Explain me 10 commen heart diseases with ecg changes and ecg images of those diseases
Reading File
Finding Sources
Searching Images
ECG changes myocardial infarction ST elevation
Finding Sources
Searching Images
atrial fibrillation ECG irregularly irregular rhythm
Searching Images
heart block complete AV block ECG bradycardia
Searching Images
ventricular tachycardia ECG wide complex tachycardia
Searching Images
hypertrophic cardiomyopathy ECG left ventricular hypertrophy voltage
Searching Images
pericarditis ECG saddle shape ST elevation diffuse
Searching Images
Wolff-Parkinson-White syndrome ECG delta wave short PR
Searching Images
pulmonary embolism ECG S1Q3T3 right heart strain sinus tachycardia
Searching Images
dilated cardiomyopathy ECG bundle branch block low voltage
I now have excellent ECG images for all 10 conditions. Let me compose the comprehensive answer.
10 Common Heart Diseases — ECG Changes & Images
1. ST-Elevation Myocardial Infarction (STEMI)
What it is: Complete occlusion of a coronary artery causing transmural myocardial ischemia and death.
ECG Changes:
- ST elevation ≥1 mm in ≥2 contiguous leads (≥2 mm in V1–V3)
- Hyperacute (peaked) T-waves — earliest sign
- Reciprocal ST depression in opposing leads
- Pathological Q waves develop within hours (indicate necrosis)
- T-wave inversion in the subacute phase
- Tombstone morphology in severe anterior STEMI
| Territory | Leads with ST elevation | Culprit artery |
|---|---|---|
| Anterior | V1–V4 | LAD (proximal) |
| Anterolateral | V1–V6, I, aVL | LAD |
| Inferior | II, III, aVF | RCA / LCx |
| Posterior | Tall R in V1–V3 + ST depression V1–V3 | LCx / RCA |
ECG — Acute Anterolateral STEMI (LAD occlusion):

ECG — Inferior + Posterior STEMI (RCA/LCx occlusion):
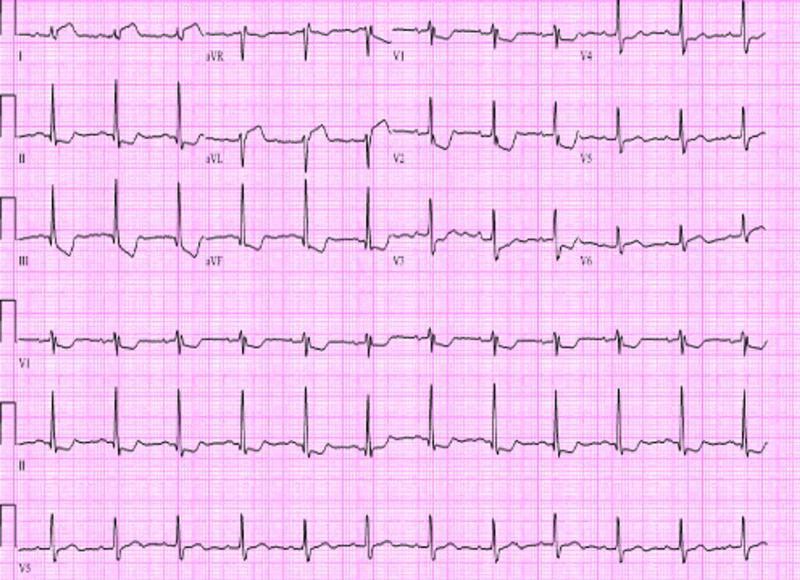
2. Atrial Fibrillation (AF)
What it is: Disorganized atrial electrical activity causing irregular ventricular response and loss of atrial kick.
ECG Changes:
- Absent P waves — replaced by low-amplitude fibrillatory (f) waves, best seen in V1 and II
- Irregularly irregular R-R intervals — hallmark finding
- Narrow QRS (unless aberrant conduction/bundle branch block)
- Ventricular rate varies: controlled (<100 bpm), uncontrolled (>100 bpm)
ECG — Atrial Fibrillation:
3. Complete (Third-Degree) Heart Block
What it is: Total failure of AV conduction — atria and ventricles beat independently.
ECG Changes:
- Complete AV dissociation — P waves and QRS complexes are independent, no fixed PR interval
- Atrial rate > ventricular rate (e.g., atrial 80 bpm, ventricular 30–40 bpm)
- Escape rhythm QRS: narrow if junctional (AV nodal block), wide/bizarre if ventricular (infra-Hisian)
- Severe bradycardia
- Prolonged QTc common with ventricular escape
ECG — Complete AV Block:

4. Ventricular Tachycardia (VT)
What it is: Life-threatening arrhythmia arising from a ventricular focus, rate >100 bpm.
ECG Changes:
- Wide complex tachycardia (QRS ≥120 ms) at rate 100–250 bpm
- AV dissociation — P waves independent of QRS (pathognomonic when visible)
- Fusion beats and capture beats (diagnostic when present)
- Concordance — all precordial leads positive or all negative
- North-West axis (aVR positive, negative in I and aVF)
- No preceding P waves
Brugada criteria help differentiate VT from SVT with aberrancy.
ECG — Monomorphic Ventricular Tachycardia:

5. Acute Pericarditis
What it is: Inflammation of the pericardium, often viral, causing diffuse pericardial irritation.
ECG Changes (4 stages):
- Stage 1 (acute): Diffuse concave ("saddle-shaped") ST elevation in almost all leads (except aVR, V1 which show reciprocal depression); PR segment depression (best seen in II and V5); Spodick's sign (downsloping TP segment)
- Stage 2: ST returns to baseline, T-waves flatten
- Stage 3: Diffuse T-wave inversions
- Stage 4: ECG normalizes
Key distinguishing features from STEMI: diffuse distribution not following one coronary territory, concave (not convex) ST elevation, PR depression, no Q waves.
ECG — Acute Pericarditis:

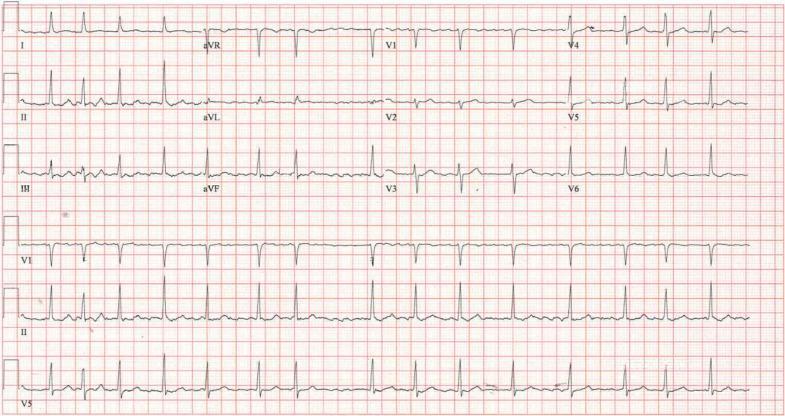
6. Hypertrophic Cardiomyopathy (HCM)
What it is: Genetic disorder causing asymmetric myocardial hypertrophy (usually interventricular septum), a leading cause of sudden cardiac death in young athletes.
ECG Changes:
- Left ventricular hypertrophy (LVH) voltage criteria — Sokolow–Lyon: S in V1 + R in V5/V6 ≥35 mm
- Deep symmetric ("giant") T-wave inversions — most prominent in V4–V6 (apical HCM/Yamaguchi variant)
- Pathological Q waves in lateral/inferior leads (septal hypertrophy)
- Left axis deviation
- Non-specific ST depression
- May show AF or pre-excitation
ECG — Apical Hypertrophic Cardiomyopathy (Yamaguchi Syndrome):
7. Pulmonary Embolism (PE)
What it is: Thrombus lodging in pulmonary vasculature causing acute right ventricular pressure overload.
ECG Changes:
- Sinus tachycardia — most common finding (>44% of cases)
- S1Q3T3 pattern (McGinn-White sign): prominent S wave in I, Q wave in III, T-wave inversion in III
- Right heart strain: T-wave inversions in V1–V4
- Incomplete/complete RBBB — due to right ventricular strain
- Right axis deviation
- P pulmonale (peaked P waves in II/III/aVF)
- Atrial arrhythmias (AF, flutter)
- Massive PE may show electrical alternans
ECG — Acute Pulmonary Embolism (S1Q3T3 pattern):

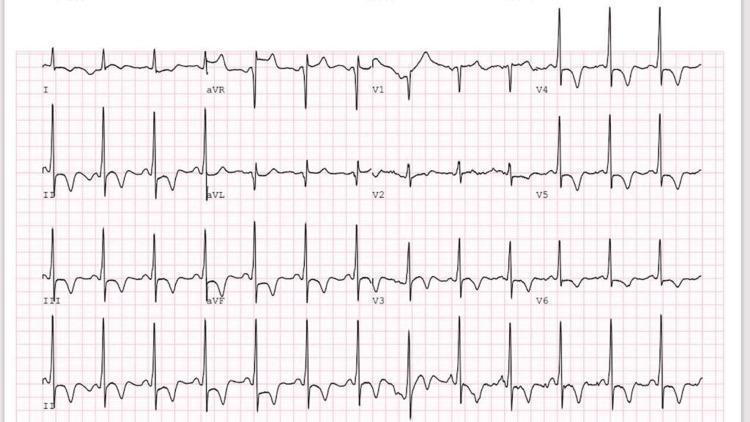
8. Wolff-Parkinson-White (WPW) Syndrome
What it is: Congenital accessory pathway (Bundle of Kent) bypasses the AV node, causing ventricular pre-excitation; risk of sudden death if AF develops with rapid conduction.
ECG Changes (classic triad):
- Short PR interval (<120 ms) — accessory pathway bypasses AV node delay
- Delta wave — slurred upstroke at the start of QRS (slow ventricular pre-excitation)
- Widened QRS (>120 ms) due to fusion of normal and anomalous conduction
- Secondary ST-T changes (discordant to QRS direction)
- "Pseudo-infarction" Q waves from negative delta waves (especially inferior leads)
- Pathway localization by delta wave polarity in 12 leads
ECG — WPW Syndrome:

9. Dilated Cardiomyopathy (DCM)
What it is: Dilation and systolic dysfunction of the left (or both) ventricles; causes include viral myocarditis, alcohol, ischemia, genetics.
ECG Changes:
- Left bundle branch block (LBBB) — broad notched R in I, V5, V6; QS in V1–V3 (most common)
- Non-specific intraventricular conduction delay
- Low QRS voltage in limb leads (<5 mm) — especially in infiltrative causes (amyloid)
- Poor R-wave progression in precordial leads
- Pathological Q waves (pseudo-infarction pattern)
- Atrial fibrillation (common in advanced disease)
- Frequent PVCs or ventricular tachycardia
- Left axis deviation
ECG — Dilated Cardiomyopathy (LBBB pattern):
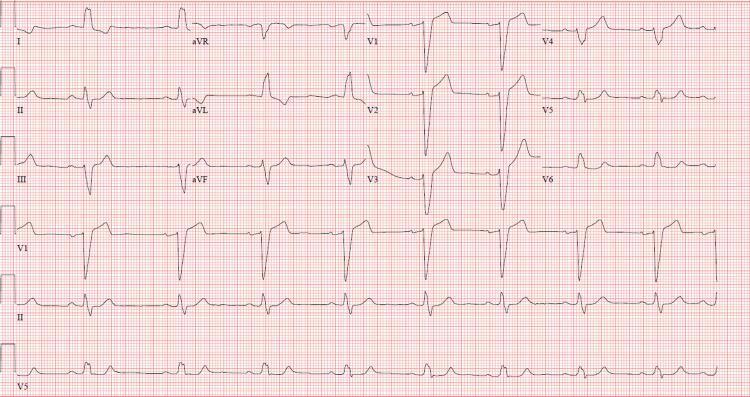
10. Inferior NSTEMI / Unstable Angina
What it is: Partial coronary occlusion or demand-supply mismatch causing subendocardial ischemia without transmural injury.
ECG Changes:
- ST depression ≥0.5 mm (horizontal or downsloping) in ≥2 contiguous leads — key marker
- T-wave inversions — symmetric, deep ("Wellens' warning" in V2–V3 = critical LAD stenosis)
- No ST elevation, no pathological Q waves
- May be dynamic — changes resolve with pain relief
- Transient ST elevation possible during ischemic episodes
- Normal ECG in ~30% at presentation — serial ECGs mandatory
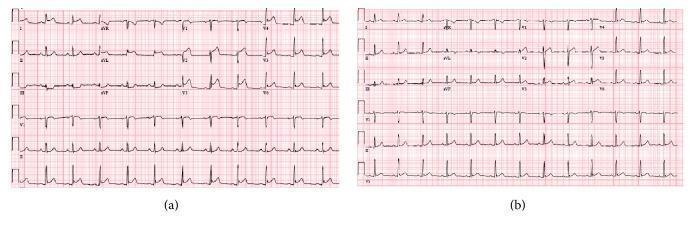
ECG — Anterior STEMI Before and After Treatment (showing dynamic changes):
Summary Table
| # | Disease | Key ECG Finding |
|---|---|---|
| 1 | STEMI | Convex ST elevation + reciprocal depression + Q waves |
| 2 | Atrial Fibrillation | No P-waves, irregularly irregular rhythm |
| 3 | Complete Heart Block | AV dissociation, slow escape rhythm |
| 4 | Ventricular Tachycardia | Wide complex tachycardia, AV dissociation |
| 5 | Acute Pericarditis | Diffuse saddle-shaped ST elevation + PR depression |
| 6 | Hypertrophic Cardiomyopathy | LVH voltage + giant T-wave inversions |
| 7 | Pulmonary Embolism | S1Q3T3 + sinus tachycardia + RBBB |
| 8 | WPW Syndrome | Short PR + delta wave + widened QRS |
| 9 | Dilated Cardiomyopathy | LBBB + low voltage + AF + PVCs |
| 10 | NSTEMI/Unstable Angina | ST depression + T-wave inversions (no Q waves) |
Clinical note: ECG interpretation must always be integrated with the clinical history, symptoms, biomarkers (troponin, BNP), and imaging. A normal ECG does not exclude serious cardiac pathology — serial tracings and continuous monitoring are often essential.
This is a shared conversation. Sign in to Orris to start your own chat.