Amyotrophic lateral scloresuis details answer with pt mangement and assessment
"amyotrophic lateral sclerosis"[MeSH Terms] AND management
Amyotrophic Lateral Sclerosis (ALS) - Comprehensive Overview
Definition
- Bradley and Daroff's Neurology in Clinical Practice
- Goldman-Cecil Medicine
Epidemiology
| Feature | Data |
|---|---|
| Incidence | ~2 per 100,000/year |
| Prevalence | 5-8 per 100,000 |
| Peak age at onset | 55-74 years |
| Male:Female ratio | ~1.6:1 (slight female predominance in bulbar-onset) |
| Sporadic vs Familial | ~90% sporadic, 5-10% familial |
| Mean survival | 2-5 years from symptom onset |
| Familial inheritance | Usually autosomal dominant |
Pathogenesis
Genetic Causes
- C9ORF72 hexanucleotide repeat expansion (GGGGCC) on chromosome 9: accounts for 40-50% of familial ALS and 7-10% of sporadic ALS - the most common genetic cause
- SOD1 mutations (chromosome 21q22.1): 20% of familial ALS, 2% overall - generates misfolded protein triggering oxidative stress, protein aggregation, mitochondrial dysfunction, excitotoxicity
- TDP-43 (TARDBP gene) and FUS/TLS - RNA-binding proteins; mutations in these converge on defective RNA processing as a shared mechanism
- Other loci: alsin, senataxin, angiogenin, VAPB, dynactin, TBK1
Key Pathogenic Mechanisms
- Oxidative stress
- Protein aggregation (SOD1 misfolding, TDP-43 inclusions)
- Mitochondrial dysfunction
- Excitotoxicity (glutamate toxicity)
- Impaired axonal transport
- Defective RNA processing
- Non-neuronal cell contribution - astrocytes expressing mutant SOD1 exert toxic effects on neighboring motor neurons
- Goldman-Cecil Medicine, Robbins & Kumar Basic Pathology
Pathology
- Atrophy of the precentral gyrus (motor cortex)
- Sclerosis and pallor of the corticospinal tracts in the spinal cord
- Thin gray anterior (ventral) spinal roots and hypoglossal nerves
- Visible muscle atrophy
- Loss of >50% of spinal anterior horn motor neurons
- Diffuse astrocytic gliosis in spinal gray matter
- Large motor unit potentials on EMG; fibrillation and positive sharp waves
- TDP-43 cytoplasmic inclusions in a subset of cases
- Spared regions: extraocular muscles, Onuf's nucleus in sacral cord (pelvic floor - bowel/bladder continence preserved until late)
Classification of ALS
- Classic spinal-onset ALS
- Bulbar-onset ALS (~25% of cases)
- Flail-arm variant (bilateral upper extremity, more common in males)
- Flail-leg variant
- Primary Lateral Sclerosis (PLS) - UMN only
- Progressive Muscular Atrophy (PMA) - LMN only
- Progressive Bulbar Palsy (PBP)
- Mills hemiplegic variant
- Respiratory/dyspnea onset (~1-2%, predominantly male)
- Monomelic presentation
- ALS1: SOD1 mutations, chr 21q22.1, AD
- ALS2: Alsin mutations, chr 2q33, AR, juvenile
- ALS4: Senataxin, chr 9q34, AD, juvenile
- ALS6: FUS/TLS
- ALS-FTD: C9ORF72 expansion (also causes frontotemporal dementia)
Clinical Features
Upper Motor Neuron Signs
- Spasticity and hypertonia
- Hyperreflexia (paradoxically brisk reflexes in wasted limbs)
- Pathological reflexes: Babinski sign, Hoffman sign
- Pseudobulbar palsy: emotional lability, brisk jaw jerk, strained "strangled" speech
- Loss of dexterity
- Clonus
Lower Motor Neuron Signs
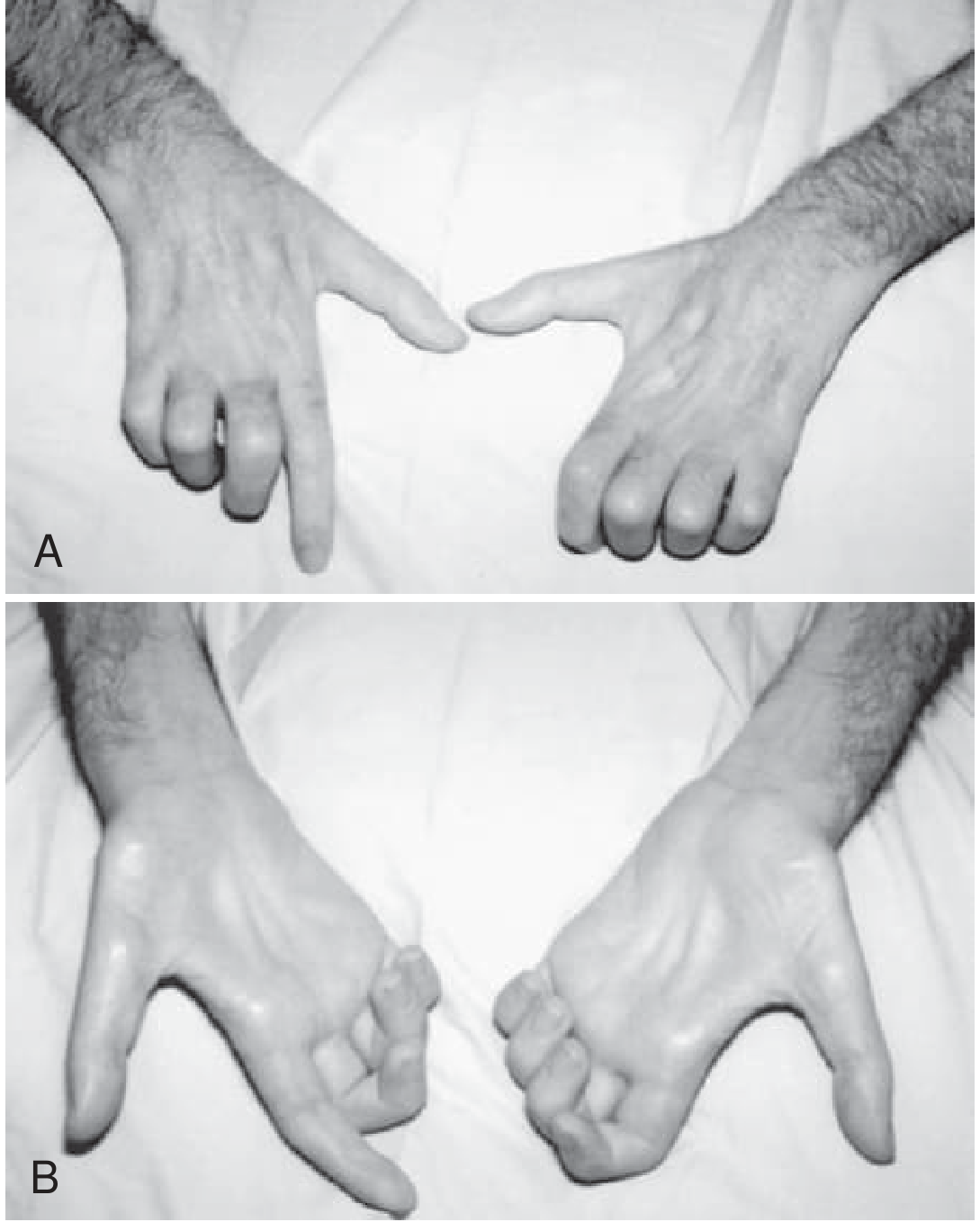
- Weakness and progressive muscle wasting (amyotrophy)
- Fasciculations (most noticeable in large proximal muscles)
- Reduced or absent reflexes in severely affected muscles
- Flaccid dysarthria with nasal quality
- Muscle cramps (often an early symptom)
Classic Presentation Pattern
- Onset typically focal, distal, asymmetric in one limb
- Spreads in anatomically contiguous progression
- Upper limb onset: difficulty turning keys, buttoning, opening bottles; thenar and intrinsic hand muscles most affected
- Lower limb onset: foot drop, gait instability
- Bulbar onset (25%): slurred speech initially when tired, progressing to dysarthria, dysphagia (liquids before solids), sialorrhea, weight loss, aspiration risk
- Respiratory onset (rare): presents to pulmonologist, may fail ventilator weaning
Features Usually Preserved (Clinically Important)
- Eye movements (EOMs)
- Bowel and bladder continence (pelvic floor via Onuf's nucleus)
- Sensation (sensory pathways usually spared)
Cognitive/Behavioral Features
- Overt frontotemporal dementia (FTD) in ~5%
- Subtle frontal lobe dysfunction in up to 50%
- C9ORF72 variant: higher risk of cognitive/behavioral disturbances and family history of dementia
Respiratory Progression
- Insidious diaphragmatic weakness causing dyspnea and orthopnea
- Paradoxical abdominal wall movement during inspiration
- Nocturnal CO2 retention: interrupted sleep, morning headaches, anorexia, daytime somnolence
- Ultimate cause of death: respiratory failure
Assessment
Diagnostic Criteria - El Escorial / Awaji Criteria
| Diagnostic Level | Criteria |
|---|---|
| Clinically Definite ALS | Clinical or electrophysiologic UMN and LMN signs in ≥3 regions |
| Clinically Probable ALS | UMN and LMN signs in ≥2 regions, with some UMN signs rostral to LMN signs |
| Clinically Possible ALS | UMN and LMN in only 1 region, OR UMN signs alone in ≥2 regions, OR LMN signs rostral to UMN signs |
Investigations
- EMG (mandatory): Active denervation (fibrillation potentials, positive sharp waves, fasciculation potentials) + chronic denervation (large motor unit potentials) in multiple regions not explainable by single nerve/root lesion
- Nerve conduction studies: Usually normal; exclude multifocal motor neuropathy
- CBC, ESR, CRP
- Serum calcium, thyroid function, parathyroid hormone
- Serum protein electrophoresis (SPEP)
- Creatine kinase (CK) - may be mildly elevated
- Anti-GM1 ganglioside antibodies and anti-MAG antibodies
- Acetylcholine receptor antibody (if myasthenia suspected)
- VDRL, HIV
- Heavy metal screen, urinary porphyrins
- Hexosaminidase A and B
- Borrelia titers
- MRI brain and spinal cord - to exclude structural causes (compression, tumor)
- Forced Vital Capacity (FVC) - supine position is more sensitive for diaphragmatic weakness
- FVC <50% predicted: indicates need for non-invasive ventilation (NIV)
- SNIP (Sniff Nasal Inspiratory Pressure)
- Peak cough flow
- Offered to both familial and sporadic cases in the current era of emerging gene therapy trials
- Only for atypical cases where diagnostic uncertainty persists
- Shows neurogenic atrophy
ALS Mimic Conditions to Exclude
- Multifocal motor neuropathy with conduction block
- Kennedy disease (spinal/bulbar muscular atrophy)
- Myasthenia gravis
- Cervical/lumbar myeloradiculopathy
- Spinal muscular atrophy (SMA)
- Paraneoplastic motor neuron syndrome
- Heavy metal toxicity
- Hyperthyroidism
Patient Management
1. Multidisciplinary Team (MDT) - Cornerstone of Care
- Neurologist
- Nurse specialist / ALS care coordinator
- Occupational therapist (OT)
- Physiotherapist
- Speech and language therapist (SLT)
- Dietitian
- Social worker
- Psychologist/psychiatrist
- Palliative care team
- Respiratory physician
2. Disease-Modifying Pharmacotherapy
| Drug | Mechanism | Effect |
|---|---|---|
| Riluzole (sodium glutamate antagonist) | Blocks glutamate release, reduces excitotoxicity | Extends survival ~2-3 months; slows decline; standard of care |
| Edaravone | Free radical scavenger, reduces oxidative stress | Confirmed in double-blind RCT; slows functional decline in selected patients |
| Tofersen (antisense oligonucleotide) | Targets SOD1 mRNA; reduces mutant SOD1 protein | For SOD1-ALS; emerging gene therapy approach |
| AMX0035 (sodium phenylbutyrate + taurursodiol) | Anti-apoptotic, mitochondrial protective | FDA approved 2022 for ALS |
3. Symptomatic Management
| Symptom | Pharmacotherapy | Non-pharmacological |
|---|---|---|
| Spasticity | Baclofen, tizanidine, dantrolene, diazepam | Physiotherapy, range-of-motion exercises, botulinum toxin |
| Muscle cramps | Quinine sulfate, baclofen, vitamin E, clonazepam | Massage, physiotherapy |
| Fatigue | Pyridostigmine, amantadine, modafinil, methylphenidate, antidepressants | Energy conservation, work modification, BiPAP if sleep apnea |
| Sialorrhea (drooling) | Hyoscyamine, glycopyrrolate, scopolamine patch, diphenhydramine, atropine | Suction machine, botulinum toxin into salivary glands, parotid gland radiation |
| Thick phlegm | Nebulized N-acetylcysteine, nebulized saline, propranolol | Insufflation-exsufflation (cough assist), cool mist humidifier |
| Pseudobulbar affect | TCAs, SSRIs, lithium, mirtazapine, quinidine/dextromethorphan (Nuedexta) | |
| Depression/anxiety | TCAs, SSRIs, venlafaxine, mirtazapine, bupropion | Counseling, support groups |
| Pain/joint pain | NSAIDs, analgesics | Range-of-motion exercises, heat |
| Fasciculations | Carbamazepine | Reassurance |
| Jaw clenching | Benzodiazepines | Botulinum toxin into masseters |
| Aspiration | Cisapride | Modified food consistency, thickened liquids, tracheostomy in severe cases |
| Insomnia | Zolpidem, zopiclone, TCAs | Sleep hygiene, BiPAP |
4. Nutritional Management
- Early referral to dietitian; monitor weight regularly
- Dysphagia management: modified diet textures, thickened liquids
- Percutaneous Endoscopic Gastrostomy (PEG): recommended when:
- FVC >50% (timing is critical - too late if respiratory compromise)
- Significant weight loss (>10%) or dysphagia compromising nutrition
- Prolonged meal times with aspiration risk
- High-calorie diet to maintain BMI and body weight (emerging evidence that caloric supplementation may slow progression)
5. Respiratory Management
- Serial FVC monitoring at every clinic visit
- Non-Invasive Ventilation (NIV / BiPAP):
- Indicated when FVC <50% or symptomatic orthopnea/dyspnea
- Extends survival and improves quality of life
- Also beneficial for sleep-disordered breathing
- Cough Assist Device (mechanical insufflation-exsufflation): for patients with impaired cough and secretion clearance
- Tracheostomy and invasive ventilation: discussed as advance care planning; extends life but requires intensive nursing/family care
6. Speech and Communication Management
- SLT assessment for dysarthria and dysphagia
- Low-tech aids: letter boards, writing
- Augmentative and Alternative Communication (AAC): voice amplifiers, speech-generating devices
- Eye-tracking devices (e.g., Tobii) for late-stage communication when limb function lost
- Banking the patient's natural voice early for later synthesis
7. Physical Rehabilitation
- Physiotherapy: Range-of-motion exercises, stretching, energy conservation; moderate exercise (not exhaustive)
- Resist overexertion - exercise should not cause post-exercise fatigue lasting >30 min
- Orthotics/adaptive devices: ankle-foot orthoses for foot drop, wrist splints, neck collars for head drop
- Occupational therapy: home adaptations, specialized wheelchairs, pressure-relieving mattresses, ceiling hoists
8. Ethical, Legal, and Advance Care Planning
- Early discussion of advance directives and healthcare proxy
- Decisions regarding NIV, PEG, invasive ventilation, and resuscitation should be made while the patient has capacity
- ALS requires repeated reassessment of goals of care as disease progresses
- Palliative/hospice care: symptom control, pain management, and psychosocial support - can be introduced early, not just end-of-life
9. Psychosocial Support
- Patient and family education about disease trajectory
- Access to ALS associations and support groups (e.g., ALS Association, Motor Neurone Disease Association)
- Psychological support for patient and caregivers
- Caregiver burden assessment and respite care
Prognosis
- Mean survival: 2-5 years from symptom onset
- ~10% of patients survive >10 years (long-term survivors)
- Better prognosis: younger onset, limb-onset (vs bulbar), slower rate of FVC decline
- Worse prognosis: bulbar onset, rapid FVC decline, older age at onset, early respiratory involvement
- Death is usually due to respiratory failure (aspiration pneumonia or ventilatory failure)
Recent Evidence (2024-2026)
- Physical therapy for global function in ALS (PMID 39182937, BMJ Open 2024): Meta-analysis supports physiotherapy for improving quality of life and reducing fatigue
- Respiratory muscle training in ALS (PMID 40488544, 2025): Systematic review/meta-analysis shows respiratory muscle training improves pulmonary function and may extend survival
- Management of cramping in ALS (PMID 41042709, 2025): Systematic review of cramp management strategies in ALS
Physiotherapy assessment and management
"amyotrophic lateral sclerosis"[MeSH Terms] AND "physical therapy"[MeSH Terms]
"amyotrophic lateral sclerosis" AND "exercise" AND rehabilitation
PMID: 38762656
PMID: 40273110
PMID: 41375893
PMID: 39182937
PMID: 40488544
PMID: 42038869
Physiotherapy Assessment and Management in ALS
Role of Physiotherapy in ALS
Part 1: Physiotherapy Assessment
1.1 Initial Assessment Framework
1.2 Subjective Assessment (History)
- Presenting complaints: pattern of weakness, location of symptom onset (limb vs. bulbar vs. respiratory)
- Functional limitations: ADL performance, gait, transfers, self-care
- Fatigue: onset, severity, aggravating/relieving factors, relationship to activity
- Respiratory symptoms: dyspnea on exertion/rest, orthopnea, morning headaches, excessive daytime sleepiness
- Pain: joint pain, cramps, spasticity-related discomfort
- Falls history: frequency, circumstances
- Home environment: stairs, accessibility, available caregivers
- Assistive devices currently in use
- Patient priorities and goals: what activities matter most to the patient
- Psychosocial status: anxiety, depression, caregiver burden
1.3 Objective Assessment
A. Muscle Strength Testing
- MRC (Medical Research Council) Scale - grade 0-5 for all major muscle groups
- Upper limbs: shoulder abductors, elbow flexors/extensors, wrist extensors, intrinsic hand muscles (thenar - most commonly affected early)
- Lower limbs: hip flexors, knee extensors/flexors, ankle dorsiflexors (foot drop assessment), plantar flexors
- Neck flexors and extensors (head drop assessment)
- Respiratory muscles: see below
- Document asymmetry and pattern (distal > proximal typically)
B. Tone and Spasticity
- Modified Ashworth Scale for spasticity in UMN-predominant cases
- Check for clonus, pathological reflexes (Babinski, Hoffman)
- Identify impact of spasticity on function and positioning
C. Range of Motion (ROM)
- Goniometric measurement of joint ROM
- Identify contractures (shoulder, ankle, wrist, finger flexors - common in weak/spastic limbs)
- Passive ROM assessment when active movement is limited
D. Functional Mobility Assessment
- Timed Up and Go (TUG) - gait speed and transfer ability
- 10-Metre Walk Test - preferred gait speed
- 6-Minute Walk Test (6MWT) - functional endurance (if feasible early-stage)
- Sit-to-stand transfers
- Stair climbing ability
- Bed mobility and rolling
E. Balance Assessment
- Berg Balance Scale (BBS) - static and dynamic balance
- Romberg test, tandem standing
- Risk of falls - STRATIFY scale
F. Respiratory Assessment (Critical - done at every visit)
- Forced Vital Capacity (FVC): the primary measure of respiratory function
- FVC in seated AND supine positions (supine FVC more sensitive for diaphragmatic weakness; a >25% drop from sitting to supine is significant)
- Refer for NIV when FVC <50% predicted (or earlier if symptomatic)
- Sniff Nasal Inspiratory Pressure (SNIP): sensitive measure of inspiratory muscle strength; <40 cmH₂O significant
- Maximal Inspiratory Pressure (MIP) and Maximal Expiratory Pressure (MEP)
- MEP <60 cmH₂O: impaired cough
- MIP <60 cmH₂O: inspiratory muscle weakness
- Peak Cough Flow (PCF):
- <270 L/min: increased risk of secretion retention
- <160 L/min: ineffective cough; cough assist device needed
- Observation for paradoxical breathing (diaphragm weakness)
- Signs of nocturnal hypoventilation: morning headaches, daytime somnolence, fragmented sleep
G. Fatigue Assessment
- Fatigue Severity Scale (FSS) - 9-item scale; score >36 indicates significant fatigue
- ALS-specific Fatigue Scale
- Pattern: is fatigue post-exertional? Does it exceed 30 min recovery? (Key safety threshold)
H. Pain Assessment
- Visual Analog Scale (VAS) or Numerical Rating Scale (NRS) for pain intensity
- Location, type (spasticity-related, joint/mechanical, neuropathic, pressure sore)
- Impact on function and sleep
I. Global Functional Rating
- ALSFRS-R (ALS Functional Rating Scale - Revised): the gold-standard, 12-item scale tracking:
- Speech, salivation, swallowing
- Handwriting, cutting food, dressing/hygiene
- Turning in bed
- Walking, climbing stairs
- Dyspnea, orthopnea, respiratory insufficiency
- Score 0-48; rate of change (decline >1 point/month = faster progression)
J. Postural and Gait Analysis
- Foot drop, steppage gait, Trendelenburg gait
- Head drop (cervical/thoracic paraspinal weakness)
- Trunk stability
- Identify orthotic needs
K. Upper Limb Function
- Grip strength (dynamometry)
- Pinch strength
- Assessment of intrinsic hand muscle atrophy (thenar/hypothenar wasting; "claw hand")
- Fine motor tasks: writing, buttoning, key-turning
1.4 Staging Systems for Assessment Guidance
| Stage | Features | Physio Focus |
|---|---|---|
| Stage 1 | Diagnosis; independently ambulant; minor deficits | Exercise, education, prevention |
| Stage 2a | Independent but with some functional limitation | Adaptive exercise, orthotics |
| Stage 2b | Dependent for some ADLs; still ambulant | Energy conservation, wheelchair |
| Stage 3 | Wheelchair dependent; upper limb function reduced | Positioning, passive ROM, respiratory |
| Stage 4 | Dependent for most ADLs | Pressure care, carer training |
| Stage 5 | End-stage; respiratory support, minimal movement | Comfort, palliative, communication |
Part 2: Physiotherapy Management
Overarching Principles
- Tailor exercise intensity to the individual - ALS muscles are vulnerable to overwork injury
- Avoid post-exercise fatigue lasting >30 minutes (key safety rule)
- Moderate exercise is beneficial; exhaustive exercise is harmful
- Adapt interventions at every visit as disease progresses
- Empower the patient and family/caregivers through education
- Set realistic, meaningful, patient-centred goals
2.1 Exercise Prescription
A. Strengthening Exercise
- Evidence is emerging but not yet definitive for strength gains due to small trial sizes and disease heterogeneity
- 2025 systematic review and meta-analysis (PMID: 40273110) found no clear superiority of strengthening over control in short-term outcomes, but no serious adverse events were reported - supporting safety
- Current practice:
- Moderate-intensity resistance training targeting relatively preserved muscle groups
- Avoid training severely wasted or denervated muscles
- Submaximal loads (60-70% max); high reps/low load preferable
- Focus on functional strength: grip, hip stabilizers, knee extensors
- Avoid eccentric-dominant exercises in weak muscles
- Frequency: 3-5 days/week
- Monitor carefully: if increased weakness or fatigue >30 min post-exercise - reduce load
B. Aerobic / Cardiovascular Exercise
- Moderate-intensity aerobic exercise is beneficial:
- Cycling (stationary bike - supported), swimming, walking
- Maintain cardiovascular health and reduce fatigue
- Low-impact options preferred as gait safety declines
- Perceived exertion (RPE) 11-13 on Borg scale (light-to-somewhat-hard)
- Network meta-analysis 2024 (PMID: 38762656): Exercise intervention had the strongest positive effect on ALSFRS-R score (SMD 1.01), FVC (SMD 0.78), quality of life, and MRC sum score among all non-pharmacological interventions in ALS
C. Flexibility and Range-of-Motion Exercises
- Daily passive and active-assisted ROM for all joints
- Priority joints: shoulder, ankle (plantarflexion contracture), hip flexors, wrist/finger flexors
- Stretching for spastic muscles (slow, sustained stretches)
- Prevents contractures and reduces pain from stiffness
- Family/carer education in ROM techniques for home program
D. Aquatic Therapy / Hydrotherapy
- Warm water buoyancy reduces gravitational load - allows movement in patients who cannot exercise on land
- Reduces spasticity, improves comfort and mood
- Suitable in early-to-middle stages (respiratory safety in water requires monitoring)
- Requires supervision; contraindicated if respiratory compromise is significant
2.2 Respiratory Physiotherapy
A. Inspiratory Muscle Training (IMT)
- Device-based (threshold loader, e.g., Threshold IMT)
- Trains inspiratory muscles to improve endurance and strength
- 2025 systematic review and meta-analysis (PMID: 40488544): Respiratory muscle training improved maximum inspiratory pressure (MIP) and maximum expiratory pressure (MEP). One study showed inspiratory muscle training as a survival predictor. No adverse events reported.
- Current recommendation: start early when FVC still >70%
B. Expiratory Muscle Training (EMT)
- Improves cough peak flow and secretion clearance
- Target MEP and PCF monitoring
C. Airway Clearance Techniques
- Manually Assisted Cough (MAC): physiotherapist or carer applies abdominal thrust timed with cough effort
- Mechanical Insufflation-Exsufflation (MIE / Cough Assist):
- Delivers positive pressure breath then rapidly reverses to negative pressure
- Simulates a cough; most effective airway clearance intervention in ALS
- Indicated when PCF <270 L/min; essential when PCF <160 L/min
- Can be used via face mask, mouthpiece, or tracheostomy
- Also used during chest infections when secretion retention is dangerous
- Glossopharyngeal breathing (frog breathing): air stacking technique to augment lung volumes
- Lung Volume Recruitment (LVR) / Air Stacking: patient takes multiple insufflations via resuscitation bag or glossopharyngeal breathing to inflate lungs beyond what inspiration alone can achieve; helps maintain lung compliance and improves cough effectiveness
- High-frequency chest wall oscillation (HFCWO): vest device that vibrates the chest wall to mobilize secretions (e.g., The Vest system)
- Postural drainage: limited use but positioning can assist in selected patients
D. Breathing Pattern Retraining
- Diaphragmatic breathing education (while diaphragm function preserved)
- Positioning: upright/semi-reclined posture optimizes diaphragm mechanics; avoid supine in patients with orthopnea
- Pursed lip breathing for dyspnea management
E. Non-Invasive Ventilation (NIV) Initiation
- Physiotherapist plays a key role in:
- Mask fitting and interface selection (nasal, oronasal, full face)
- Titrating patient comfort with BiPAP settings
- Education of patient and carers in NIV use
- Monitoring compliance and troubleshooting (mask leak, interface intolerance)
- NIV is indicated when: FVC <50%, SNIP <40 cmH₂O, MIP <60 cmH₂O, or symptomatic orthopnea/morning headaches
- NIV extends survival and improves quality of life - one of the most important interventions in ALS
2.3 Spasticity Management
- Physiotherapy is first-line before pharmacotherapy where possible
- Slow, sustained stretching (30-60 seconds holds)
- Hydrotherapy for spasticity relief
- Orthoses (ankle-foot orthosis, resting hand splints) to maintain length
- Positioning: careful positioning in chair/bed to avoid spasm
- Cryotherapy: ice packs temporarily reduce spasticity
- Adjunct: pharmacological (baclofen, tizanidine) or botulinum toxin for focal spasticity
2.4 Gait and Mobility Management
- Gait retraining: compensatory strategies for foot drop, hip weakness
- Ankle-Foot Orthosis (AFO): for foot drop; improves gait safety and reduces fall risk
- Walking aids: walking stick, quad stick, rollator frame (with forearm support if grip weak)
- Fall prevention: home hazard assessment, removal of rugs/thresholds, installation of grab rails
- Energy conservation: teach activity pacing
- Continue gait aids; upgrade to rollator or forearm crutches
- Stair management advice; plan for stair-free access
- Teach safe sit-to-stand transfers with carer
- Powered wheelchair prescription: joystick, sip-and-puff, head-switch control as upper limb function declines
- Manual wheelchair for short distances or carer-propelled
- Tilt-in-space wheelchair for trunk control and pressure relief
2.5 Positioning and Pressure Care
- 24-hour postural management plan: coordinate with OT
- Regular repositioning to prevent pressure injuries (every 2 hours in bedbound patients)
- Pressure-relieving mattresses: dynamic air mattress, memory foam
- Pressure-relieving wheelchair cushions (e.g., ROHO air cushion)
- Head support: headrest, cervical collar (soft collar or rigid for dropped head syndrome) - balance between neck support and patient comfort
- Trunk support: thoracic supports, lateral trunk supports in wheelchair
2.6 Upper Limb Management
- Functional upper limb exercises while strength preserved
- Wrist and resting hand splints: prevent wrist drop, maintain hand position for function
- Assistive devices: button hooks, key turners, dycem mats, universal cuffs
- Shoulder pain prevention: careful handling, correct sling if subluxation, avoid overhead ROM when rotator cuff weak
- Elbow extension splints overnight to prevent elbow flexion contractures
2.7 Fatigue Management
- Activity pacing: plan high-priority activities during peak energy times (typically morning)
- Energy conservation principles: seated techniques for ADLs, labor-saving devices
- Sleep quality: address nocturnal respiratory symptoms (refer for NIV if nocturnal hypoventilation)
- Aerobic conditioning (paradoxically reduces central fatigue in those who can tolerate it)
- Avoid post-exertional fatigue >30 minutes - reduce activity if this occurs
2.8 Pain Management
- Joint pain and stiffness: regular passive ROM, heat therapy
- Shoulder subluxation pain: sling, proper positioning, careful transfers
- Spasticity-related pain: stretching, splinting, baclofen
- Pressure-area pain: offloading, pressure mattress
- Cramps: gentle massage, warm baths, gentle stretching
- Refer to physiotherapist-led pain management if neuropathic pain suspected
2.9 Carer/Family Education and Training
- Manual handling techniques: safe transfers, hoisting, positioning
- Home ROM exercise program
- Use of assistive technology and mobility aids
- Airway clearance (manually assisted cough, cough assist device)
- NIV care and troubleshooting
- Recognizing respiratory deterioration - when to call for help
- Carer fatigue assessment and referral for respite care
- Home safety assessment
2.10 Telehealth and Home-Based Physiotherapy
- Telehealth-based exercise in ALS (PMID: 37564731, Front Neurol 2023): telehealth delivery of physiotherapy is feasible and acceptable in ALS, reducing travel burden for patients with limited mobility
- Particularly valuable in late-stage disease when travel to clinic is difficult
- Video-based exercise supervision, caregiver coaching, respiratory monitoring at home
Part 3: Stage-Based Summary
| ALS Stage | Primary Physio Goals | Key Interventions |
|---|---|---|
| Early | Maintain function, prevent deconditioning | Moderate aerobic + strengthening exercise, education, gait assessment, respiratory baseline |
| Middle | Maximise independence, prevent falls, respiratory support | AFO, walking aids, ROM exercises, airway clearance techniques, NIV planning, fatigue management |
| Late | Maintain comfort and dignity, prevent complications | Wheelchair, positioning, pressure care, cough assist/NIV, carer training |
| End-stage | Comfort, symptom control | Palliative positioning, secretion management, family support |
Key Outcome Measures for Physiotherapy in ALS
| Measure | What it Assesses |
|---|---|
| ALSFRS-R | Overall function (0-48) |
| MRC Sum Score | Global muscle strength |
| FVC (seated and supine) | Respiratory function |
| SNIP / MIP / MEP | Respiratory muscle strength |
| Peak Cough Flow (PCF) | Cough effectiveness |
| Fatigue Severity Scale (FSS) | Fatigue severity |
| Berg Balance Scale (BBS) | Balance |
| Timed Up and Go (TUG) | Mobility |
| 10-Metre Walk Test | Gait speed |
| Visual Analog Scale (VAS) | Pain |
| McGill Quality of Life Questionnaire | QoL |
Evidence Summary (2024-2026)
| Study | Finding |
|---|---|
| Li & Kang, Sci Rep 2024 (Network meta-analysis, 12 RCTs) | Exercise intervention had the greatest benefit on ALSFRS-R, FVC, QoL and MRC sum score among all non-pharmacological ALS interventions |
| Silva et al., BMJ Open 2024 (Systematic review) | Physiotherapy may improve short-term global function; no serious adverse events; evidence quality still low |
| Souza et al., PLoS One 2025 (Systematic review + meta-analysis) | Strengthening exercise is safe in ALS; no serious adverse events; inconclusive superiority vs. control due to small study sizes |
| Benzo-Iglesias et al., Ther Adv Respir Dis 2025 (Systematic review + meta-analysis, 5 RCTs) | Respiratory muscle training improves MIP and MEP; one study shows inspiratory training may predict survival |
| Gratzer et al., J Clin Med 2025 (Clinical review) | Evidence supports moderate tailored exercise, early respiratory therapy, spasticity and mobility management as key physiotherapy elements in ALS |
Create a structured physiotherapy intake form for ALS assessment
mkdir -p /home/daytona/workspace/als-intake-form && ls /home/daytona/workspace/a…
~/als-intake-form/generate_form.js
const {
Document, Packer, Paragraph, TextRun, Table, TableRow, TableCell,
AlignmentType, HeadingLevel, BorderStyle, WidthType, ShadingType,
VerticalAlign, PageNumber, Header, Footer, PageBreak,
UnderlineType
} = require('docx');
const fs = require('fs');
// ─── Helpers ────────────────────────────────────────────────────────────────
const TEAL = "1A7A8A";
const TEAL_LIGHT = "E6F4F6";
const GREY_LIGHT = "F5F5F5";
const WHITE = "FFFFFF";
const DARK = "1A1A2E";
const MID_GREY = "CCCCCC";
function sectionHeader(text) {
return new Paragraph({
heading: HeadingLevel.HEADING_1,
spacing: { before: 280, after: 100 },
shading: { type: ShadingType.SOLID, color: TEAL },
children: [
new TextRun({
text: text,
color: WHITE,
bold: true,
size: 24,
font: "Calibri",
}),
],
});
}
function subHeader(text) {
return new Paragraph({
spacing: { before: 200, after: 60 },
children: [
new TextRun({
text: text,
bold: true,
color: TEAL,
size: 22,
font: "Calibri",
underline: { type: UnderlineType.SINGLE, color: TEAL },
}),
],
});
}
function label(text) {
return new TextRun({ text, bold: true, size: 20, font: "Calibri", color: DARK });
}
function field(width = 3500) {
return new TextRun({ text: "_".repeat(Math.floor(width / 80)), size: 20, font: "Calibri", color: MID_GREY });
}
function labelLine(labelText, extraField = "") {
return new Paragraph({
spacing: { before: 80, after: 60 },
children: [
label(labelText + " "),
field(),
...(extraField ? [new TextRun({ text: " " }), label(extraField + " "), field()] : []),
],
});
}
function checkboxLine(labelText, options) {
const runs = [label(labelText + ": ")];
options.forEach((opt) => {
runs.push(new TextRun({ text: "\u25A1 " + opt + " ", size: 20, font: "Calibri" }));
});
return new Paragraph({ spacing: { before: 80, after: 60 }, children: runs });
}
function yesNoLine(labelText) {
return checkboxLine(labelText, ["Yes", "No"]);
}
function multiLine(labelText) {
return [
new Paragraph({
spacing: { before: 80, after: 20 },
children: [label(labelText)],
}),
new Paragraph({
spacing: { before: 0, after: 40 },
children: [new TextRun({ text: "_".repeat(120), size: 20, font: "Calibri", color: MID_GREY })],
}),
new Paragraph({
spacing: { before: 0, after: 60 },
children: [new TextRun({ text: "_".repeat(120), size: 20, font: "Calibri", color: MID_GREY })],
}),
];
}
function smallNote(text) {
return new Paragraph({
spacing: { before: 40, after: 40 },
children: [new TextRun({ text, size: 17, font: "Calibri", color: "888888", italics: true })],
});
}
function spacer() {
return new Paragraph({ spacing: { before: 60, after: 60 }, children: [new TextRun("")] });
}
// ─── Scoring Table ───────────────────────────────────────────────────────────
function scoreTable(title, rows) {
const headerRow = new TableRow({
tableHeader: true,
children: ["Domain", "Score", "Notes"].map((h) =>
new TableCell({
shading: { type: ShadingType.SOLID, color: TEAL },
children: [new Paragraph({
children: [new TextRun({ text: h, bold: true, color: WHITE, size: 20, font: "Calibri" })],
alignment: AlignmentType.CENTER,
})],
verticalAlign: VerticalAlign.CENTER,
})
),
});
const dataRows = rows.map((r, i) =>
new TableRow({
children: [
new TableCell({
shading: { type: ShadingType.SOLID, color: i % 2 === 0 ? GREY_LIGHT : WHITE },
width: { size: 40, type: WidthType.PERCENTAGE },
children: [new Paragraph({ children: [new TextRun({ text: r, size: 19, font: "Calibri" })] })],
}),
new TableCell({
shading: { type: ShadingType.SOLID, color: i % 2 === 0 ? GREY_LIGHT : WHITE },
width: { size: 20, type: WidthType.PERCENTAGE },
children: [new Paragraph({ children: [new TextRun({ text: "___/___", size: 19, font: "Calibri", color: MID_GREY })] })],
}),
new TableCell({
shading: { type: ShadingType.SOLID, color: i % 2 === 0 ? GREY_LIGHT : WHITE },
width: { size: 40, type: WidthType.PERCENTAGE },
children: [new Paragraph({ children: [new TextRun({ text: "________________________________", size: 19, font: "Calibri", color: MID_GREY })] })],
}),
],
})
);
return [
subHeader(title),
new Table({
width: { size: 100, type: WidthType.PERCENTAGE },
rows: [headerRow, ...dataRows],
}),
spacer(),
];
}
// ─── Two-column row helper ────────────────────────────────────────────────────
function twoColRow(left, right) {
return new Table({
width: { size: 100, type: WidthType.PERCENTAGE },
borders: {
top: { style: BorderStyle.NONE }, bottom: { style: BorderStyle.NONE },
left: { style: BorderStyle.NONE }, right: { style: BorderStyle.NONE },
insideH: { style: BorderStyle.NONE }, insideV: { style: BorderStyle.NONE },
},
rows: [
new TableRow({
children: [
new TableCell({ width: { size: 50, type: WidthType.PERCENTAGE }, children: [left] }),
new TableCell({ width: { size: 50, type: WidthType.PERCENTAGE }, children: [right] }),
],
}),
],
});
}
// ─── Muscle Strength Table ───────────────────────────────────────────────────
function muscleTable() {
const muscles = [
["Shoulder Abductors", "", ""],
["Elbow Flexors", "", ""],
["Elbow Extensors", "", ""],
["Wrist Extensors", "", ""],
["Finger Flexors", "", ""],
["Intrinsic Hand / Thenar", "", ""],
["Hip Flexors", "", ""],
["Knee Extensors", "", ""],
["Knee Flexors", "", ""],
["Ankle Dorsiflexors", "", ""],
["Ankle Plantar Flexors", "", ""],
["Neck Flexors", "", ""],
["Neck Extensors", "", ""],
];
const headerRow = new TableRow({
tableHeader: true,
children: ["Muscle Group", "R (MRC 0-5)", "L (MRC 0-5)", "Notes"].map((h) =>
new TableCell({
shading: { type: ShadingType.SOLID, color: TEAL },
children: [new Paragraph({
children: [new TextRun({ text: h, bold: true, color: WHITE, size: 19, font: "Calibri" })],
alignment: AlignmentType.CENTER,
})],
})
),
});
const dataRows = muscles.map((m, i) =>
new TableRow({
children: [
new TableCell({
shading: { type: ShadingType.SOLID, color: i % 2 === 0 ? GREY_LIGHT : WHITE },
width: { size: 40, type: WidthType.PERCENTAGE },
children: [new Paragraph({ children: [new TextRun({ text: m[0], size: 19, font: "Calibri" })] })],
}),
...["R", "L", "Notes"].map(() =>
new TableCell({
shading: { type: ShadingType.SOLID, color: i % 2 === 0 ? GREY_LIGHT : WHITE },
width: { size: 20, type: WidthType.PERCENTAGE },
children: [new Paragraph({ children: [new TextRun({ text: "________", size: 19, font: "Calibri", color: MID_GREY })] })],
})
),
],
})
);
return new Table({
width: { size: 100, type: WidthType.PERCENTAGE },
rows: [headerRow, ...dataRows],
});
}
// ─── ALSFRS-R Table ──────────────────────────────────────────────────────────
function alsfrTable() {
const items = [
"1. Speech",
"2. Salivation",
"3. Swallowing",
"4. Handwriting",
"5. Cutting Food / Utensils",
"6. Dressing / Hygiene",
"7. Turning in Bed",
"8. Walking",
"9. Climbing Stairs",
"10. Dyspnea",
"11. Orthopnea",
"12. Respiratory Insufficiency",
];
const headerRow = new TableRow({
tableHeader: true,
children: ["ALSFRS-R Item", "Score (0-4)", "Notes"].map((h) =>
new TableCell({
shading: { type: ShadingType.SOLID, color: TEAL },
children: [new Paragraph({
children: [new TextRun({ text: h, bold: true, color: WHITE, size: 19, font: "Calibri" })],
alignment: AlignmentType.CENTER,
})],
})
),
});
const dataRows = items.map((item, i) =>
new TableRow({
children: [
new TableCell({
shading: { type: ShadingType.SOLID, color: i % 2 === 0 ? GREY_LIGHT : WHITE },
width: { size: 50, type: WidthType.PERCENTAGE },
children: [new Paragraph({ children: [new TextRun({ text: item, size: 19, font: "Calibri" })] })],
}),
new TableCell({
shading: { type: ShadingType.SOLID, color: i % 2 === 0 ? GREY_LIGHT : WHITE },
width: { size: 15, type: WidthType.PERCENTAGE },
children: [new Paragraph({ alignment: AlignmentType.CENTER, children: [new TextRun({ text: "___/4", size: 19, font: "Calibri", color: MID_GREY })] })],
}),
new TableCell({
shading: { type: ShadingType.SOLID, color: i % 2 === 0 ? GREY_LIGHT : WHITE },
width: { size: 35, type: WidthType.PERCENTAGE },
children: [new Paragraph({ children: [new TextRun({ text: "________________________________", size: 19, font: "Calibri", color: MID_GREY })] })],
}),
],
})
);
const totalRow = new TableRow({
children: [
new TableCell({
shading: { type: ShadingType.SOLID, color: TEAL_LIGHT },
children: [new Paragraph({ children: [new TextRun({ text: "TOTAL SCORE", bold: true, size: 20, font: "Calibri" })] })],
}),
new TableCell({
shading: { type: ShadingType.SOLID, color: TEAL_LIGHT },
children: [new Paragraph({ alignment: AlignmentType.CENTER, children: [new TextRun({ text: "___/48", bold: true, size: 20, font: "Calibri", color: TEAL })] })],
}),
new TableCell({
shading: { type: ShadingType.SOLID, color: TEAL_LIGHT },
children: [new Paragraph({ children: [new TextRun({ text: "Rate of change: ___ pts/month", size: 19, font: "Calibri", italics: true })] })],
}),
],
});
return new Table({
width: { size: 100, type: WidthType.PERCENTAGE },
rows: [headerRow, ...dataRows, totalRow],
});
}
// ─── Respiratory Table ───────────────────────────────────────────────────────
function respiratoryTable() {
const params = [
["FVC Seated (%predicted)", "____%", "Normal >80%"],
["FVC Supine (%predicted)", "____%", "Drop >25% from seated = significant"],
["SNIP (cmH₂O)", "____", "<40 = significant impairment"],
["MIP (cmH₂O)", "____", "<60 = inspiratory muscle weakness"],
["MEP (cmH₂O)", "____", "<60 = impaired cough"],
["Peak Cough Flow (L/min)", "____", "<270 = retention risk; <160 = ineffective cough"],
["Oxygen Saturation (SpO₂)", "____%", ""],
["Respiratory Rate (/min)", "____", "Normal 12-20"],
["Nocturnal symptoms", "\u25A1 Yes \u25A1 No", "Headache / somnolence / orthopnea"],
];
const headerRow = new TableRow({
tableHeader: true,
children: ["Parameter", "Value", "Clinical Threshold"].map((h) =>
new TableCell({
shading: { type: ShadingType.SOLID, color: TEAL },
children: [new Paragraph({ children: [new TextRun({ text: h, bold: true, color: WHITE, size: 19, font: "Calibri" })] })],
})
),
});
const dataRows = params.map((p, i) =>
new TableRow({
children: p.map((cell) =>
new TableCell({
shading: { type: ShadingType.SOLID, color: i % 2 === 0 ? GREY_LIGHT : WHITE },
children: [new Paragraph({ children: [new TextRun({ text: cell, size: 19, font: "Calibri" })] })],
})
),
})
);
return new Table({ width: { size: 100, type: WidthType.PERCENTAGE }, rows: [headerRow, ...dataRows] });
}
// ─── Title Page ──────────────────────────────────────────────────────────────
function titleBlock() {
return [
new Paragraph({
alignment: AlignmentType.CENTER,
spacing: { before: 200, after: 60 },
shading: { type: ShadingType.SOLID, color: TEAL },
children: [
new TextRun({ text: " PHYSIOTHERAPY INTAKE & ASSESSMENT FORM", bold: true, size: 34, color: WHITE, font: "Calibri" }),
],
}),
new Paragraph({
alignment: AlignmentType.CENTER,
spacing: { before: 0, after: 40 },
shading: { type: ShadingType.SOLID, color: "155F6B" },
children: [
new TextRun({ text: " AMYOTROPHIC LATERAL SCLEROSIS (ALS / MND)", bold: true, size: 24, color: WHITE, font: "Calibri" }),
],
}),
new Paragraph({
alignment: AlignmentType.CENTER,
spacing: { before: 60, after: 160 },
children: [
new TextRun({ text: "Multidisciplinary ALS Clinic | Neurological Physiotherapy Department", size: 19, font: "Calibri", italics: true, color: "555555" }),
],
}),
];
}
// ─── Build Document ──────────────────────────────────────────────────────────
const children = [
// Title
...titleBlock(),
// ═══════════════════════════════════════════
// SECTION 1 – Patient Demographics
// ═══════════════════════════════════════════
sectionHeader("SECTION 1 — PATIENT DEMOGRAPHICS"),
spacer(),
labelLine("Patient Name:", "Date of Birth:"),
labelLine("MRN / Hospital No.:", "Date of Assessment:"),
labelLine("Referring Physician:", "Diagnosis Date:"),
labelLine("ALS Clinic / Centre:", "Therapist Name:"),
checkboxLine("ALS Type", ["Sporadic", "Familial"]),
checkboxLine("Onset Region", ["Spinal – Upper Limb", "Spinal – Lower Limb", "Bulbar", "Respiratory", "Unknown"]),
checkboxLine("Genetic Testing", ["Not done", "SOD1", "C9ORF72", "FUS/TLS", "TARDBP", "Other: ________"]),
labelLine("Emergency Contact Name:", "Relationship:"),
labelLine("Emergency Contact Phone:", ""),
spacer(),
// ═══════════════════════════════════════════
// SECTION 2 – Subjective History
// ═══════════════════════════════════════════
sectionHeader("SECTION 2 — SUBJECTIVE HISTORY"),
spacer(),
subHeader("2.1 Presenting Complaints"),
...multiLine("Chief complaint (in patient's own words):"),
labelLine("Date of first symptom:", "Body region first affected:"),
labelLine("Disease duration (months):", ""),
spacer(),
subHeader("2.2 Symptom Profile"),
checkboxLine("Current Symptoms", ["Weakness", "Fasciculations", "Muscle cramps", "Spasticity", "Fatigue"]),
checkboxLine("", ["Dysphagia", "Dysarthria", "Sialorrhea", "Dyspnea", "Orthopnea"]),
checkboxLine("", ["Foot drop", "Head drop", "Pain / joint stiffness", "Mood changes", "Sleep disturbance"]),
checkboxLine("Cognitive Changes", ["None", "Mild frontal", "Formal FTD diagnosis"]),
...multiLine("Other symptoms / notes:"),
spacer(),
subHeader("2.3 Functional History"),
checkboxLine("Mobility Status", ["Independently ambulant", "Ambulant with aid", "Wheelchair part-time", "Wheelchair full-time", "Bedbound"]),
checkboxLine("Walking Aid Used", ["None", "Walking stick", "Quad stick", "Rollator", "Forearm crutches", "Walker frame"]),
checkboxLine("Wheelchair", ["None", "Manual – self-propelled", "Manual – carer-propelled", "Powered – joystick", "Powered – alternative control"]),
labelLine("Approximate walking distance:", "Falls in past 3 months:"),
checkboxLine("ADL Independence", ["Fully independent", "Independent with aids", "Requires some assistance", "Fully dependent"]),
...multiLine("Activities most limited by ALS (patient-stated priorities):"),
spacer(),
subHeader("2.4 Fatigue Assessment"),
labelLine("Fatigue Severity Scale (FSS) Score:", "(threshold: >36 = significant fatigue)"),
checkboxLine("Post-exercise fatigue >30 minutes", ["Yes – reduce activity load", "No"]),
...multiLine("Fatigue pattern / triggers:"),
spacer(),
subHeader("2.5 Pain Assessment"),
yesNoLine("Current pain"),
labelLine("Pain location:", "NRS Score (0-10):"),
checkboxLine("Pain type", ["Spasticity-related", "Joint / mechanical", "Cramps", "Pressure area", "Neuropathic", "Other"]),
spacer(),
subHeader("2.6 Respiratory Symptoms"),
yesNoLine("Dyspnea on exertion"),
yesNoLine("Orthopnea (breathlessness when lying flat)"),
yesNoLine("Morning headaches"),
yesNoLine("Excessive daytime sleepiness"),
yesNoLine("Interrupted / poor-quality sleep"),
yesNoLine("Currently on NIV / BiPAP"),
labelLine("If on NIV – hours/night:", "Interface type:"),
spacer(),
subHeader("2.7 Social and Home Environment"),
checkboxLine("Living Situation", ["Alone", "With spouse/partner", "With family", "Supported accommodation", "Residential care"]),
checkboxLine("Home Type", ["Single storey", "Multi-storey – lift", "Multi-storey – stairs only", "Other"]),
yesNoLine("Home modifications in place (grab rails, ramp, stairlift, hospital bed)"),
labelLine("Primary carer:", "Carer availability (hrs/day):"),
yesNoLine("Carer trained in manual handling"),
checkboxLine("Employment Status", ["Working full-time", "Working part-time", "Reduced duties", "Unable to work", "Retired"]),
spacer(),
subHeader("2.8 Medical History & Medications"),
...multiLine("Relevant past medical history:"),
labelLine("Current medications relevant to PT:", ""),
checkboxLine("Disease-modifying therapy", ["Riluzole", "Edaravone", "Tofersen", "AMX0035", "None", "Clinical trial"]),
checkboxLine("Medications affecting PT", ["Baclofen", "Tizanidine", "Opioids", "Benzodiazepines", "None"]),
spacer(),
subHeader("2.9 Patient Goals"),
...multiLine("Short-term goals (1-3 months):"),
...multiLine("Long-term goals (3-12 months):"),
...multiLine("Priority activities to maintain:"),
spacer(),
// ═══════════════════════════════════════════
// SECTION 3 – Objective Assessment
// ═══════════════════════════════════════════
new Paragraph({ children: [new PageBreak()] }),
sectionHeader("SECTION 3 — OBJECTIVE ASSESSMENT"),
spacer(),
subHeader("3.1 General Observations"),
...multiLine("Posture, affect, nutritional status, communication, resting respiratory pattern:"),
spacer(),
subHeader("3.2 ALS Functional Rating Scale – Revised (ALSFRS-R)"),
smallNote("Score each item 0 (unable) to 4 (normal). Total score /48. Rate of decline >1 pt/month = faster progression."),
spacer(),
alsfrTable(),
spacer(),
// ═══════════════════════════════════════════
// SECTION 4 – Muscle Strength
// ═══════════════════════════════════════════
sectionHeader("SECTION 4 — MUSCLE STRENGTH (MRC SCALE)"),
smallNote("MRC Grade: 0 = No contraction | 1 = Flicker | 2 = Movement with gravity eliminated | 3 = Movement against gravity | 4 = Movement against resistance | 5 = Normal"),
spacer(),
muscleTable(),
spacer(),
labelLine("Grip Strength R (kg):", "Grip Strength L (kg):"),
labelLine("Pinch Strength R:", "Pinch Strength L:"),
...multiLine("Notes on asymmetry, fatigue, pattern of weakness:"),
spacer(),
// ═══════════════════════════════════════════
// SECTION 5 – Tone & Spasticity
// ═══════════════════════════════════════════
sectionHeader("SECTION 5 — TONE & SPASTICITY"),
spacer(),
checkboxLine("UMN Signs Present", ["Hyperreflexia", "Clonus", "Babinski sign", "Hoffman sign", "Spasticity"]),
checkboxLine("LMN Signs Present", ["Hyporeflexia/areflexia", "Fasciculations", "Muscle wasting"]),
...scoreTable("Modified Ashworth Scale (MAS)", [
"Shoulder / Elbow (R)",
"Shoulder / Elbow (L)",
"Wrist / Finger flexors (R)",
"Wrist / Finger flexors (L)",
"Hip flexors / Adductors (R)",
"Hip flexors / Adductors (L)",
"Ankle plantar flexors (R)",
"Ankle plantar flexors (L)",
]),
...multiLine("Functional impact of spasticity:"),
spacer(),
// ═══════════════════════════════════════════
// SECTION 6 – Range of Motion
// ═══════════════════════════════════════════
sectionHeader("SECTION 6 — RANGE OF MOTION"),
spacer(),
labelLine("Shoulder Flexion R:", "L:"),
labelLine("Shoulder Abduction R:", "L:"),
labelLine("Elbow Extension R:", "L:"),
labelLine("Wrist Extension R:", "L:"),
labelLine("Finger Extension R:", "L:"),
labelLine("Hip Extension R:", "L:"),
labelLine("Knee Extension R:", "L:"),
labelLine("Ankle Dorsiflexion R:", "L:"),
checkboxLine("Contractures Present", ["None", "Shoulder", "Elbow", "Wrist", "Finger", "Hip", "Knee", "Ankle"]),
...multiLine("Notes:"),
spacer(),
// ═══════════════════════════════════════════
// SECTION 7 – Respiratory Assessment
// ═══════════════════════════════════════════
new Paragraph({ children: [new PageBreak()] }),
sectionHeader("SECTION 7 — RESPIRATORY ASSESSMENT"),
spacer(),
respiratoryTable(),
spacer(),
checkboxLine("Paradoxical breathing (abdominal wall movement)", ["Present", "Absent"]),
checkboxLine("Cough effectiveness", ["Effective", "Weak but functional", "Ineffective – cough assist needed"]),
checkboxLine("Secretion management", ["Independent", "Requires airway clearance", "Cough assist device in use"]),
checkboxLine("NIV / BiPAP Recommendation", ["Not yet indicated", "Discuss / plan for initiation", "Initiate – FVC <50% / symptomatic", "Already established"]),
...multiLine("Respiratory notes / plan:"),
spacer(),
// ═══════════════════════════════════════════
// SECTION 8 – Functional Mobility & Balance
// ═══════════════════════════════════════════
sectionHeader("SECTION 8 — FUNCTIONAL MOBILITY & BALANCE"),
spacer(),
...scoreTable("Functional Outcome Measures", [
"Timed Up and Go (TUG) – seconds",
"10-Metre Walk Test – seconds / speed (m/s)",
"6-Minute Walk Test – metres (if safe)",
"Berg Balance Scale (BBS) – /56",
"Sit-to-Stand (5 times) – seconds",
]),
checkboxLine("Gait Deviations", ["Foot drop / steppage gait", "Trendelenburg (hip abductor weakness)", "Head drop affecting balance", "Trunk instability", "Reduced arm swing", "None"]),
checkboxLine("Falls Risk", ["Low (BBS >45)", "Moderate (BBS 36-45)", "High (BBS <36)"]),
...multiLine("Fall history details / near-misses:"),
spacer(),
// ═══════════════════════════════════════════
// SECTION 9 – Posture & Pressure Care
// ═══════════════════════════════════════════
sectionHeader("SECTION 9 — POSTURE & PRESSURE CARE"),
spacer(),
checkboxLine("Head Drop", ["Absent", "Mild", "Moderate – collar considered", "Severe – collar required"]),
checkboxLine("Trunk Control", ["Good", "Mildly impaired", "Significantly impaired – supports required"]),
checkboxLine("Pressure Areas", ["Intact", "Red areas – at risk", "Grade 1 pressure injury", "Grade 2+", "Refer to tissue viability"]),
checkboxLine("Seating", ["Standard chair adequate", "Adapted seating", "Tilt-in-space wheelchair", "Custom moulded seating"]),
checkboxLine("Mattress", ["Standard", "Pressure-relieving foam", "Dynamic air mattress"]),
...multiLine("Postural management plan:"),
spacer(),
// ═══════════════════════════════════════════
// SECTION 10 – Staging
// ═══════════════════════════════════════════
sectionHeader("SECTION 10 — ALS STAGING (KING'S CLINICAL STAGING)"),
spacer(),
checkboxLine("Current Stage", [
"Stage 1 – Ambulant, minor deficits",
"Stage 2a – Independent, some functional limitation",
"Stage 2b – Dependent for some ADLs",
"Stage 3 – Wheelchair, reduced upper limb",
"Stage 4 – Dependent most ADLs",
"Stage 5 – End-stage / palliative",
]),
labelLine("ALSFRS-R decline rate (pts/month):", "King's stage at last visit:"),
spacer(),
// ═══════════════════════════════════════════
// SECTION 11 – Problem List
// ═══════════════════════════════════════════
new Paragraph({ children: [new PageBreak()] }),
sectionHeader("SECTION 11 — PHYSIOTHERAPY PROBLEM LIST"),
spacer(),
...["1.", "2.", "3.", "4.", "5.", "6."].flatMap((n) => [
new Paragraph({
spacing: { before: 60, after: 80 },
children: [
new TextRun({ text: n + " ", bold: true, size: 20, font: "Calibri", color: TEAL }),
new TextRun({ text: "_".repeat(110), size: 20, font: "Calibri", color: MID_GREY }),
],
}),
]),
spacer(),
// ═══════════════════════════════════════════
// SECTION 12 – Physiotherapy Goals
// ═══════════════════════════════════════════
sectionHeader("SECTION 12 — PHYSIOTHERAPY GOALS (SMART)"),
spacer(),
subHeader("Short-Term Goals (1-3 months)"),
...["1.", "2.", "3."].flatMap((n) => [
new Paragraph({
spacing: { before: 60, after: 80 },
children: [
new TextRun({ text: n + " ", bold: true, size: 20, font: "Calibri", color: TEAL }),
new TextRun({ text: "_".repeat(110), size: 20, font: "Calibri", color: MID_GREY }),
],
}),
]),
spacer(),
subHeader("Long-Term Goals (3-12 months)"),
...["1.", "2.", "3."].flatMap((n) => [
new Paragraph({
spacing: { before: 60, after: 80 },
children: [
new TextRun({ text: n + " ", bold: true, size: 20, font: "Calibri", color: TEAL }),
new TextRun({ text: "_".repeat(110), size: 20, font: "Calibri", color: MID_GREY }),
],
}),
]),
spacer(),
// ═══════════════════════════════════════════
// SECTION 13 – Intervention Plan
// ═══════════════════════════════════════════
sectionHeader("SECTION 13 — PHYSIOTHERAPY INTERVENTION PLAN"),
spacer(),
subHeader("13.1 Exercise Program"),
checkboxLine("Aerobic Exercise", ["Stationary cycling", "Walking program", "Hydrotherapy", "Arm ergometer", "None currently"]),
checkboxLine("Strengthening", ["Moderate resistance – preserved muscles", "Functional strengthening", "None – too weak / fatigued"]),
checkboxLine("Flexibility / Stretching", ["Active stretching", "Active-assisted ROM", "Passive ROM", "Carer-assisted home program"]),
labelLine("Exercise frequency (days/week):", "Session duration (mins):"),
smallNote("Safety rule: post-exercise fatigue must resolve within 30 minutes. Reduce load if this is exceeded."),
spacer(),
subHeader("13.2 Respiratory Physiotherapy"),
checkboxLine("Interventions Planned", ["Inspiratory Muscle Training (IMT)", "Expiratory Muscle Training (EMT)", "Manually Assisted Cough (MAC)"]),
checkboxLine("", ["Mechanical Insufflation-Exsufflation (Cough Assist)", "Air stacking / LVR", "HFCWO vest therapy"]),
checkboxLine("", ["NIV education and mask fitting", "Breathing pattern retraining", "Carer education in airway clearance"]),
spacer(),
subHeader("13.3 Mobility & Orthotics"),
checkboxLine("Orthotics / Aids", ["Ankle-foot orthosis (AFO) – R/L", "Cervical collar / head support", "Wrist splint", "Resting hand splint"]),
checkboxLine("", ["Walking stick", "Rollator", "Forearm crutches", "Manual wheelchair", "Powered wheelchair"]),
checkboxLine("", ["Stair rail installation advised", "Home modifications referral (OT)", "Ceiling hoist referral"]),
spacer(),
subHeader("13.4 Spasticity Management"),
checkboxLine("Physiotherapy Approach", ["Slow sustained stretching", "Positioning program", "Cryotherapy", "Hydrotherapy", "Splinting"]),
checkboxLine("Referral for", ["Botulinum toxin (focal spasticity)", "Intrathecal baclofen review", "None"]),
spacer(),
subHeader("13.5 Fatigue & Pain Management"),
checkboxLine("Fatigue Strategies", ["Activity pacing", "Energy conservation education", "Prioritisation of high-energy tasks to morning", "Sleep hygiene"]),
checkboxLine("Pain Management", ["Heat therapy", "TENS", "Joint ROM for stiffness", "Positioning / offloading", "Referral to pain team"]),
spacer(),
subHeader("13.6 Carer / Family Education"),
checkboxLine("Education Provided On", ["Safe manual handling", "Passive ROM home program", "Cough assist technique", "NIV use and care", "Pressure area prevention"]),
checkboxLine("", ["Fall prevention", "Adaptive equipment use", "Signs of respiratory deterioration", "Caregiver self-care / respite resources"]),
spacer(),
subHeader("13.7 Telehealth / Home Program"),
yesNoLine("Telehealth appropriate for this patient"),
yesNoLine("Written home exercise program provided"),
labelLine("Home program frequency:", "Review via telehealth:"),
spacer(),
// ═══════════════════════════════════════════
// SECTION 14 – MDT Referrals
// ═══════════════════════════════════════════
sectionHeader("SECTION 14 — MDT REFERRALS & COORDINATION"),
spacer(),
checkboxLine("Referrals Made", ["Occupational Therapy", "Speech & Language Therapy", "Dietitian / Nutritionist", "Respiratory Physician"]),
checkboxLine("", ["Palliative Care", "Psychology / Psychiatry", "Social Work", "Orthotics", "Community / Home PT"]),
...multiLine("Referral notes / reason:"),
spacer(),
// ═══════════════════════════════════════════
// SECTION 15 – Follow-Up Plan
// ═══════════════════════════════════════════
sectionHeader("SECTION 15 — FOLLOW-UP & REVIEW PLAN"),
spacer(),
checkboxLine("Follow-up Frequency", ["Every 2 weeks", "Monthly", "Every 2 months", "Every 3 months", "As needed"]),
labelLine("Next review date:", "Next ALSFRS-R to be completed:"),
labelLine("Next respiratory function test:", "Planned reassessment of goals:"),
...multiLine("Additional notes / special considerations:"),
spacer(),
// ═══════════════════════════════════════════
// SECTION 16 – Signature
// ═══════════════════════════════════════════
sectionHeader("SECTION 16 — CLINICIAN SIGN-OFF"),
spacer(),
labelLine("Physiotherapist Name (Print):", "Designation:"),
labelLine("Signature:", "Date:"),
labelLine("Countersigned (if applicable):", "Date:"),
smallNote("This form is a clinical record. Handle in accordance with patient data protection and confidentiality guidelines."),
spacer(),
];
// ─── Assemble Document ───────────────────────────────────────────────────────
const doc = new Document({
creator: "ALS Physiotherapy Clinic",
title: "ALS Physiotherapy Intake & Assessment Form",
description: "Structured physiotherapy intake and assessment form for patients with Amyotrophic Lateral Sclerosis",
styles: {
default: {
document: {
run: { font: "Calibri", size: 20 },
},
},
},
sections: [
{
properties: {
page: {
margin: { top: 720, bottom: 720, left: 900, right: 900 },
},
},
headers: {
default: new Header({
children: [
new Paragraph({
alignment: AlignmentType.RIGHT,
spacing: { after: 0 },
children: [
new TextRun({ text: "ALS Physiotherapy Intake Form | Page ", size: 17, font: "Calibri", color: "888888" }),
new TextRun({ children: [PageNumber.CURRENT], size: 17, font: "Calibri", color: "888888" }),
new TextRun({ text: " of ", size: 17, font: "Calibri", color: "888888" }),
new TextRun({ children: [PageNumber.TOTAL_PAGES], size: 17, font: "Calibri", color: "888888" }),
],
}),
],
}),
},
footers: {
default: new Footer({
children: [
new Paragraph({
alignment: AlignmentType.CENTER,
children: [
new TextRun({
text: "CONFIDENTIAL – Clinical Record | ALS / Motor Neuron Disease Service",
size: 16, font: "Calibri", color: "888888", italics: true,
}),
],
}),
],
}),
},
children,
},
],
});
Packer.toBuffer(doc).then((buffer) => {
fs.writeFileSync("/home/daytona/workspace/als-intake-form/ALS_Physiotherapy_Intake_Form.docx", buffer);
console.log("SUCCESS: Form generated at /home/daytona/workspace/als-intake-form/ALS_Physiotherapy_Intake_Form.docx");
});
cd /home/daytona/workspace/als-intake-form && node generate_form.js
python /home/daytona/skills/docx/scripts/office/validate.py /home/daytona/worksp…
python -c " import zipfile, os path = '/home/daytona/workspace/als-intake-form/A…
ALS Physiotherapy Intake Form
Word Document · DOCX
What's Included - 16 Sections
| # | Section | Contents |
|---|---|---|
| 1 | Patient Demographics | Name, MRN, DOB, ALS type, onset region, genetic subtype |
| 2 | Subjective History | Presenting complaints, symptom profile, fatigue (FSS), pain (NRS), respiratory symptoms, social/home environment, medications, patient goals |
| 3 | Objective Assessment | General observations + full ALSFRS-R table (12 items, /48) with rate-of-decline field |
| 4 | Muscle Strength | Full MRC table for 13 bilateral muscle groups + grip/pinch dynamometry |
| 5 | Tone & Spasticity | UMN/LMN sign checklist + Modified Ashworth Scale table (8 regions bilaterally) |
| 6 | Range of Motion | 8 joint measurements bilaterally + contracture checklist |
| 7 | Respiratory Assessment | Full respiratory table - FVC seated/supine, SNIP, MIP, MEP, PCF with clinical thresholds annotated; NIV recommendation |
| 8 | Functional Mobility & Balance | TUG, 10MWT, 6MWT, Berg Balance Scale, 5xSTS; gait deviation checklist; falls risk stratification |
| 9 | Posture & Pressure Care | Head drop, trunk control, pressure areas, seating, mattress |
| 10 | ALS Staging | King's Clinical Staging (Stages 1-5) with ALSFRS-R decline rate |
| 11 | Problem List | 6 numbered free-text problem entries |
| 12 | SMART Goals | Short-term (1-3 months) and long-term (3-12 months) goal boxes |
| 13 | Intervention Plan | Exercise, respiratory physiotherapy, mobility/orthotics, spasticity, fatigue/pain, carer education, telehealth |
| 14 | MDT Referrals | OT, SLT, Dietitian, Respiratory, Palliative, Psychology, Social Work |
| 15 | Follow-up Plan | Frequency, next review dates, reassessment schedule |
| 16 | Clinician Sign-Off | Signature, designation, countersign, confidentiality notice |