Placental site trophoblastic tumors and make detail s p df
Reading File
Finding Sources
Finding Sources
Searching PubMed
"placental site trophoblastic tumor" diagnosis treatment
Reading File
Reading File
Reading File
Reading Article
PMID: 39322463
Reading File
Finding Sources
Reading Article
PMID: 40631439
Finding Sources
Finding Sources
Loading Image
Loading Image
Reading File
Finding Sources
Reading File
Running Command
ls /home/daytona/workspace/ 2>/dev/null && echo "---" && python3 -c "import repo…
Running Command
mkdir -p /home/daytona/workspace/pstt-pdf && cat > /home/daytona/workspace/pstt-…
Running Command
cd /home/daytona/workspace/pstt-pdf && python3 generate_pstt_pdf.py 2>&1
Running Command
ls -lh /home/daytona/workspace/pstt-pdf/PSTT_Detailed_Review.pdf
Your detailed PSTT PDF is ready (6.2 MB, ~18 sections):
PSTT Detailed Review
PDF Document · PDF
What's Inside - Placental Site Trophoblastic Tumor: Full Summary
Cell of Origin
PSTT arises from extravillous (intermediate) trophoblasts - the cells that normally invade the maternal decidua and myometrium during implantation. These cells overlap cytotrophoblast and syncytiotrophoblast features but are distinct from both.
Key Distinguishing Features vs. Choriocarcinoma
| Feature | PSTT | Choriocarcinoma |
|---|---|---|
| hCG | Low / normal | Markedly elevated |
| Primary marker | hPL | hCG |
| Histology | Mononuclear cells, vessel invasion | Biphasic, hemorrhage, necrosis |
| Chemo sensitivity | Resistant | Highly sensitive |
| Primary Rx | Hysterectomy | Chemotherapy |
| WHO risk score | Not applied | Applied |
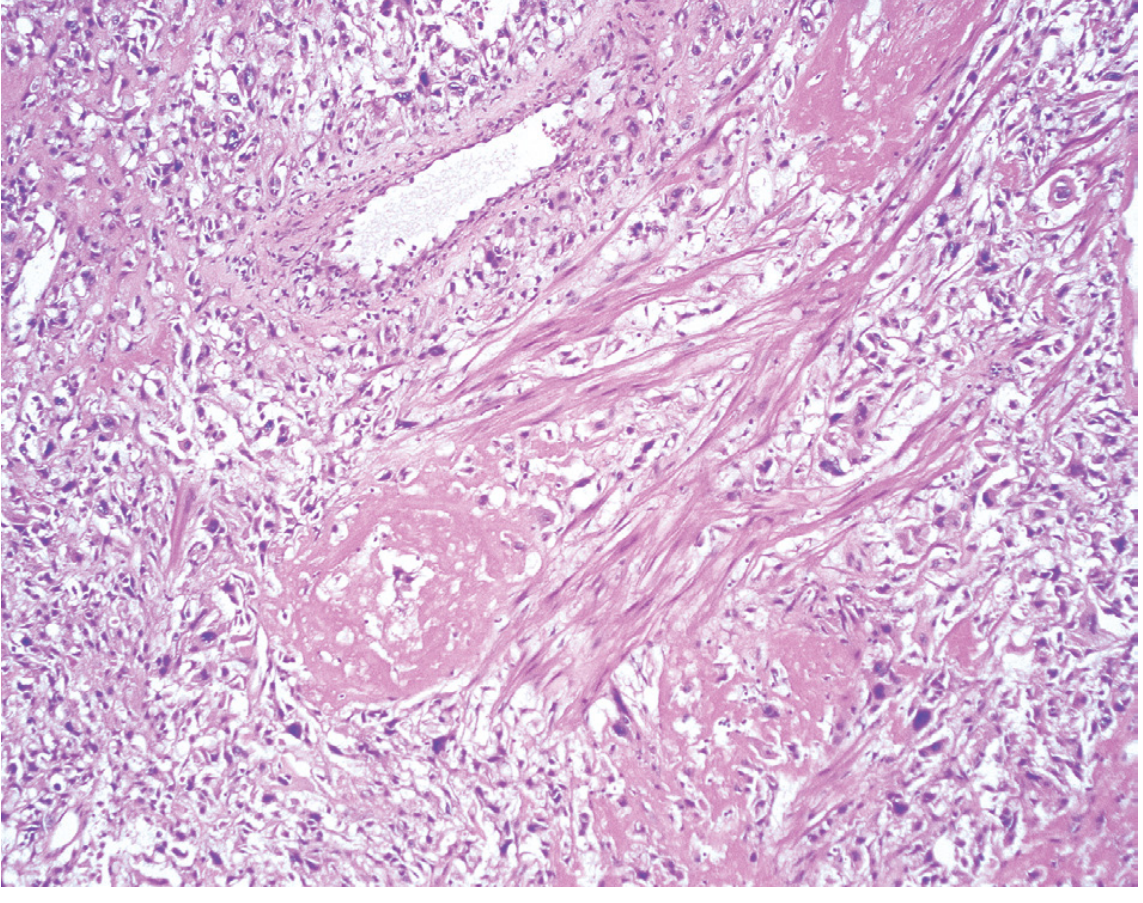
Pathology
- Polygonal mononuclear/binucleated cells with abundant cytoplasm
- "Splay-apart" invasion of smooth muscle fibers without destruction
- Fibrinoid deposition; replaces vascular endothelium
- IHC: hPL strong+, hCG focal+, Mel-CAM+, p63 negative (p63+ = ETT, not PSTT)
Histology image below (from Robbins Pathologic Basis of Disease):
Staging & Risk (FIGO)
- Stage I (uterus confined) = low risk; surgery curative in >90%
- High risk = Stage II+ OR interval from antecedent pregnancy >= 48 months
Treatment
- Hysterectomy - primary and often curative for Stage I
- Multi-agent chemotherapy (EMA-CO, EMA-EP, TP/TE) for high-risk/metastatic disease
- Pembrolizumab (anti-PD-1) - now considered in recurrent/refractory disease per 2024-2025 updates (Wang et al. 2024; Ngan et al. 2025)
- Fertility-sparing surgery - only for carefully selected Stage I patients (limited case reports)
ETT vs. PSTT
ETT (Epithelioid Trophoblastic Tumor) is a closely related but distinct entity: p63 positive, hyaline material, geographic necrosis, tends to be cervical. Both are managed primarily with surgery.
Sources: Robbins Basic Pathology 10e, Robbins Pathologic Basis of Disease 10e, Berek & Novak's Gynecology 16e, PubMed PMID 39322463 & 40631439.
This is a shared conversation. Sign in to Orris to start your own chat.