HEPATITIS D (HDV)
Key Concept: HDV is a Satellite Virus
- HDV (the "delta agent") is a defective RNA virus that requires HBV for its life cycle
- It uses HBsAg as its own envelope protein - cannot infect without HBV
- Smallest genome of any known animal virus
- Delta antigen (HDAg) is the only viral protein produced
Epidemiology
- 5% of HBV-infected individuals are co-infected with HDV = ~15 million people worldwide
- Highest prevalence: Amazon basin, central Africa, Middle East, Mediterranean
- Rare in Southeast Asia and China
- Transmission: parenteral route (IV drug use, blood transfusions)
Clinical Patterns (Two Types)
1. Co-infection (HDV + HBV simultaneously):
- Presents as acute hepatitis indistinguishable from acute HBV
- Usually self-limited; both viruses clear
- Higher rate of fulminant hepatic failure in IV drug users
2. Superinfection (HDV infecting a chronic HBV carrier):
- Presents as severe acute hepatitis in HBsAg carrier, OR exacerbation of existing chronic HBV
- Chronic HDV infection in >80% of superinfections - much worse prognosis
- Accelerated progression to cirrhosis
Serology
- HBsAg positive (required for HDV to exist)
- IgM anti-HDV - most reliable indicator of recent HDV exposure
- HDV RNA detectable just before and during acute illness
PART 6: HEPATITIS E (HEV)
Virus Properties
- Unenveloped, positive-stranded RNA virus
- Hepeviridae family (genus Orthohepevirus)
- Genome 7.3 kb; four open reading frames
- Zoonotic disease - animal reservoirs include pigs, monkeys, cats, dogs
Epidemiology
- Fecal-oral transmission; waterborne epidemics
- Endemic in: Asia, Indian subcontinent, sub-Saharan Africa, Middle East, China, Mexico
- In India: accounts for >30% of sporadic acute hepatitis (exceeds HAV)
- In high-income countries: associated with pig farming or consumption of undercooked organ meat
- Can occur in travelers returning from endemic regions
Incubation
4-5 weeks (average)
Clinical Features
- Self-limited acute hepatitis in most cases; resolves in 2-4 weeks
- Immunocompetent: no chronic carrier state, no chronic hepatitis
- Most important: mortality ~20% in pregnant women (especially third trimester) - a classic exam fact
- Immunocompromised (AIDS, transplant recipients): can develop chronic HEV infection with progressive liver disease
Serology
- IgM anti-HEV and HEV RNA appear simultaneously with clinical symptoms
- IgM → replaced by persistent IgG anti-HEV during recovery
- HEV RNA detectable in stool and serum before onset of illness
PART 7: COMPARISON TABLE - All Hepatitis Viruses
| Feature | HAV | HBV | HCV | HDV | HEV |
|---|
| Virus type | RNA (Picornavirus) | DNA (Hepadnavirus) | RNA (Flavivirus) | RNA (defective) | RNA (Hepevirus) |
| Transmission | Fecal-oral | Parenteral, sexual, perinatal | Parenteral (mainly) | Parenteral (requires HBV) | Fecal-oral (waterborne) |
| Incubation | 2-6 weeks | 4 wks-6 months | 2-26 weeks | Same as HBV | 4-5 weeks |
| Chronic hepatitis? | No | Yes (2-95% depending on age) | Yes (~70-80%) | Yes (>80% superinfection) | Only immunocompromised |
| Carrier state? | No | Yes | Yes | Only with HBV | No (except immunocompromised) |
| Acute liver failure | 0.1-0.3% | <1% | Very rare | Higher with co-infection | Rare (except pregnancy ~20%) |
| HCC risk | No | Yes (even without cirrhosis) | Yes (mainly via cirrhosis) | Yes | No |
| Vaccine available | Yes | Yes | No | Prevented by HBV vaccine | Yes (some countries) |
| Treatment | Supportive | Tenofovir/Entecavir | DAAs (cure >95%) | Supportive; prevent HBV | Supportive (Ribavirin in immunocompromised) |
PART 8: CHRONIC HEPATITIS - General Concept
Definition
Hepatic inflammation lasting > 6 months, with risk of progressive fibrosis and cirrhosis.
Causes (in order of global importance)
- HBV
- HCV
- Autoimmune hepatitis
- Drug-induced (e.g., methotrexate, isoniazid, methyldopa)
- Wilson's disease, Alpha-1 antitrypsin deficiency
- Non-alcoholic steatohepatitis (NASH)
Histologic Grading and Staging
- Grade = degree of necroinflammatory activity (predicts current damage rate)
- Stage = degree of fibrosis (predicts prognosis and risk of cirrhosis)
- Staging systems: Metavir (F0-F4), Ishak (0-6)
- F4 = cirrhosis
Clinical Presentation
- Often asymptomatic for years (especially HCV)
- Fatigue, malaise, mild RUQ discomfort
- Hepatomegaly, splenomegaly (late)
- ALT elevated (fluctuating, especially in HCV)
- Jaundice, ascites, encephalopathy = signs of decompensation (advanced disease)
Assessment of Fibrosis (Stage)
- Liver biopsy - gold standard
- Non-invasive: FIB-4 score, APRI score, FibroScan (transient elastography)
PART 9: PATHOLOGY OF HEPATITIS (Key Histological Findings)
Acute Hepatitis (all viral types)
- Hepatocyte swelling (ballooning degeneration)
- Councilman (acidophilic) bodies = apoptotic hepatocytes; eosinophilic, shrunken
- Lobular disarray - disruption of normal hepatic architecture
- Mononuclear cell infiltrate (lymphocytes, macrophages) in portal tracts and lobule
- Kupffer cell hyperplasia
- Cholestasis (bile plugs) in severe cases
Chronic Hepatitis
- Portal tracts expanded by lymphocytic infiltrate
- Interface hepatitis (piecemeal necrosis) = lymphocytes spill into periportal hepatocytes - hallmark of activity
- Bridging fibrosis (F3): fibrous septa connect portal tracts to central veins
- Periportal fibrosis → bridging fibrosis → cirrhosis (progression)
- "Ground glass" hepatocytes in HBV = cytoplasm stuffed with HBsAg (smooth ER hypertrophy)
Fulminant Hepatitis
- Massive hepatic necrosis - large confluent zones of hepatocyte death
- Collapsed reticulin framework
- Bile duct proliferation in portal tracts
PART 10: CHRONIC HEPATITIS → CIRRHOSIS (The Progression Story)
This is the central theme of all hepatology:
Active hepatitis (ongoing inflammation) → fibrosis accumulation (stellate cell activation, collagen deposition) → cirrhosis (diffuse nodular regeneration + fibrous septa → loss of normal architecture) → portal hypertension + hepatic synthetic failure + HCC risk
Key factors accelerating progression:
- Male sex, older age at infection
- High viral load (HBV DNA, HCV RNA)
- Alcohol use (synergistic with both HBV and HCV)
- HIV co-infection
- HDV co-/super-infection
- Non-alcoholic fatty liver disease
PART 11: HEPATITIS AND THE DOWNSTREAM GI/HEPATOLOGY COMPLICATIONS
The remaining items on your Gastroenterology list all flow from the progression of chronic hepatitis to cirrhosis and its complications:
| Complication | Mechanism Link to Hepatitis |
|---|
| Liver cirrhosis | End result of chronic HBV/HCV - diffuse fibrosis + nodular regeneration |
| Portal hypertension | Cirrhosis → increased intrahepatic vascular resistance → raised portal venous pressure |
| Ascites | Portal hypertension + hypoalbuminemia + splanchnic vasodilation → fluid in peritoneal cavity |
| Hepatic encephalopathy | Liver synthetic failure → toxins (ammonia etc.) bypass liver → CNS dysfunction |
| Spontaneous bacterial peritonitis (SBP) | Ascites fluid becomes infected (E. coli, Klebsiella) - complication of cirrhotic ascites |
| Upper GI bleeding | Portal hypertension → esophageal/gastric varices → rupture; also portal hypertensive gastropathy |
| HCC | Chronic HBV/HCV + cirrhosis → hepatocellular carcinoma |
QUICK-REFERENCE: Exam Memory Aids
"Which hepatitis can become chronic?" → B, C, D (and E in immunocompromised)
"Which can cause HCC?" → B (even without cirrhosis) and C (mainly via cirrhosis)
"Which is fatal in pregnancy?" → E (~20% mortality in third trimester)
"Which needs HBV to replicate?" → D (delta agent, satellite virus)
"Which is curable with drugs?" → C (DAAs, >95% SVR)
"Window period serology?" → Only IgG anti-HBc positive (HBsAg gone, anti-HBs not yet appeared)
"How to diagnose acute HBV in window period?" → IgM anti-HBc
"Newborn exposed to HBsAg-positive mother?" → Give HBIG + HBV vaccine within 12 hours of birth
"ALT vs AST?" → Viral hepatitis: ALT > AST. Alcoholic hepatitis: AST:ALT > 2:1
Sources:
- Robbins & Kumar Pathologic Basis of Disease (Robbins Pathology), Ch. 18
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease, Chs. 79-81
- Goldman-Cecil Medicine International Edition, Vol. 2
- Yamada's Textbook of Gastroenterology, 7th ed.