heart attack in detail point wise manner
Reading File
Finding Sources
Finding Sources
Searching PubMed
"myocardial infarction"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have all the information needed for a comprehensive, point-wise answer. Here is the full detailed response:
Heart Attack (Myocardial Infarction) - A Complete Point-wise Overview
1. Definition
- Myocardial infarction (MI), commonly called a "heart attack," is necrosis of the heart muscle resulting from ischemia.
- The 2018 joint U.S./European Cardiology task force defines it as: "The presence of acute myocardial injury detected by abnormal cardiac biomarkers in the setting of evidence of acute myocardial ischemia."
- The underlying damage is irreversible once ischemia persists beyond 20-40 minutes - Robbins & Kumar Basic Pathology, p. 354
2. Epidemiology & Risk Factors
- ~10% of MIs occur before age 40; ~45% occur before age 65.
- Men are at greater risk than women; however, the gap narrows with age.
- Women are relatively protected during reproductive years, but menopause (declining estrogen) accelerates coronary artery disease.
- IHD is the most common cause of death in older adult women.
- Risk factors mirror those for atherosclerosis: hypertension, dyslipidemia, diabetes, smoking, obesity, family history, sedentary lifestyle - Robbins & Kumar Basic Pathology, p. 353
3. Classification (Types of MI)
Type 1 MI:
- Caused by atherosclerotic plaque rupture with acute thrombosis.
- Divided into STEMI (ST-elevation MI) and NSTEMI (non-ST-elevation MI).
- Treatment is revascularization (PCI or thrombolysis).
Type 2 MI:
- Caused by supply-demand mismatch (demand ischemia) - not plaque rupture.
- Examples: severe anemia, tachycardia, hypotension, hypertensive crisis.
- Treatment targets reducing cardiac oxygen demand.
Acute Coronary Syndrome (ACS) spectrum:
- STEMI → NSTEMI → Unstable Angina (no biomarker elevation in UA).
-
- Sabiston Textbook of Surgery, p. 2928
4. Pathogenesis - The Step-by-Step Sequence
In a typical MI, the following cascade occurs:
- Plaque disruption - An atheromatous plaque is eroded or suddenly disrupted by endothelial injury, intraplaque hemorrhage, or mechanical forces, exposing subendothelial collagen and necrotic plaque contents to blood.
- Platelet activation - Platelets adhere, aggregate, and release thromboxane A₂, ADP, and serotonin, causing further platelet aggregation and vasospasm.
- Coagulation cascade activation - Exposure of tissue factor activates coagulation, adding to the growing thrombus.
- Complete occlusion - The enlarging thrombus may completely occlude the coronary artery lumen within minutes.
- Angiography within 4 hours shows coronary thrombosis in ~90% of cases; by 12-24 hours, only 60% (some occlusions spontaneously lyse).
- 10% of MIs occur without occlusive atherosclerosis - causes include vasospasm, embolism from atrial fibrillation, or valve vegetations. - Robbins & Kumar Basic Pathology, p. 353
5. Progression of Myocardial Necrosis
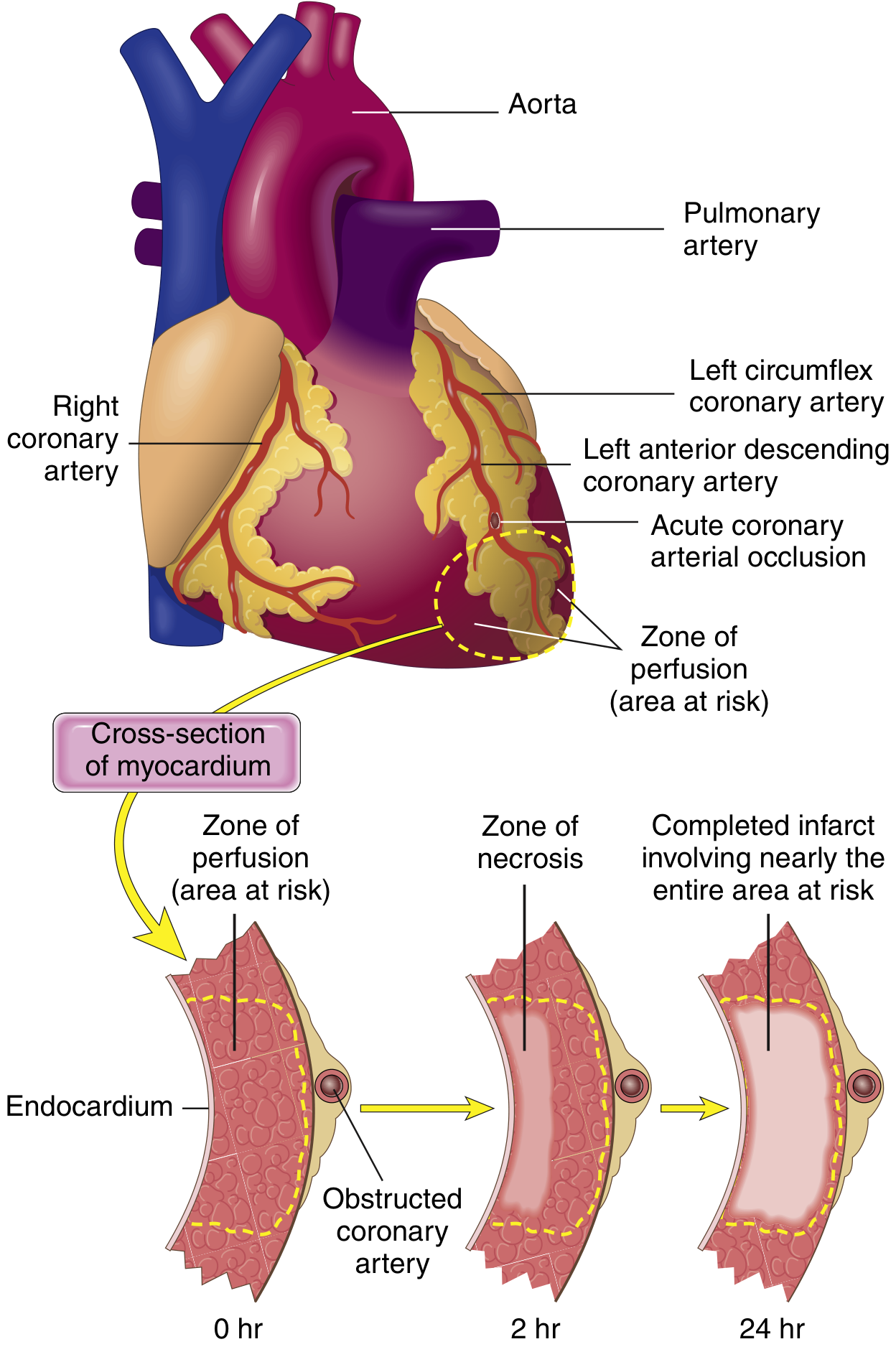
- Within seconds: aerobic metabolism ceases; ATP drops; lactic acid accumulates.
- Within minutes: loss of contractility (reversible at this stage).
- 20-40 minutes: irreversible damage begins; sarcolemmal membrane disruption allows intracellular macromolecules (troponins) to leak out.
- Necrosis begins in the subendocardial zone (most vulnerable - furthest from epicardial vessels, highest intramural pressure).
- A wavefront of cell death then moves outward toward the epicardium.
- Without intervention, a transmural infarct develops fully in 3-6 hours. - Robbins & Kumar Basic Pathology, p. 354-355
6. Infarct Location by Artery Involved
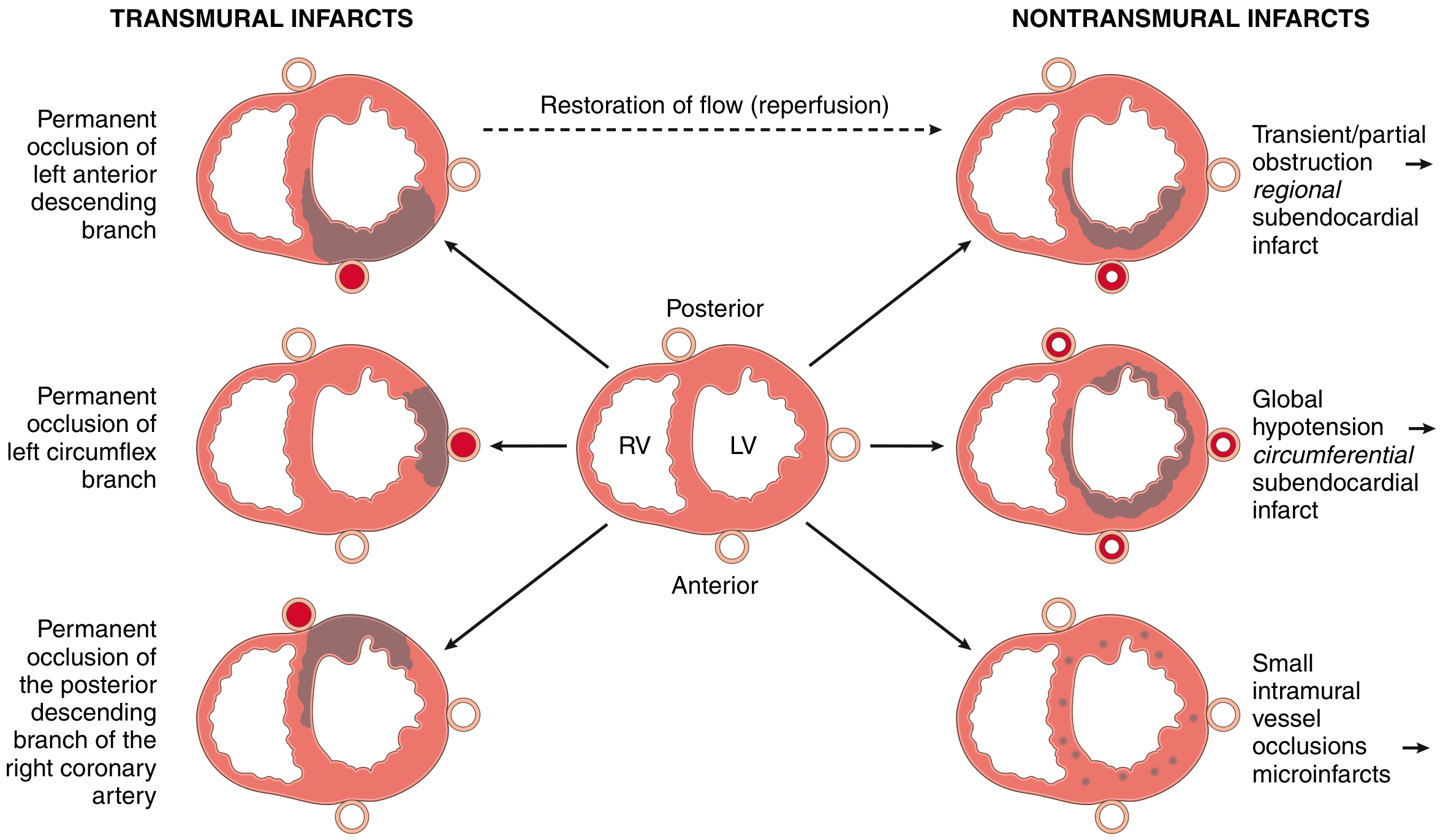
| Artery | % of MIs | Territory Affected |
|---|---|---|
| Left Anterior Descending (LAD) | 40-50% | Anterior LV wall, anterior 2/3 of septum, cardiac apex |
| Right Coronary Artery (RCA) | 30-40% | Right ventricle, posterior LV wall, posterior 1/3 of septum |
| Left Circumflex (LCX) | 15-20% | Lateral left ventricle |
- Proximal LAD occlusions are often fatal; distal occlusions may affect only the apex.
- Isolated RV infarcts occur in only 1-3% of IHD cases.
-
- Robbins & Kumar Basic Pathology, p. 355-356
Types of Infarcts:
- Transmural infarct - Full thickness of ventricular wall; from total epicardial vessel occlusion (classic STEMI).
- Subendocardial infarct - Limited to inner 1/3 of myocardium; often from partial/transient occlusion or severe global hypoperfusion (NSTEMI pattern).
- Microscopic infarct - Small-vessel occlusions (vasculitis, emboli, cocaine-induced vasospasm); may show no ECG changes.
7. Morphological Changes Over Time (Pathological Timeline)
| Time Frame | Gross Features | Light Microscopy | Electron Microscopy |
|---|---|---|---|
| 0-30 min | None (reversible) | None | Relaxation of myofibrils; glycogen loss; mitochondrial swelling |
| 30 min - 4 hrs | None | Variable fiber waviness at border | Sarcolemmal disruption; mitochondrial amorphous densities |
| 4-12 hrs | Occasional dark mottling | Coagulation necrosis onset; edema; hemorrhage | - |
| 12-24 hrs | Dark mottling | Coagulation necrosis; pyknotic nuclei; hypereosinophilic myocytes; early neutrophilic infiltrate | - |
| 1-3 days | Yellow-tan infarct center | Coagulation necrosis with loss of nuclei and striations; increased neutrophils | - |
| 3-7 days | Hyperemic border; central softening | Neutrophil disintegration; macrophage phagocytosis begins at border | - |
| 7-10 days | Maximally yellow-tan and soft | Well-developed macrophage phagocytosis; early granulation tissue at margins | - |
| 10-14 days | Red-gray depressed borders | Well-established granulation tissue | - |
| 2-8 weeks | Gray-white scar forming | Collagen deposition | - |
| >2 months | Dense white scar | Dense collagen scar; fully healed | - |
- Myocardial necrosis proceeds invariably to scar - no significant regeneration occurs. - Robbins & Kumar Basic Pathology, p. 357
8. Clinical Features (Symptoms)
Classic Presentation:
- Crushing/squeezing chest pain - central, often described as "pressure," "tightness," or "heaviness"
- Radiation - to left arm, jaw, neck, back, or epigastrium
- Duration - typically >30 minutes (unlike angina which resolves within 20 min)
- Diaphoresis (profuse sweating)
- Nausea and vomiting
- Dyspnea (shortness of breath)
- Anxiety and sense of impending doom
- Palpitations (from arrhythmias)
Atypical Presentations (especially in women, elderly, diabetics):
- Epigastric pain or indigestion
- Fatigue, weakness
- Jaw or arm pain alone
- Silent MI (no pain, detected only on ECG or biomarkers)
- Women more often present without chest pain, which leads to delayed and less aggressive care - Symptom to Diagnosis, p. 175
9. ECG Changes
Three key electrical changes occur:
- Rapid repolarization of infarcted cells → current flows out of infarct → ST segment elevation
- Decreased resting membrane potential (K⁺ leaks out) → current flows into infarct during diastole → TQ depression (recorded as ST elevation)
- Delayed depolarization of infarcted cells → also causes ST segment elevation
ECG Evolution:
- Acute (hours): ST segment elevation in leads overlying the infarct; reciprocal ST depression in opposite leads
- Days to weeks: ST changes subside; Q waves appear (electrically silent dead muscle)
- Chronic: Q waves persist as a permanent marker of prior infarction
- NSTEMI: ST depression or T-wave changes, but no ST elevation; no Q waves typically
- Non-Q-wave infarcts tend to be less severe but carry high risk of reinfarction - Ganong's Review of Medical Physiology, p. 534-535
10. Cardiac Biomarkers
- Cardiac Troponin I and T - Most specific and sensitive; rise within 3-6 hours, peak at 12-24 hours, remain elevated 7-14 days (troponin T can persist up to 2 weeks).
- CK-MB - Rises within 3-6 hours; returns to normal within 48-72 hours (useful for detecting reinfarction).
- Myoglobin - Earliest to rise (1-3 hours) but not cardiac-specific; used for early rule-out.
- LDH - Rises later (24-48 hrs); was used historically but largely replaced by troponins.
- The 4th Universal Definition of MI classifies infarction based on rising/falling troponin pattern with at least one value above the 99th percentile. - Tietz Textbook of Laboratory Medicine, 7th Edition
11. Causes of Death After Acute MI
From Guyton & Hall:
- Decreased cardiac output (Cardiogenic shock) - Occurs when >40% of left ventricle is infarcted; mortality 40-50%. The infarcted segment undergoes systolic stretch (bulges outward during systole instead of contracting), further reducing effective pumping force.
- Pulmonary edema - Blood backs up into pulmonary circulation; elevated capillary pressure causes pulmonary edema, often days after the event as reduced renal perfusion leads to fluid retention.
- Ventricular fibrillation - Most common mechanism of sudden cardiac death; occurs in 80-90% of cardiac deaths from ischemia. Two danger windows: within 10 minutes and at 1-2 hours post-infarction. Caused by:
- Extracellular K⁺ elevation from leaking ischemic cells (increases irritability)
- Injury currents from partially depolarized ischemic areas
- Sympathetic activation (baroreceptor reflex response to low BP)
- Ventricular dilation increasing conduction pathway length
- Cardiac rupture - Rare; most likely between days 3-7 when the infarct is maximally soft (neutrophil-mediated dissolution), before adequate scar forms.
-
- Guyton & Hall Textbook of Medical Physiology, p. 271-272
12. Complications
Early (days):
- Arrhythmias (ventricular fibrillation, ventricular tachycardia, heart block, AF)
- Cardiogenic shock
- Acute left ventricular failure / pulmonary edema
- Right ventricular infarction (with proximal RCA occlusion) - gives low-output state with clear lungs
- Pericarditis (early, within 24-72 hours - overlies the infarct zone)
Subacute (days to weeks):
- Papillary muscle rupture (mitral regurgitation)
- Interventricular septum rupture (new VSD)
- Free wall rupture (cardiac tamponade)
- Mural thrombus formation (with risk of systemic embolism)
Late (weeks to months):
- Left ventricular aneurysm
- Dressler's syndrome (autoimmune pericarditis, 2-10 weeks post-MI)
- Chronic heart failure
- Sudden cardiac death from late arrhythmia (persistent risk)
13. Diagnosis - Summary
| Test | Finding |
|---|---|
| ECG | ST elevation (STEMI) or ST/T changes (NSTEMI); Q waves (old MI) |
| Troponin I/T | Rise and fall pattern; most definitive |
| Echo | Wall motion abnormality; LV function |
| Coronary angiography | Confirms occlusion; guides revascularization |
| CXR | May show pulmonary edema or widened mediastinum |
14. Treatment
Acute Management (STEMI):
A. Medications:
- Aspirin - Immediate 300 mg loading dose; antiplatelet (inhibits TXA₂)
- P2Y12 inhibitors - Clopidogrel, ticagrelor, or prasugrel; dual antiplatelet therapy
- Anticoagulation - Unfractionated heparin, LMWH, fondaparinux, or bivalirudin
- Nitroglycerin - Sublingual or IV; reduces preload, relieves chest pain (avoid in RV infarction as it reduces preload and can cause catastrophic hypotension)
- Beta-blockers - Cardioprotective; reduce oxygen demand and risk of arrhythmia (avoid if hypotension, reduced EF, bradycardia, or cardiogenic shock)
- High-intensity statins - Early HMG-CoA reductase inhibitors (target LDL <70 mg/dL)
- Oxygen - Only if patient is hypoxic (SpO₂ <90%)
- Morphine - For pain not relieved by nitrates (though routine use now questioned)
B. Reperfusion (most time-critical intervention):
- Primary PCI (percutaneous coronary intervention) with stent placement is the gold standard - lower mortality, lower hemorrhagic stroke risk vs. thrombolysis
- Systemic thrombolysis (tPA, streptokinase) - Only if PCI cannot be delivered within 2 hours of presentation
- Both are most effective within 12 hours of symptom onset
- Even patients requiring transfer to a PCI-capable center have better outcomes with PCI than bedside thrombolysis
C. Post-reperfusion (secondary prevention):
- Beta-blockers (survival benefit)
- ACE inhibitors (reduce remodeling, especially if EF is reduced)
- Aspirin (lifelong)
- P2Y12 inhibitor (duration based on stent type and bleeding risk)
- High-intensity statins
- Glycoprotein IIb/IIIa inhibitors (recommended if stenting was performed)
D. NSTEMI management:
- Similar medical therapy; PCI can be delayed up to 72 hours in many cases
- No systemic thrombolysis
E. Type 2 MI:
- Treat the underlying cause (correct anemia, control heart rate, treat hypotension)
-
- Symptom to Diagnosis, p. 175; Sabiston Textbook of Surgery, p. 2934-2936
15. Reperfusion Injury
- Restoring blood flow saves myocardium but can paradoxically cause additional injury.
- Mechanisms: calcium overload, oxidative stress from reactive oxygen species, inflammatory mediators.
- Stunned myocardium - Post-ischemic myocardium remains non-contractile for days despite restored flow; this is transient and reversible.
-
- Robbins & Kumar Basic Pathology, p. 354
16. Prognosis
- In-hospital mortality: ~10.3% in men, ~14.6% in women.
- Women have worse outcomes partly due to presentation without chest pain, leading to delayed diagnosis and less aggressive treatment.
- Mortality difference between sexes narrows and eventually reverses with advancing age.
- Cardiogenic shock (>40% LV infarction) carries 40-50% short-term mortality.
- Exercise stress testing is recommended within 3 weeks of MI (for patients not undergoing PCI/angiography) for risk stratification and functional assessment.
- A recent 2025 meta-analysis (PMID 39298680) found that beta-blocker benefit for secondary prevention post-MI may be limited in patients without reduced ejection fraction or heart failure, suggesting potential refinement of current guidelines. - Symptom to Diagnosis, p. 175
17. Special Considerations
Subendocardial oxygen demand:
- Cardiac muscle requires ~1.3 mL O₂/100g/min just to stay alive vs. ~8 mL O₂/100g/min delivered normally. Even 15-30% of normal resting flow can prevent cell death in marginal zones. The central infarct with near-zero flow is what undergoes irreversible necrosis. - Guyton & Hall Textbook of Medical Physiology, p. 271
Post-surgical MI:
- In the perioperative setting, the critical distinction between Type 1 (plaque rupture - needs revascularization) and Type 2 (demand ischemia - needs oxygen demand reduction) is essential because anticoagulation for PCI may be contraindicated after recent neurosurgery or major procedures. - Sabiston Textbook of Surgery, p. 2932
Cocaine-induced MI:
- Causes vasospasm and microscopic infarcts even in young patients without atherosclerosis - Robbins & Kumar Basic Pathology, p. 356
Sources: Robbins & Kumar Basic Pathology; Guyton & Hall Textbook of Medical Physiology; Ganong's Review of Medical Physiology; Sabiston Textbook of Surgery; Symptom to Diagnosis, 4th Edition; Tietz Textbook of Laboratory Medicine, 7th Edition
Generate a PDF quick reference guide on MI diagnosis and treatment
Reading File
Reading File
Running Command
ls /home/daytona/workspace/ 2>/dev/null || echo "workspace empty or not found"
Writing File
~/mi-quickref/generate_mi_pdf.py
from reportlab.lib.pagesizes import A4
from reportlab.lib import colors
from reportlab.lib.units import mm, cm
from reportlab.lib.styles import getSampleStyleSheet, ParagraphStyle
from reportlab.lib.enums import TA_CENTER, TA_LEFT, TA_JUSTIFY
from reportlab.platypus import (
SimpleDocTemplate, Paragraph, Spacer, Table, TableStyle,
HRFlowable, KeepTogether
)
from reportlab.platypus.flowables import HRFlowable
import os
OUTPUT_PATH = "/home/daytona/workspace/mi-quickref/MI_Quick_Reference_Guide.pdf"
os.makedirs(os.path.dirname(OUTPUT_PATH), exist_ok=True)
# ── Colour palette ──────────────────────────────────────────────────────────
RED = colors.HexColor("#C0392B")
DARK_RED = colors.HexColor("#922B21")
ORANGE = colors.HexColor("#E67E22")
TEAL = colors.HexColor("#1A6B7C")
TEAL_LIGHT= colors.HexColor("#D6EEF3")
GREY_BG = colors.HexColor("#F4F6F7")
GREY_LINE = colors.HexColor("#BDC3C7")
WHITE = colors.white
BLACK = colors.HexColor("#1C2833")
GREEN = colors.HexColor("#1E8449")
GREEN_LIGHT= colors.HexColor("#D5F5E3")
AMBER = colors.HexColor("#D68910")
AMBER_LIGHT= colors.HexColor("#FEF9E7")
BLUE_HEAD = colors.HexColor("#1B4F72")
# ── Styles ───────────────────────────────────────────────────────────────────
styles = getSampleStyleSheet()
def S(name, **kw):
return ParagraphStyle(name, **kw)
Title = S("Title",
fontName="Helvetica-Bold", fontSize=22, textColor=WHITE,
leading=28, alignment=TA_CENTER, spaceAfter=2)
Subtitle = S("Subtitle",
fontName="Helvetica", fontSize=11, textColor=colors.HexColor("#FDFEFE"),
leading=16, alignment=TA_CENTER)
SectionHead = S("SectionHead",
fontName="Helvetica-Bold", fontSize=11, textColor=WHITE,
leading=15, spaceBefore=6, spaceAfter=3,
leftIndent=6, rightIndent=6)
SubHead = S("SubHead",
fontName="Helvetica-Bold", fontSize=9.5, textColor=BLUE_HEAD,
leading=13, spaceBefore=5, spaceAfter=2)
Body = S("Body",
fontName="Helvetica", fontSize=8.5, textColor=BLACK,
leading=12, spaceAfter=2)
BulletStyle = S("Bullet",
fontName="Helvetica", fontSize=8.5, textColor=BLACK,
leading=12, leftIndent=12, firstLineIndent=-8, spaceAfter=1)
BoldBody = S("BoldBody",
fontName="Helvetica-Bold", fontSize=8.5, textColor=BLACK,
leading=12, spaceAfter=2)
SmallGrey = S("SmallGrey",
fontName="Helvetica-Oblique", fontSize=7.5, textColor=colors.HexColor("#7F8C8D"),
leading=10, alignment=TA_CENTER)
CellHead = S("CellHead",
fontName="Helvetica-Bold", fontSize=8.5, textColor=WHITE,
leading=11, alignment=TA_CENTER)
CellBody = S("CellBody",
fontName="Helvetica", fontSize=8, textColor=BLACK, leading=11)
CellBold = S("CellBold",
fontName="Helvetica-Bold", fontSize=8, textColor=BLACK, leading=11)
AlertRed = S("AlertRed",
fontName="Helvetica-Bold", fontSize=9, textColor=RED,
leading=13, spaceAfter=2)
def bullet(text, bold_prefix=None):
if bold_prefix:
return Paragraph(f'<bullet>\u2022</bullet> <b>{bold_prefix}</b> {text}', BulletStyle)
return Paragraph(f'<bullet>\u2022</bullet> {text}', BulletStyle)
def section_bar(text, bg=TEAL):
data = [[Paragraph(text, SectionHead)]]
t = Table(data, colWidths=[175*mm])
t.setStyle(TableStyle([
('BACKGROUND', (0,0), (-1,-1), bg),
('TOPPADDING', (0,0), (-1,-1), 5),
('BOTTOMPADDING', (0,0), (-1,-1), 5),
('LEFTPADDING', (0,0), (-1,-1), 8),
('RIGHTPADDING', (0,0), (-1,-1), 8),
('ROUNDEDCORNERS', [4, 4, 4, 4]),
]))
return t
def hr(color=GREY_LINE, thickness=0.5):
return HRFlowable(width="100%", thickness=thickness, color=color, spaceAfter=3, spaceBefore=3)
# ── Document setup ────────────────────────────────────────────────────────────
doc = SimpleDocTemplate(
OUTPUT_PATH,
pagesize=A4,
leftMargin=15*mm, rightMargin=15*mm,
topMargin=12*mm, bottomMargin=12*mm,
title="MI Quick Reference Guide",
author="Orris Medical Reference",
subject="Myocardial Infarction – Diagnosis & Treatment"
)
story = []
W = 175*mm # usable width
# ═══════════════════════════════════════════════════════════════════════════
# HEADER BANNER
# ═══════════════════════════════════════════════════════════════════════════
header_data = [[
Paragraph("MYOCARDIAL INFARCTION", Title),
Paragraph("Quick Reference Guide | Diagnosis & Treatment", Subtitle),
Paragraph("Based on Braunwald's, Robbins, Harrison's, Guyton & Hall", SmallGrey)
]]
header = Table([[
Paragraph("MYOCARDIAL INFARCTION", Title)
], [
Paragraph("Quick Reference Guide \u2022 Diagnosis & Treatment", Subtitle)
], [
Paragraph("Braunwald's \u2022 Robbins \u2022 Harrison's \u2022 Guyton & Hall \u2022 Sabiston", SmallGrey)
]], colWidths=[W])
header.setStyle(TableStyle([
('BACKGROUND', (0,0), (-1,-1), RED),
('TOPPADDING', (0,0), (-1,-1), 10),
('BOTTOMPADDING', (0,0), (-1,-1), 10),
('LEFTPADDING', (0,0), (-1,-1), 10),
('RIGHTPADDING', (0,0), (-1,-1), 10),
('ROUNDEDCORNERS', [6, 6, 6, 6]),
]))
story.append(header)
story.append(Spacer(1, 6))
# ═══════════════════════════════════════════════════════════════════════════
# ROW 1: DEFINITION + CLASSIFICATION (2 columns)
# ═══════════════════════════════════════════════════════════════════════════
def box(content_rows, bg=GREY_BG, width=None):
t = Table([[c] for c in content_rows], colWidths=[width or 84*mm])
t.setStyle(TableStyle([
('BACKGROUND', (0,0), (-1,-1), bg),
('TOPPADDING', (0,0), (-1,-1), 5),
('BOTTOMPADDING', (0,0), (-1,-1), 5),
('LEFTPADDING', (0,0), (-1,-1), 7),
('RIGHTPADDING', (0,0), (-1,-1), 7),
('BOX', (0,0), (-1,-1), 0.5, GREY_LINE),
('ROUNDEDCORNERS', [4, 4, 4, 4]),
]))
return t
col_w = 84*mm
gap = 7*mm
# ── DEFINITION box ──────────────────────────────────────────────────────────
def_content = [
section_bar("DEFINITION", DARK_RED),
Spacer(1, 4),
Paragraph("Necrosis of heart muscle from sustained ischemia.", Body),
Paragraph('<b>2018 Universal Definition:</b> "Acute myocardial injury detected by abnormal cardiac biomarkers in the setting of evidence of acute myocardial ischemia."', Body),
hr(),
Paragraph("<b>Key time thresholds:</b>", BoldBody),
bullet("<b>Seconds:</b> Aerobic metabolism ceases; ATP falls"),
bullet("<b>Minutes:</b> Loss of contractility (reversible)"),
bullet("<b>20-40 min:</b> Irreversible cell death begins"),
bullet("<b>3-6 hrs:</b> Full transmural infarct if untreated"),
]
# ── CLASSIFICATION box ───────────────────────────────────────────────────────
class_content = [
section_bar("CLASSIFICATION", TEAL),
Spacer(1, 4),
Paragraph("<b>Type 1 MI</b> – Plaque rupture / thrombosis", BoldBody),
bullet("STEMI: ST elevation + biomarker rise"),
bullet("NSTEMI: No ST elevation; biomarker rise"),
bullet("UA: Ischemia symptoms; no biomarker rise"),
hr(),
Paragraph("<b>Type 2 MI</b> – Supply/demand mismatch", BoldBody),
bullet("Tachycardia, anemia, hypotension, hypertension"),
bullet("Treatment: reduce cardiac O<sub rise='2'>2</sub> demand"),
hr(),
Paragraph("<b>ACS Spectrum:</b> STEMI > NSTEMI > Unstable Angina", Body),
]
row1 = Table([[
Table([[c] for c in def_content], colWidths=[col_w]),
Spacer(gap, 1),
Table([[c] for c in class_content], colWidths=[col_w]),
]], colWidths=[col_w, gap, col_w])
row1.setStyle(TableStyle([
('VALIGN', (0,0), (-1,-1), 'TOP'),
('LEFTPADDING', (0,0), (-1,-1), 0),
('RIGHTPADDING', (0,0), (-1,-1), 0),
('TOPPADDING', (0,0), (-1,-1), 0),
('BOTTOMPADDING', (0,0), (-1,-1), 0),
]))
story.append(row1)
story.append(Spacer(1, 5))
# ═══════════════════════════════════════════════════════════════════════════
# SYMPTOMS & ECG (2 columns)
# ═══════════════════════════════════════════════════════════════════════════
symp_content = [
section_bar("SYMPTOMS", colors.HexColor("#6C3483")),
Spacer(1, 4),
Paragraph("<b>Classic (Type 1):</b>", BoldBody),
bullet("Central crushing/squeezing chest pain >30 min"),
bullet("Radiation: left arm, jaw, neck, back, epigastrium"),
bullet("Diaphoresis, nausea/vomiting, dyspnea"),
bullet("Anxiety, sense of impending doom"),
hr(),
Paragraph("<b>Atypical</b> (women, elderly, diabetics):", BoldBody),
bullet("Epigastric pain or indigestion"),
bullet("Fatigue, jaw or arm pain alone"),
bullet("Silent MI (no pain) – ECG/biomarkers only"),
Paragraph('<font color="#C0392B"><b>! Women presenting without chest pain receive delayed care – higher in-hospital mortality (14.6% vs 10.3%)</b></font>', Body),
]
ecg_content = [
section_bar("ECG CHANGES", colors.HexColor("#1A5276")),
Spacer(1, 4),
Paragraph("<b>Hyperacute (minutes):</b>", BoldBody),
bullet("Tall, peaked T waves"),
Paragraph("<b>Acute STEMI:</b>", BoldBody),
bullet("ST elevation in leads over infarct"),
bullet("Reciprocal ST depression in opposite leads"),
Paragraph("<b>Hours to days:</b>", BoldBody),
bullet("T-wave inversion"),
bullet("Q waves appear (electrically silent necrosis)"),
Paragraph("<b>NSTEMI / UA:</b>", BoldBody),
bullet("ST depression or T-wave changes"),
bullet("No ST elevation; no Q waves"),
hr(),
Paragraph("<b>Lead localisation:</b>", BoldBody),
bullet("V1-V4: Anterior (LAD)"),
bullet("II, III, aVF: Inferior (RCA)"),
bullet("I, aVL, V5-V6: Lateral (LCX)"),
]
row2 = Table([[
Table([[c] for c in symp_content], colWidths=[col_w]),
Spacer(gap, 1),
Table([[c] for c in ecg_content], colWidths=[col_w]),
]], colWidths=[col_w, gap, col_w])
row2.setStyle(TableStyle([
('VALIGN', (0,0), (-1,-1), 'TOP'),
('LEFTPADDING', (0,0), (-1,-1), 0),
('RIGHTPADDING', (0,0), (-1,-1), 0),
('TOPPADDING', (0,0), (-1,-1), 0),
('BOTTOMPADDING', (0,0), (-1,-1), 0),
]))
story.append(row2)
story.append(Spacer(1, 5))
# ═══════════════════════════════════════════════════════════════════════════
# BIOMARKERS TABLE (full width)
# ═══════════════════════════════════════════════════════════════════════════
story.append(section_bar("CARDIAC BIOMARKERS", colors.HexColor("#784212")))
story.append(Spacer(1, 3))
bio_head = [
Paragraph("Marker", CellHead),
Paragraph("Rises", CellHead),
Paragraph("Peaks", CellHead),
Paragraph("Returns to Normal", CellHead),
Paragraph("Notes", CellHead),
]
bio_data = [
["Troponin I / T", "3-6 hrs", "12-24 hrs", "7-14 days (TnT up to 2 wks)", "Most specific & sensitive. Gold standard."],
["CK-MB", "3-6 hrs", "18-24 hrs", "48-72 hrs", "Useful for reinfarction detection"],
["Myoglobin", "1-3 hrs", "6-9 hrs", "24 hrs", "Earliest; not cardiac-specific. Rule-out only."],
["LDH", "24-48 hrs", "3-6 days", "8-14 days", "Historical; largely replaced by troponins"],
]
bio_rows = [bio_head] + [[Paragraph(c, CellBody) for c in row] for row in bio_data]
bio_col = [28*mm, 18*mm, 18*mm, 45*mm, 66*mm]
bio_table = Table(bio_rows, colWidths=bio_col, repeatRows=1)
bio_table.setStyle(TableStyle([
('BACKGROUND', (0,0), (-1,0), colors.HexColor("#784212")),
('BACKGROUND', (0,1), (-1,1), GREY_BG),
('BACKGROUND', (0,2), (-1,2), WHITE),
('BACKGROUND', (0,3), (-1,3), GREY_BG),
('BACKGROUND', (0,4), (-1,4), WHITE),
('GRID', (0,0), (-1,-1), 0.4, GREY_LINE),
('TOPPADDING', (0,0), (-1,-1), 4),
('BOTTOMPADDING', (0,0), (-1,-1), 4),
('LEFTPADDING', (0,0), (-1,-1), 5),
('RIGHTPADDING', (0,0), (-1,-1), 5),
('VALIGN', (0,0), (-1,-1), 'MIDDLE'),
]))
story.append(bio_table)
story.append(Spacer(1, 5))
# ═══════════════════════════════════════════════════════════════════════════
# INFARCT LOCATION TABLE (full width)
# ═══════════════════════════════════════════════════════════════════════════
story.append(section_bar("INFARCT LOCATION BY VESSEL", colors.HexColor("#1A6B7C")))
story.append(Spacer(1, 3))
loc_head = [
Paragraph("Artery", CellHead),
Paragraph("% of MIs", CellHead),
Paragraph("Territory Affected", CellHead),
Paragraph("ECG Leads", CellHead),
]
loc_data = [
["Left Anterior Descending (LAD)", "40-50%", "Anterior LV wall, anterior 2/3 septum, cardiac apex", "V1-V4"],
["Right Coronary Artery (RCA)", "30-40%", "Right ventricle, posterior LV wall, posterior 1/3 septum", "II, III, aVF"],
["Left Circumflex (LCX)", "15-20%", "Lateral left ventricle", "I, aVL, V5-V6"],
]
loc_rows = [loc_head] + [[Paragraph(c, CellBody) for c in row] for row in loc_data]
loc_col = [50*mm, 22*mm, 73*mm, 30*mm]
loc_table = Table(loc_rows, colWidths=loc_col, repeatRows=1)
loc_table.setStyle(TableStyle([
('BACKGROUND', (0,0), (-1,0), TEAL),
('BACKGROUND', (0,1), (-1,1), TEAL_LIGHT),
('BACKGROUND', (0,2), (-1,2), WHITE),
('BACKGROUND', (0,3), (-1,3), TEAL_LIGHT),
('GRID', (0,0), (-1,-1), 0.4, GREY_LINE),
('TOPPADDING', (0,0), (-1,-1), 4),
('BOTTOMPADDING', (0,0), (-1,-1), 4),
('LEFTPADDING', (0,0), (-1,-1), 5),
('RIGHTPADDING', (0,0), (-1,-1), 5),
('VALIGN', (0,0), (-1,-1), 'MIDDLE'),
]))
story.append(loc_table)
story.append(Spacer(1, 5))
# ═══════════════════════════════════════════════════════════════════════════
# TREATMENT (2 columns: Acute Meds | Reperfusion)
# ═══════════════════════════════════════════════════════════════════════════
med_content = [
section_bar("ACUTE MEDICATIONS", RED),
Spacer(1, 4),
Paragraph("<b>Antiplatelet:</b>", BoldBody),
bullet("Aspirin 300 mg loading (immediate)"),
bullet("P2Y12 inhibitor: clopidogrel / ticagrelor / prasugrel"),
bullet("GP IIb/IIIa inhibitor (if PCI performed)"),
Paragraph("<b>Anticoagulation:</b>", BoldBody),
bullet("UFH, LMWH, fondaparinux, or bivalirudin"),
Paragraph("<b>Nitrates:</b>", BoldBody),
bullet("Sublingual or IV nitroglycerin"),
Paragraph('<font color="#C0392B"><b>! Avoid nitrates in RV infarction – reduces preload causing catastrophic hypotension</b></font>', Body),
Paragraph("<b>Beta-blockers:</b>", BoldBody),
bullet("Cardioprotective; reduce O2 demand + arrhythmia risk"),
Paragraph('<font color="#C0392B"><b>! Avoid if: hypotension, low EF, bradycardia, cardiogenic shock</b></font>', Body),
Paragraph("<b>Statins:</b>", BoldBody),
bullet("High-intensity (target LDL <70 mg/dL); start early"),
Paragraph("<b>ACE Inhibitors:</b>", BoldBody),
bullet("Reduce ventricular remodeling; start within 24 hrs"),
Paragraph("<b>Oxygen:</b>", BoldBody),
bullet("Only if SpO2 <90% (hyperoxia is harmful)"),
Paragraph("<b>Morphine:</b>", BoldBody),
bullet("Pain unrelieved by nitrates (routine use now questioned)"),
]
reperf_content = [
section_bar("REPERFUSION STRATEGY", GREEN),
Spacer(1, 4),
Paragraph('<b><font color="#1E8449">Primary PCI</font></b> – Gold Standard', BoldBody),
bullet("Percutaneous coronary intervention + stent"),
bullet("Lower mortality than thrombolysis"),
bullet("Lower hemorrhagic stroke risk"),
bullet("<b>Target: <90 min door-to-balloon time</b>"),
bullet("Effective up to 12 hrs from symptom onset"),
hr(),
Paragraph('<b><font color="#D68910">Thrombolysis</font></b> – If PCI unavailable within 2 hrs', BoldBody),
bullet("tPA (alteplase), streptokinase, tenecteplase"),
bullet("Most effective within 12 hrs of symptom onset"),
bullet("Higher bleeding/stroke risk than PCI"),
bullet("Contraindicated: recent surgery, stroke, active bleeding"),
hr(),
Paragraph("<b>NSTEMI:</b>", BoldBody),
bullet("PCI can be delayed up to 72 hrs in stable patients"),
bullet("No systemic thrombolysis"),
hr(),
Paragraph("<b>Post-Reperfusion (long-term):</b>", BoldBody),
bullet("Beta-blockers + ACE inhibitors + Aspirin"),
bullet("P2Y12 inhibitor (duration per stent/bleeding risk)"),
bullet("High-intensity statin"),
bullet("Exercise test 3 wks post-MI (if no angio/PCI)"),
]
row3 = Table([[
Table([[c] for c in med_content], colWidths=[col_w]),
Spacer(gap, 1),
Table([[c] for c in reperf_content], colWidths=[col_w]),
]], colWidths=[col_w, gap, col_w])
row3.setStyle(TableStyle([
('VALIGN', (0,0), (-1,-1), 'TOP'),
('LEFTPADDING', (0,0), (-1,-1), 0),
('RIGHTPADDING', (0,0), (-1,-1), 0),
('TOPPADDING', (0,0), (-1,-1), 0),
('BOTTOMPADDING', (0,0), (-1,-1), 0),
]))
story.append(row3)
story.append(Spacer(1, 5))
# ═══════════════════════════════════════════════════════════════════════════
# COMPLICATIONS (full width, 2-col layout inside table)
# ═══════════════════════════════════════════════════════════════════════════
story.append(section_bar("COMPLICATIONS", colors.HexColor("#6E2F12")))
story.append(Spacer(1, 3))
comp_early = [
Paragraph("<b>Early (hours - days):</b>", BoldBody),
bullet("Ventricular fibrillation / tachycardia"),
bullet("Cardiogenic shock (>40% LV involved; mortality 40-50%)"),
bullet("Acute LV failure / pulmonary oedema"),
bullet("Heart block / bradyarrhythmia (inferior MI - RCA)"),
bullet("RV infarction: low output + clear lungs + JVD"),
bullet("Early pericarditis (24-72 hrs; overlying infarct)"),
]
comp_late = [
Paragraph("<b>Subacute / Late (days - weeks):</b>", BoldBody),
bullet("Papillary muscle rupture - acute mitral regurgitation"),
bullet("VSD from septal rupture (new pansystolic murmur)"),
bullet("Free wall rupture - cardiac tamponade (days 3-7)"),
bullet("Mural thrombus - systemic embolism"),
bullet("LV aneurysm (weeks to months)"),
bullet("Dressler's syndrome: autoimmune pericarditis (2-10 wks)"),
bullet("Chronic heart failure"),
]
comp_table = Table([[
Table([[c] for c in comp_early], colWidths=[col_w]),
Spacer(gap, 1),
Table([[c] for c in comp_late], colWidths=[col_w]),
]], colWidths=[col_w, gap, col_w])
comp_table.setStyle(TableStyle([
('VALIGN', (0,0), (-1,-1), 'TOP'),
('LEFTPADDING', (0,0), (-1,-1), 0),
('RIGHTPADDING', (0,0), (-1,-1), 0),
('TOPPADDING', (0,0), (-1,-1), 0),
('BOTTOMPADDING', (0,0), (-1,-1), 0),
]))
story.append(comp_table)
story.append(Spacer(1, 5))
# ═══════════════════════════════════════════════════════════════════════════
# MORPHOLOGY TIMELINE (condensed table)
# ═══════════════════════════════════════════════════════════════════════════
story.append(section_bar("MORPHOLOGICAL TIMELINE OF MI (Robbins Pathology)", colors.HexColor("#4A235A")))
story.append(Spacer(1, 3))
morph_head = [
Paragraph("Time", CellHead),
Paragraph("Gross Features", CellHead),
Paragraph("Microscopy", CellHead),
]
morph_data = [
["0-4 hrs", "None visible", "Waviness of fibers at border; sarcolemmal disruption on EM"],
["4-24 hrs", "Dark mottling", "Coagulation necrosis; pyknotic nuclei; hypereosinophilic myocytes; neutrophil infiltrate"],
["1-3 days", "Yellow-tan center", "Necrosis with loss of nuclei/striations; heavy neutrophil infiltrate"],
["3-10 days", "Hyperemic border; yellow-tan soft center", "Neutrophil disintegration; macrophage phagocytosis; early granulation tissue"],
["10 days - 8 wks", "Red-gray depressed borders; grey-white scar forming", "Progressive collagen deposition; granulation tissue replaced by scar"],
[">2 months", "Dense white scar", "Dense collagen scar - fully healed (no regeneration)"],
]
morph_rows = [morph_head] + [[Paragraph(c, CellBody) for c in row] for row in morph_data]
morph_col = [28*mm, 45*mm, 102*mm]
morph_table = Table(morph_rows, colWidths=morph_col, repeatRows=1)
row_colors = [colors.HexColor("#4A235A"), GREY_BG, WHITE, GREY_BG, WHITE, GREY_BG, WHITE]
morph_style = [
('BACKGROUND', (0,0), (-1,0), colors.HexColor("#4A235A")),
('GRID', (0,0), (-1,-1), 0.4, GREY_LINE),
('TOPPADDING', (0,0), (-1,-1), 3),
('BOTTOMPADDING', (0,0), (-1,-1), 3),
('LEFTPADDING', (0,0), (-1,-1), 5),
('RIGHTPADDING', (0,0), (-1,-1), 5),
('VALIGN', (0,0), (-1,-1), 'TOP'),
]
for i, c in enumerate(row_colors[1:], 1):
morph_style.append(('BACKGROUND', (0,i), (-1,i), c))
morph_table.setStyle(TableStyle(morph_style))
story.append(morph_table)
story.append(Spacer(1, 5))
# ═══════════════════════════════════════════════════════════════════════════
# FOOTER
# ═══════════════════════════════════════════════════════════════════════════
footer_data = [[
Paragraph(
"Sources: Robbins & Kumar Basic Pathology | Braunwald's Heart Disease | Guyton & Hall Medical Physiology | "
"Ganong's Review of Medical Physiology | Sabiston Textbook of Surgery | Symptom to Diagnosis (4th Ed) | "
"Tietz Textbook of Laboratory Medicine | Harrison's Principles of Internal Medicine",
SmallGrey
)
]]
footer = Table(footer_data, colWidths=[W])
footer.setStyle(TableStyle([
('BACKGROUND', (0,0), (-1,-1), colors.HexColor("#EAECEE")),
('TOPPADDING', (0,0), (-1,-1), 5),
('BOTTOMPADDING', (0,0), (-1,-1), 5),
('LEFTPADDING', (0,0), (-1,-1), 8),
('RIGHTPADDING', (0,0), (-1,-1), 8),
('BOX', (0,0), (-1,-1), 0.5, GREY_LINE),
]))
story.append(footer)
# ── Build ─────────────────────────────────────────────────────────────────
doc.build(story)
print(f"PDF created: {OUTPUT_PATH}")
Running Command
cd /home/daytona/workspace/mi-quickref && python generate_mi_pdf.py 2>&1
Running Command
ls -lh /home/daytona/workspace/mi-quickref/MI_Quick_Reference_Guide.pdf
Running Command
cd /home/daytona/workspace/mi-quickref && python -c " from pypdf import PdfReade…
Running Command
cd /home/daytona/workspace/mi-quickref && python -c " from pypdf import PdfReade…
Your MI Quick Reference Guide PDF is ready:
MI Quick Reference Guide
PDF Document · PDF
What's inside (3 pages, A4):
| Section | Content |
|---|---|
| Header | Red title banner with source attribution |
| Definition & Classification | 2018 Universal Definition, key time thresholds, Type 1 vs Type 2 MI, ACS spectrum |
| Symptoms & ECG Changes | Classic vs atypical presentation, ECG evolution (hyperacute → acute → chronic), lead localisation table |
| Cardiac Biomarkers | Colour-coded table: Troponin I/T, CK-MB, Myoglobin, LDH - with rise/peak/normalisation times |
| Infarct Location | LAD / RCA / LCX with % frequency, territory, and ECG leads |
| Acute Medications | Antiplatelet, anticoagulation, nitrates, beta-blockers, statins, ACE inhibitors, oxygen - with red warning boxes for nitrates in RV infarction and beta-blocker contraindications |
| Reperfusion Strategy | Primary PCI vs thrombolysis decision guide, door-to-balloon target, NSTEMI approach, post-reperfusion secondary prevention |
| Complications | Early (VF, cardiogenic shock, pulmonary oedema) and late (papillary rupture, VSD, free wall rupture, Dressler's) |
| Morphological Timeline | Robbins-based table from 0 hrs to >2 months |
| Footer | Full source list from 8 authoritative textbooks |
This is a shared conversation. Sign in to Orris to start your own chat.