anatomy of abdominal incisions
Reading File
Finding Sources
Searching Images
abdominal incisions anatomy types
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
I now have comprehensive information from Schwartz's Principles of Surgery. Let me compile a thorough answer.
Anatomy of Abdominal Incisions
Abdominal Wall Anatomy (the foundation)
Before choosing or understanding any incision, you need to know what layers you are cutting through.
Layers (superficial → deep)
| Layer | Notes |
|---|---|
| Skin | |
| Subcutaneous tissue | Superficial fatty layer (Camper's fascia) + deep membranous layer (Scarpa's fascia) |
| External oblique muscle/aponeurosis | Fibers run medial and caudal; arises from the 8th rib |
| Internal oblique muscle/aponeurosis | Fibers run cranially and anteriorly; from thoracolumbar fascia |
| Transversus abdominis muscle/aponeurosis | Horizontal fibers; from costal margin and lumbar fascia |
| Transversalis fascia | Weak fibrous layer; posterior to rectus below arcuate line |
| Extraperitoneal (preperitoneal) fat | |
| Parietal peritoneum |
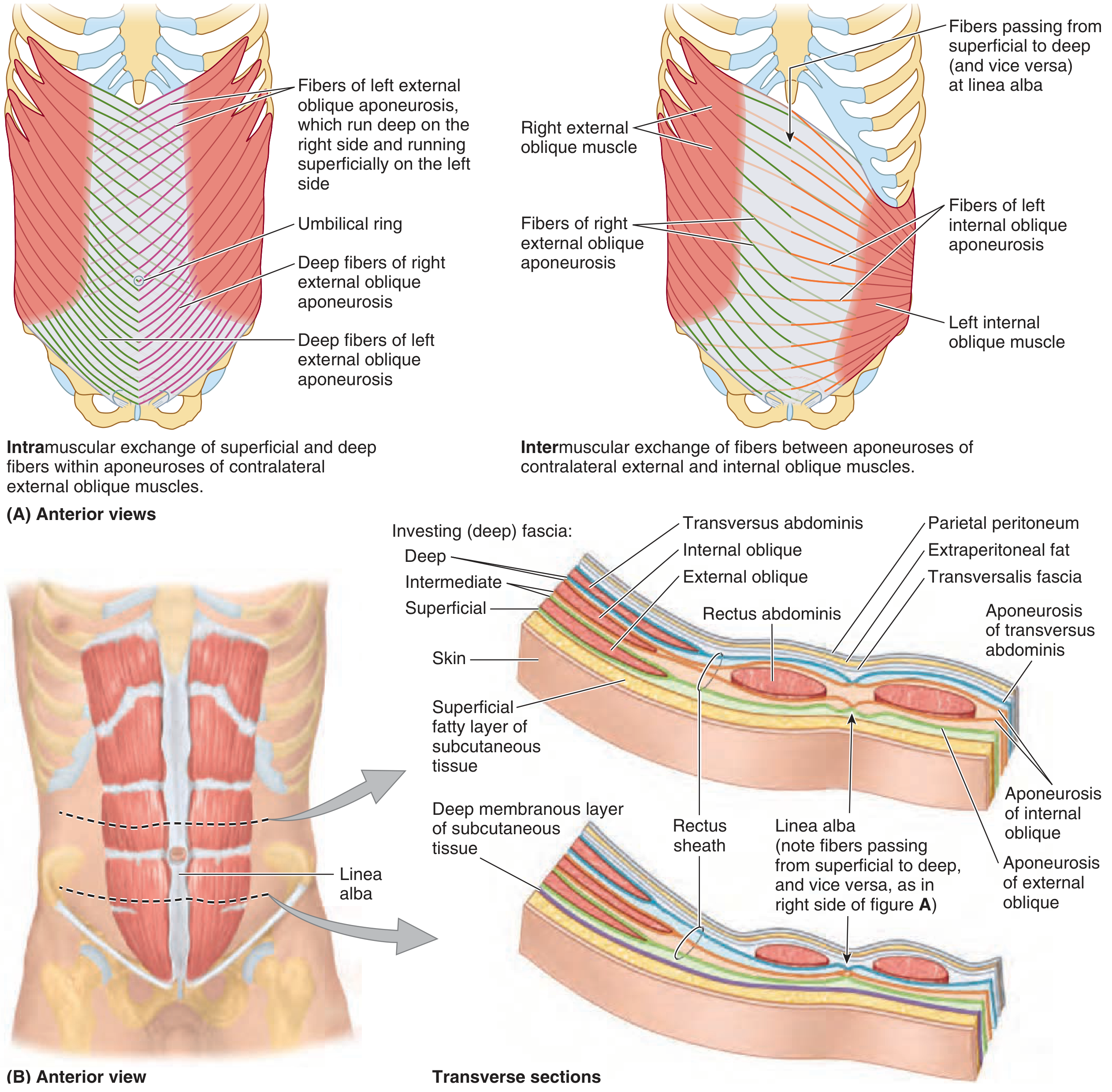
The Rectus Sheath and Arcuate Line
The three lateral muscle aponeuroses fuse in the midline as the linea alba and form the rectus sheath around the rectus abdominis.
- Above the arcuate line: Anterior sheath = external oblique + anterior leaf of internal oblique. Posterior sheath = posterior leaf of internal oblique + transversus abdominis aponeurosis.
- Below the arcuate line: All three aponeurotic layers shift anteriorly, so the posterior sheath is absent — only transversalis fascia covers the rectus posteriorly.
This is surgically relevant: incisions below the arcuate line provide no posterior fascial strength.
Neurovascular Anatomy
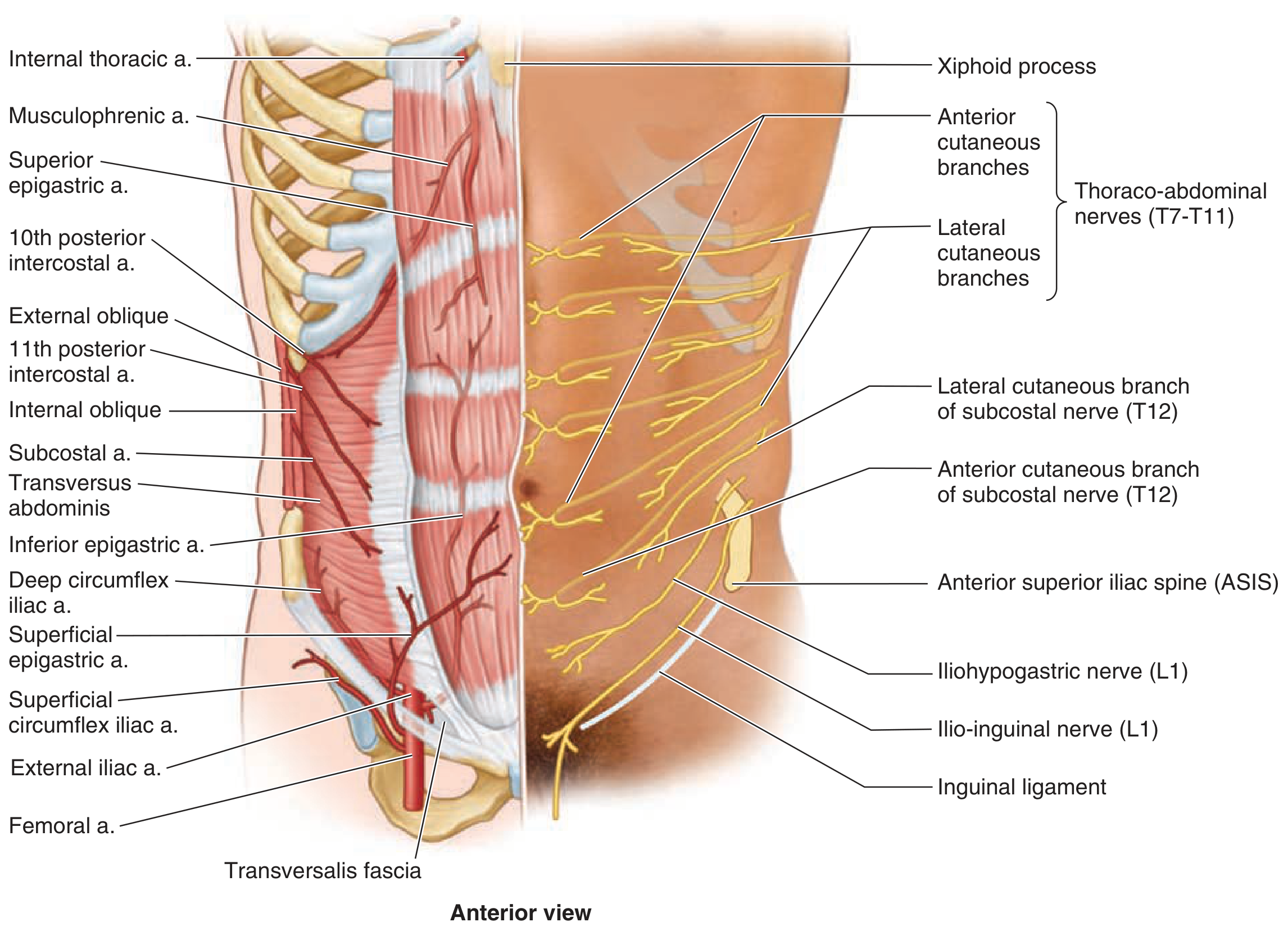
Arteries (deep):
- Superior epigastric artery — terminal branch of the internal thoracic; enters rectus sheath below the costal margin, travels on the posterior surface of the rectus
- Inferior epigastric artery — arises from the external iliac; these two vessels anastomose at the level of the umbilicus
- Also supplied by subcostal and lumbar arteries; superficial supply from superficial epigastric, superficial circumflex iliac, and superficial external pudendal arteries
Nerves:
- Sensory innervation: afferent branches of T4–L1 (dermatomal pattern)
- Motor innervation: efferent branches of T6–T12 to the abdominal wall muscles
- Lower incisions risk the iliohypogastric (L1) and ilio-inguinal (L1) nerves
Types of Abdominal Incisions
There are two general categories: longitudinal and transverse/oblique. Neither is clearly superior in overall outcomes — the choice is guided by the target organ and surgeon preference. Transverse incisions may have lower incisional hernia rates but higher wound infection rates.
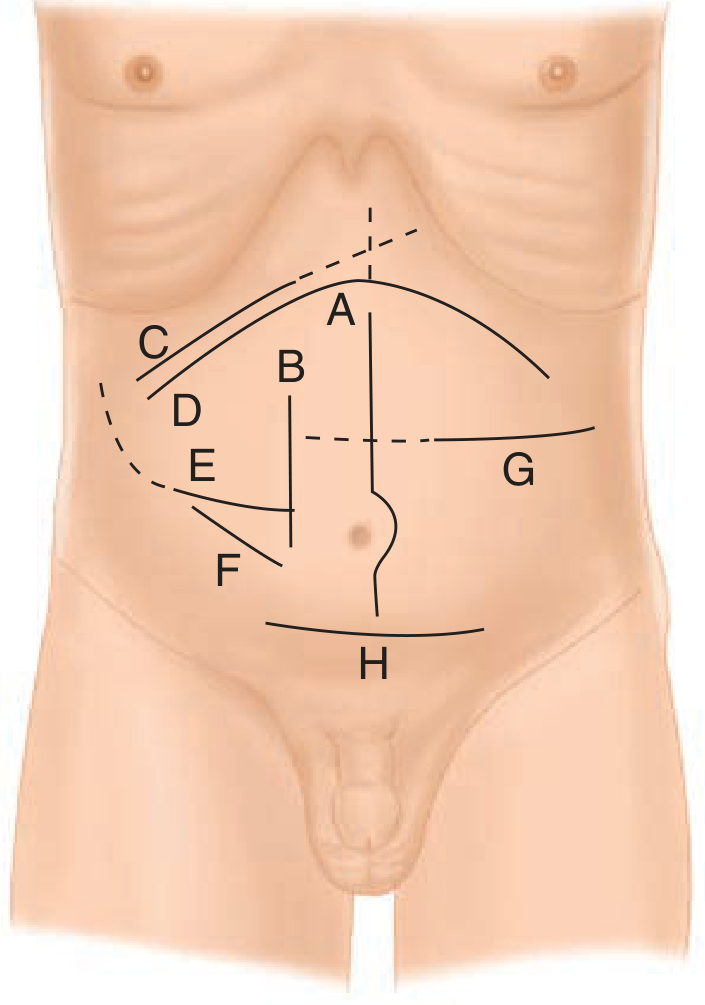
1. Midline Incision
- Direction: Longitudinal through the linea alba
- Access: Most intraabdominal organs and some retroperitoneal structures
- Advantages: Minimal injury to muscles, nerves, and vessels (the linea alba is avascular); rapid entry; extensile
- Closure: Requires reapproximation of the linea alba without undue tension; sutures placed at 5–8 mm intervals with 5 mm width shown to reduce incisional hernia rates
2. Paramedian Incision
- Direction: Longitudinal, lateral to the midline through the rectus sheath (medial paramedian) or in the pararectus location
- Limitation: Restricts access to the contralateral abdomen and pelvis; risks damage to musculature, vessels, and nerves supplying the rectus
3. Subcostal Incision (Kocher)
- Direction: Oblique, parallel and ~2–3 cm below the costal margin
- Right subcostal: Classic approach for cholecystectomy and right liver resections
- Bilateral subcostal (Chevron): Used for liver transplantation and bilateral adrenalectomy; can be extended with a midline ("Mercedes Benz") extension
4. Transverse Incision
- Direction: Horizontal across the abdomen
- Crosses the rectus muscles and oblique muscles
- Advantages over midline: may reduce hernia; incision follows Langer's lines → better cosmesis
5. McBurney / Rocky-Davis Incision
- McBurney: Oblique muscle-splitting incision in the right iliac fossa; centered over McBurney's point (1/3 of the way from ASIS to umbilicus)
- Rocky-Davis: Transverse version at the same location
- Weir extension: lateral extension of the Rocky-Davis for more exposure
- Used for: open appendectomy
6. Pfannenstiel Incision
- Direction: Transverse semilunar, two fingerbreadths above the pubic bone
- Layers divided: Skin → anterior rectus sheath (opened transversely) → linea alba taken down superiorly and inferiorly → rectus muscles bluntly separated from sheath → midline opened into the extraperitoneal space (Space of Retzius) or peritoneum
- Used for: Caesarean section, radical retropubic prostatectomy, pelvic lymphadenectomy, specimen extraction post-nephrectomy
- Closure: Peritoneum and muscle reapproximated; fascia closed with running or figure-of-eight absorbable suture
- Advantages: Low incisional hernia rates; can be extended into a Gibson incision
7. Gibson Incision
- Direction: Oblique/curvilinear, from a few cm medial to the ASIS extending down toward the inguinal fold, terminating lateral to the rectus or continuing to above the pubic symphysis
- A J-shaped ("hockey-stick") modification exists, though some data suggest higher hernia rates
- Layers: External oblique → internal oblique → transversus abdominis split in the same fashion; peritoneum mobilized medially for an extraperitoneal approach
- Used for: Renal transplantation, transplant nephrectomy, access to pelvic vessels, lower ureter, and bladder
- Closure: Two layers with running absorbable sutures
Complications of Abdominal Incisions
| Complication | Notes |
|---|---|
| Hematoma / seroma | Especially with large flaps |
| Surgical site infection | Higher with transverse incisions |
| Fascial dehiscence | Related to suture technique, tension |
| Incisional hernia | Most common long-term complication; higher with midline |
| Nerve injury | Risk varies by incision location — lower incisions risk iliohypogastric and ilio-inguinal nerves |
Sources: Schwartz's Principles of Surgery, 11e (Ch. 35); Campbell-Walsh-Wein Urology (Ch. 9)
steps of total thyroidectomy
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
You've run out of free credits. Sign up for a free account to continue using Orris.
This is a shared conversation. Sign in to Orris to start your own chat.