Hyperpigmentation on face / cheeks
Reading File
Finding Sources
Finding Sources
Searching PubMed
facial hyperpigmentation melasma treatment
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have rich content from textbooks. Let me compile the comprehensive answer.
Hyperpigmentation on the Face / Cheeks
Facial hyperpigmentation is an increase in melanin deposition causing brown/dark patches on the face. The most common cause on the cheeks is melasma, but several other entities must be considered.
Clinical Image
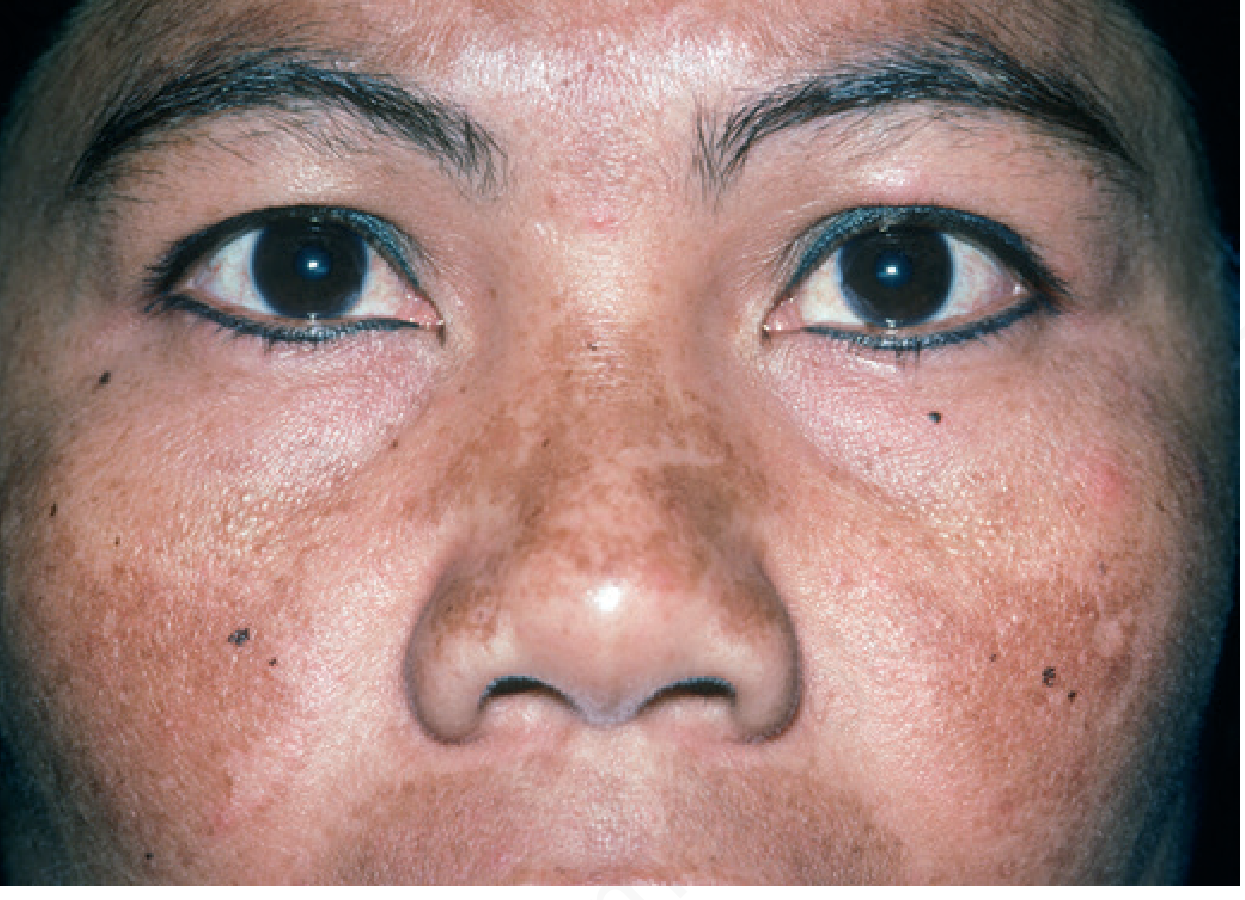
Melasma showing bilateral malar (cheek) and centrofacial hyperpigmentation - Andrews' Diseases of the Skin
Differential Diagnosis of Facial Hyperpigmentation
| Condition | Pattern | Key Clues |
|---|---|---|
| Melasma | Symmetric, malar/centrofacial | Women, pregnancy, OCP, sun exposure |
| Post-inflammatory hyperpigmentation (PIH) | Corresponds to prior lesion site | History of acne, eczema, injury |
| Solar lentigines | Discrete flat spots | Older age, sun-exposed areas |
| Freckles (ephelides) | Small, discrete | Fair skin, sun-dependent, fade in winter |
| Drug-induced pigmentation | Variable | Minocycline, amiodarone, antimalarials |
| Addison's disease | Diffuse + mucosal | Fatigue, hypotension, hyponatremia |
| Lichen planus pigmentosus | Dusky brown | Often diffuse, face/neck |
Melasma - The Most Common Cause on Cheeks
Pathogenesis
Melasma has two primary triggers: UV/sun exposure and female sex hormones.
-
Affects darker skin types preferentially (Fitzpatrick IV-V): East/Southeast/West Asians, Hispanics, Black individuals
-
Melasma patients have a lower minimal erythema dose (MED) to UV light and pigment more easily
-
Worsens in summer, affects sun-exposed facial skin
-
Associated with increased Wnt signaling (stimulates melanogenesis) and solar elastosis in affected skin
-
Hormonal triggers: pregnancy (up to 70% of pregnant women), oral contraceptives, hormone replacement therapy, phenytoin, finasteride therapy
-
OCP/HRT discontinuation rarely clears it quickly - may persist for years; pregnancy melasma usually clears within months of delivery
-
Andrews' Diseases of the Skin, p. 993
Clinical Patterns (Three Types)
- Centrofacial - forehead, nose, upper lip, chin (most common)
- Malar - cheeks/nose (most common alongside centrofacial)
- Mandibular - jawline (least common)
Most patients have multiple pattern types. Patches are sharply demarcated and brown.
Epidermal vs. Dermal Melasma
- Epidermal melasma: Wood's light accentuates pigment (responds better to treatment)
- Dermal melasma: Wood's light does not enhance it; dermal melanophages present; more treatment-resistant
- Most cases have both components - a therapeutic trial should be offered regardless of Wood's light findings
Post-Inflammatory Hyperpigmentation (PIH)
PIH follows any inflammatory skin condition (acne, eczema, psoriasis, dermatitis, cosmetic procedures):
Two mechanisms:
- Increased epidermal pigmentation via increased melanocyte activity
- Dermal melanosis - melanin "dropout" from epidermis into dermis (melanophages in upper dermis)
- More common in Fitzpatrick types IV-VI
- Tends to be tan to brown; gray hue suggests dermal involvement
- Often resolves spontaneously once the triggering inflammation is controlled
- Andrews' Diseases of the Skin, p. 993
Treatment
1. Sun Protection (First and Most Important Step)
- Broad-spectrum UVA/UVB sunscreen (SPF 30+) daily - also blocks visible light, which can worsen melasma
- Sun protection alone modestly improves melasma AND enhances efficacy of bleaching agents
2. Topical Depigmenting Agents
| Agent | Notes |
|---|---|
| Hydroquinone (HQ) | Gold standard; 2% OTC, 4% prescription. Inhibits tyrosinase. Most effective topical agent. |
| Tretinoin (retinoic acid) | Enhances HQ efficacy; some effect alone. Increases cell turnover, disperses melanin |
| Kligman's Triple Combination | HQ + tretinoin + topical corticosteroid - most effective topical regimen. Twice-weekly for maintenance. Overuse causes telangiectasias, acneiform eruptions, hypertrichosis. Prolonged HQ use risks exogenous ochronosis |
| Azelaic acid | Dicarboxylic acid; useful for melasma and PIH; well-tolerated |
| Kojic acid | Tyrosinase inhibitor; second-line |
| Niacinamide | Inhibits melanosome transfer |
| Tranexamic acid (oral/topical/intradermal) | Emerging evidence; intradermal injection supported by recent meta-analysis (PMID 39574359) |
3. Procedural Options (Use with Caution)
- Chemical peels (glycolic acid, salicylic acid, TCA) - mixed evidence; risk of PIH if irritation occurs; recent systematic review (PMID 38530985) supports use in melasma
- Intense pulsed light (IPL) - can improve melasma but high relapse rate; risk of PIH
- Q-switched Nd:YAG laser (1064 nm) - used for melasma but can paradoxically increase pigmentation; low-fluence protocols used
- Fractional CO2 laser - used for refractory PIH with caution
- All laser/light treatments carry higher PIH risk in darker skin types
4. For PIH Specifically
- Treat the underlying cause first (e.g., control acne)
- Hydroquinone for Wood's light-enhancing (epidermal) lesions
- Tretinoin to enhance HQ effect
- Laser/chemical peels must be done with extreme caution in darker patients - results unpredictable
Recent Evidence (2024-2026)
- Chemical peels for melasma [Systematic Review, Sarkar R, 2024 - PMID 38530985]: Supports peels as adjuncts to topical therapy
- Tranexamic acid intradermal injection [Systematic Review + Meta-analysis, Chen LY, 2025 - PMID 39574359]: Effective for adult melasma in RCTs
- Thiamidol (isobutylamido thiazolyl resorcinol) [Systematic Review, Klein PA, 2024 - PMID 39496126]: A newer topical tyrosinase inhibitor showing clinical efficacy for hyperpigmentation
- Solar lentigines treatment [Systematic Review, Mardani G, 2025 - PMID 40145274]: Laser and light treatments effective for solar lentigines specifically
When to Investigate Further
Consider systemic workup if:
- Diffuse or rapidly progressive pigmentation (rule out Addison's disease - check cortisol, ACTH, electrolytes)
- No obvious sun/hormonal trigger
- Associated systemic symptoms (fatigue, weight loss, GI symptoms)
- Drug history (minocycline, amiodarone, antimalarials, chemotherapy)
Key takeaway: Facial cheek hyperpigmentation is usually melasma. First-line = strict sun protection + topical hydroquinone ± tretinoin. Kligman's triple combination is the most effective topical regimen. All procedural treatments carry risk of worsening pigmentation, especially in darker skin types.
Sources: Andrews' Diseases of the Skin (Clinical Dermatology), Fitzpatrick's Dermatology Vol. 1-2, Dermatology 2-Volume Set 5e (Bolognia)
How to use hyderquin plus for it
Searching the Web
Hydroquin Plus cream composition hydroquinone tretinoin how to use instructions
Finding Sources
I have all the information needed for a clear, practical guide.
How to Use Hydroquin Plus for Facial Hyperpigmentation
Hydroquin Plus is a triple-combination cream containing:
- Hydroquinone 4% - tyrosinase inhibitor (reduces melanin production)
- Tretinoin - retinoid that increases skin cell turnover and enhances HQ penetration
- Mild corticosteroid (e.g., fluocinolone or hydrocortisone) - reduces inflammation and irritation from the other two ingredients
This is essentially Kligman's formula, considered the most effective topical regimen for melasma and facial hyperpigmentation.
Step-by-Step Application
Nighttime (Only - Do NOT Use in the Morning)
- Cleanse - Wash face gently with a mild, alcohol-free cleanser using your fingers (no washcloth). Rinse and pat dry.
- Wait 10 minutes - Let skin fully dry before applying. Damp or moist skin absorbs the cream too quickly and increases irritation risk.
- Apply the cream - Use a pea-sized/small amount only. Apply sparingly to the hyperpigmented (darker) patches and extend about 1 cm (½ inch) onto the surrounding normal skin. Gently rub in until it becomes nearly invisible. If you can still see white cream, you've used too much.
- Wash your hands thoroughly after applying - HQ can discolor fingernails and the skin around them.
- Do not cover with bandages or occlusive dressings unless specifically directed.
Morning Routine (Essential)
- Wash face gently
- Apply a moisturizer if needed (dryness is common, especially from tretinoin)
- Apply broad-spectrum SPF 30+ sunscreen - this step is non-negotiable. Sun exposure undoes the effect of the cream completely. Cover the treated areas from all UV and visible light.
Frequency and Duration
| Phase | Frequency |
|---|---|
| Starting | Once daily at night |
| Ongoing treatment | Once nightly, for up to 8-12 weeks |
| Maintenance (after improvement) | Taper to 2-3 nights per week |
| Maximum use | Do NOT use continuously for more than 5-6 months without a break |
Do not stop abruptly after achieving results - taper gradually (e.g., 3x/week for 2 weeks, then 2x/week for 2 weeks, then stop). Abrupt stopping can cause rebound pigmentation from a "tyrosinase rebound" effect.
What to Avoid
- Do not use in the morning - tretinoin is photosensitized and degrades in sunlight
- Avoid the eye area, nostrils, and mouth - the skin there is too thin and sensitive
- Do not apply to broken, sunburned, or irritated skin
- Avoid harsh astringents, alcohol-based toners, AHAs (glycolic acid), vitamin C serums on treated areas unless already tolerated - combining too many actives increases irritation
- No waxing, electrolysis, or hair removal on treated areas
- Avoid sunbeds entirely during treatment
- If traveling to a very sunny destination, stop the cream 1 week before
When to Expect Results
- Visible improvement takes 4-8 weeks minimum
- Significant results at 2-3 months
- Full effect may take up to 6 months
Side Effects to Watch For
| Side Effect | What to Do |
|---|---|
| Mild redness, dryness, peeling | Normal - usually settles in 2-4 weeks as skin adapts |
| Burning or stinging | Reduce frequency to every other night temporarily |
| Skin becomes darker with treatment | Stop and see your doctor - this indicates irritation-driven PIH |
| Prolonged redness, acne-like breakouts, fine hair growth | Overuse signs - reduce dose or take a break |
| Gray-blue skin discoloration | Rare - exogenous ochronosis from prolonged HQ overuse - stop immediately |
Key Reminders
- Sunscreen every morning is mandatory - without it, the cream will not work
- This cream is not for long-term continuous use due to the steroid component
- Results will be lost without ongoing sun protection, even after stopping the cream
- If no improvement after 3 months, see a dermatologist - may need a peel, laser, or alternative agent
Based on: Andrews' Diseases of the Skin (Clinical Dermatology); Fitzpatrick's Dermatology; Cleveland Clinic & Mayo Clinic drug information for fluocinolone/hydroquinone/tretinoin combination cream
Is it use for dark circles
Finding Sources
Searching the Web
hydroquinone tretinoin cream dark circles under eyes periorbital safe use
Can Hydroquin Plus Be Used for Dark Circles?
The Short Answer
Hydroquin Plus (the full triple combination) is generally NOT recommended directly under the eyes - but the situation is nuanced depending on the cause of your dark circles and which ingredient you're using.
Why Dark Circles Are Different
Dark circles have multiple causes, and hyperpigmentation is only one of them:
| Cause | Type | Responds to HQ cream? |
|---|---|---|
| Melanin/pigmentation (brown discoloration) | Pigmentary | Possibly yes - with caution |
| Vascular (bluish/purplish hue from blood vessels showing through thin skin) | Vascular | No - HQ won't help |
| Structural/hollow (shadow from volume loss, fat pads) | Structural | No - needs filler or surgery |
| Fatigue/lifestyle | Temporary | No |
So first: the cause of your dark circles matters. Only the pigmentary (brown) type may respond to a lightening cream at all.
Why Hydroquin Plus Specifically Is Risky Around the Eyes
The under-eye skin is the thinnest skin on the body (0.5 mm vs 2 mm elsewhere). Because of this:
- Tretinoin is a strong irritant - it commonly causes dryness, peeling, and redness. Under the eye this can cause significant inflammation and paradoxically worsen pigmentation (post-inflammatory hyperpigmentation)
- Corticosteroid component - long-term use around the eyes is a serious concern. It can cause:
- Periorbital skin thinning (making dark circles worse long-term)
- Steroid-induced glaucoma - steroids absorbed near the eye can raise intraocular pressure
- Cataracts with prolonged use
- Hydroquinone alone has been used safely in the periocular area, but the full triple combination is too harsh for routine eye area use
The FDA-approved triple combination (HQ 4% / tretinoin 0.05% / fluocinolone) is approved for melasma but its long-term use in the periorbital area is a specific concern due to the steroid component - PMC Periorbital Hyperpigmentation Review
What Actually Works for Periorbital (Under-Eye) Pigmentation
If your dark circles are the pigmentary (brown) type:
| Treatment | Notes |
|---|---|
| Hydroquinone 4% alone (without tretinoin/steroid) | Studied specifically for periorbital pigmentation - safer option |
| Kojic acid cream | Tyrosinase inhibitor, gentler alternative |
| Vitamin C serum (ascorbic acid) | Antioxidant, brightens pigmentation, safe for eye area |
| Niacinamide | Inhibits melanin transfer, very well-tolerated |
| Azelaic acid | Gentle, suitable near the eye area |
| Tretinoin alone (very low concentration, 0.025%) | Can be used under-eye with great caution, sparingly |
| Chemical peels (lactic acid, TCA - done by dermatologist) | Professional option for resistant pigmentation |
| Q-switched Nd:YAG or fractional laser | For pigmentary dark circles, done by specialist |
| Sunscreen daily | Essential regardless of treatment |
Bottom Line
- Do NOT apply Hydroquin Plus directly under the eyes - the steroid and high-strength tretinoin make it unsafe for the periorbital area
- If your dark circles are brown/pigmentary, see a dermatologist who can prescribe a hydroquinone-only eye-area formulation or guide you on safer alternatives
- If your dark circles are bluish/hollow/structural, Hydroquin Plus will do nothing for them regardless
This is a shared conversation. Sign in to Orris to start your own chat.