Iron deficiency anemia according to to Robbins
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the content needed to compose a comprehensive answer from both Robbins textbooks. Here is the full answer:
Iron Deficiency Anemia - Robbins
Sources: Robbins & Kumar Basic Pathology (9780323790185) and Robbins, Cotran & Kumar Pathologic Basis of Disease (9780443264528)
Overview
Iron deficiency is the most common nutritional deficiency in the world, and the most common cause of anemia globally. About 10% of people in higher-resource countries and 25-50% of those in lower-resource countries are anemic, with iron deficiency being the most frequent cause. It is especially prevalent in toddlers, adolescent girls, and females of childbearing age.
Iron Metabolism
Understanding iron deficiency begins with normal iron metabolism.
Body iron distribution (healthy young adults):
| Pool | Males (mg) | Females (mg) |
|---|---|---|
| Total | 3450 | 2450 |
| Hemoglobin | 2100 | 1750 |
| Myoglobin | 300 | 250 |
| Enzymes | 50 | 50 |
| Storage (ferritin/hemosiderin) | 1000 | 400 |
- ~80% of body iron is functional (hemoglobin, myoglobin, iron-containing enzymes like catalase and cytochromes)
- ~15-20% is storage iron as ferritin and hemosiderin, found in macrophages of the liver, spleen, and bone marrow
- Iron is transported in plasma bound to transferrin (normally ~33% saturated); serum iron averages 120 μg/dL in males, 100 μg/dL in females; total iron-binding capacity (TIBC) is normally 300-350 μg/dL
Storage forms:
- Ferritin - protein-iron complex in hepatocytes and macrophages; serum ferritin correlates with body iron stores. In iron deficiency: serum ferritin <12 μg/L; in iron overload: up to 5000 μg/L
- Hemosiderin - aggregated, partially degraded ferritin; turns blue-black with potassium ferrocyanide (Prussian blue stain)
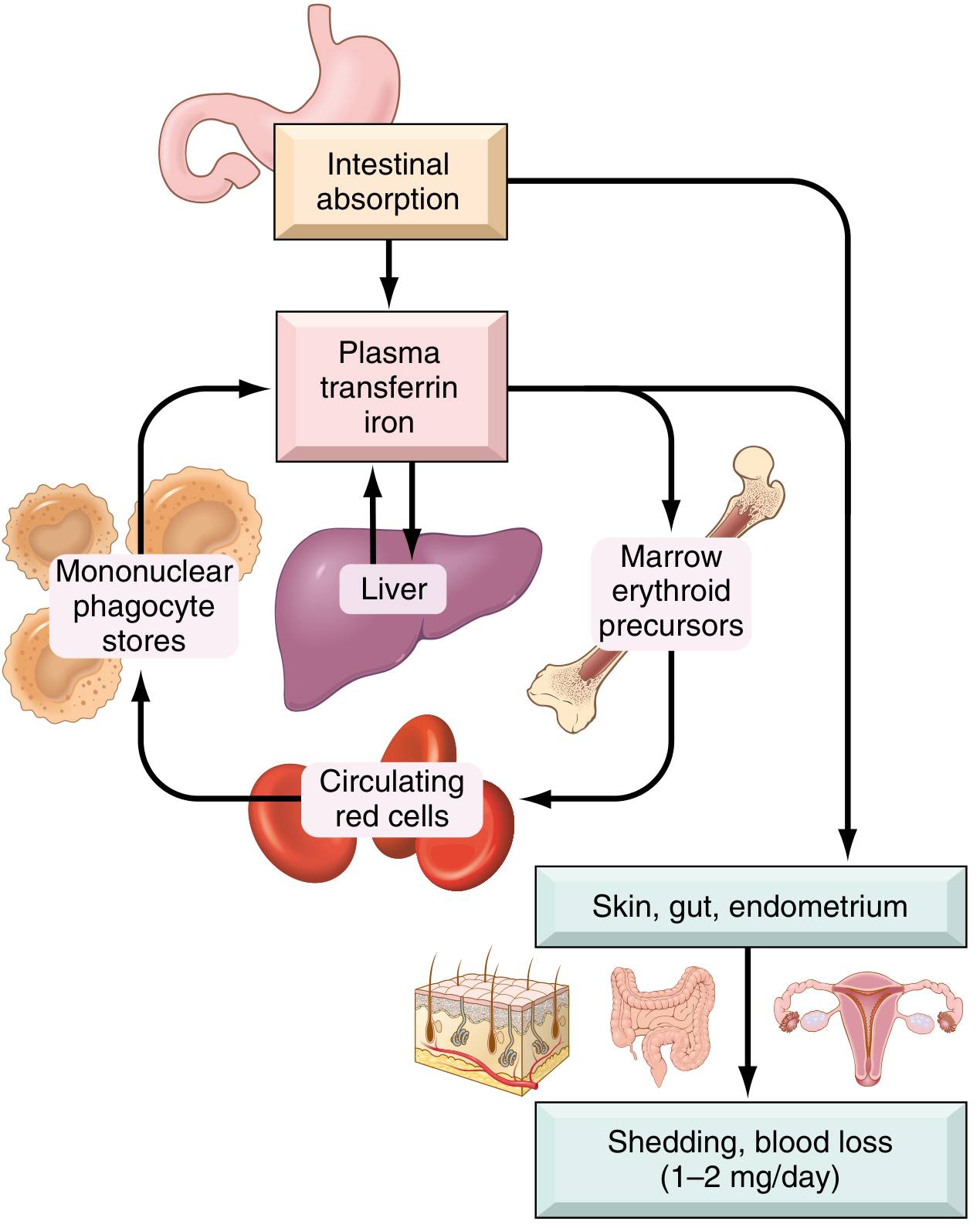
Absorption regulation:
- Dietary iron is absorbed in the proximal duodenum
- Nonheme iron (Fe³⁺) is reduced to Fe²⁺ by ferrireductases (duodenal cytochrome B), then transported across the apical membrane by DMT1 (divalent metal transporter-1)
- Heme iron crosses via separate transporters with much higher bioavailability (~20% vs 1-2% for nonheme)
- Fe²⁺ exits enterocytes across the basolateral membrane via ferroportin, then is oxidized to Fe³⁺ by hephaestin and ceruloplasmin to bind transferrin
- Hepcidin (synthesized by the liver) is the master regulator - it binds ferroportin, causing its degradation, thereby trapping iron in enterocytes and macrophages. High iron stores → high hepcidin → decreased absorption. Low iron stores → low hepcidin → increased absorption
- Inflammatory mediators (e.g., IL-6) upregulate hepcidin; erythroferrone (from erythroblasts) suppresses hepcidin to enhance iron supply during erythropoiesis
Daily balance: Iron is lost at 1-2 mg/day (shedding of mucosal and skin epithelial cells). Normal Western diet contains 10-20 mg/day; ~20% of heme iron and only 1-2% of nonheme iron is absorbable.
Etiology and Pathogenesis
Iron deficiency arises from four main mechanisms:
1. Dietary Lack
- Rare in high-resource countries (two-thirds of dietary iron is heme iron from meat)
- Common in low-resource countries where most dietary iron is nonheme (vegetables)
- At-risk groups: infants (breast milk has only ~0.3 mg/L iron; cow's milk iron is poorly bioavailable), vegans, the elderly (restricted diets), and the impoverished
- In the US: seen in infants fed exclusively milk, those with food insecurity, and the elderly
- Bioavailability is enhanced by: ascorbic acid, citric acid, amino acids, sugars
- Bioavailability is reduced by: tannins (tea), carbonates, oxalates, phosphates
2. Impaired Absorption
- Celiac disease, other causes of fat malabsorption (steatorrhea), chronic diarrhea
- Gastrectomy (reduces duodenal acidity and transit time)
- Various forms of gastritis
3. Increased Demand
- Infancy, childhood, adolescence (rapid growth)
- Pregnancy - a major cause worldwide
- Premenopausal females; females in low-resource countries with multiple closely spaced pregnancies are at exceptionally high risk
4. Chronic Blood Loss (Most Important in High-Resource Countries)
- GI tract: peptic ulcers, colon cancer, hemorrhoids, angiodysplasia
- Female genital tract: menorrhagia, metrorrhagia, endometrial cancer
- Key clinical rule: Iron deficiency in adult males or postmenopausal females in high-income countries must be attributed to gastrointestinal blood loss until proven otherwise - to do otherwise risks missing a GI cancer or other bleeding lesion
Sequence of Depletion (Insidious Progression)
- Iron stores depleted first - serum ferritin falls; no stainable iron in bone marrow macrophages (no anemia yet)
- Serum iron falls, transferrin (TIBC) rises - increased erythroid activity in bone marrow but still compensated
- Frank anemia appears - when stores are completely depleted; low serum iron and ferritin, low transferrin saturation, microcytic hypochromic anemia, impaired work capacity, cognitive performance, and immunocompetence
Morphology
Bone marrow:
- Mild to moderate increase in erythroid progenitors
- Absence of stainable iron in macrophages - the most diagnostically significant finding, best assessed with Prussian blue stain on aspirated marrow
Peripheral blood smear:

- Microcytic red cells (small)
- Hypochromic red cells (pale) - the zone of central pallor normally occupies ~1/3 of cell diameter; in iron deficiency, this is enlarged and hemoglobin may be seen only as a narrow peripheral rim
- Poikilocytosis: characteristic "pencil cells" (small, elongated cells)
- Thrombocytosis (elevated platelet count) is often seen for unclear reasons
Clinical Features
Symptoms (mostly mild and nonspecific):
- Most cases are mild and asymptomatic
- Weakness, listlessness, pallor in moderate-to-severe cases
- Dominating signs/symptoms often relate to the underlying cause (GI disease, gynecologic disorder, malnutrition)
Features of severe/long-standing iron deficiency (depletion of iron-containing enzymes throughout the body):
- Koilonychia (spoon nails) - thinning, flattening, "spooning" of fingernails
- Alopecia
- Atrophic changes in the tongue (atrophic glossitis) and gastric mucosa
- Intestinal malabsorption
- Pica - compulsion to eat non-foodstuffs (dirt, clay) or specific food ingredients like ice (pagophagia) or flour; due to iron depletion from the CNS
- Plummer-Vinson syndrome (rare triad): microcytic hypochromic anemia + atrophic glossitis + esophageal webs
Laboratory Findings
| Test | Finding in IDA |
|---|---|
| Hemoglobin / Hematocrit | Decreased (usually moderate) |
| Red cell morphology | Microcytic, hypochromic, poikilocytosis (pencil cells) |
| Serum ferritin | Low (<12 μg/L) |
| Serum iron | Low |
| TIBC (transferrin) | Elevated |
| Transferrin saturation | Reduced to <15% |
| Serum hepcidin | Low (reduced iron stores inhibit hepcidin synthesis) |
| Platelet count | Often elevated |
| Erythropoietin | Elevated (but marrow response blunted by iron deficiency) |
| Bone marrow Prussian blue | No stainable iron in macrophages |
Response to treatment: Oral iron supplementation produces a rise in reticulocytes within 5-7 days, followed by a steady increase in blood counts and normalization of red cell indices.
Key Clinical Maxim (Robbins)
"Persons often die with iron deficiency anemia but virtually never of it. An important point to remember is that in well-nourished persons, microcytic hypochromic anemia is not a disease but rather a symptom of another underlying disorder (e.g., colon cancer leading to chronic blood loss)."
- Robbins & Kumar Basic Pathology, p. 393
Differentiating IDA from Anemia of Chronic Inflammation
| Feature | IDA | Anemia of Chronic Inflammation |
|---|---|---|
| Serum iron | Low | Low |
| TIBC | Increased | Decreased |
| Serum ferritin | Low | Increased (or normal) |
| Bone marrow iron stores | Absent | Increased/present |
| Hepcidin | Low | Elevated |
The key distinguishing point: in anemia of chronic inflammation, iron is trapped in macrophages (elevated ferritin, reduced TIBC) due to inflammatory upregulation of hepcidin - the opposite pattern from true IDA.
This is a shared conversation. Sign in to Orris to start your own chat.