Hypertension management of 133/88mm hg of 35 year old male
Reading File
Finding Sources
Searching PubMed
"hypertension" AND "stage 1" AND "lifestyle" AND "treatment"
Searching the Web
ACC AHA 2024 hypertension guidelines Stage 1 management young adults
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a thorough, evidence-based management plan for this patient.
Hypertension Management: 133/88 mmHg in a 35-Year-Old Male
Classification
By ACC/AHA 2017 guidelines (still the standard U.S. reference as of 2025):
- Stage 1 Hypertension: SBP 130-139 mmHg or DBP 80-89 mmHg
- This patient meets both criteria (133 systolic AND 88 diastolic)
Important: Confirm the reading is an average of 2+ readings on 2+ separate occasions. Rule out white-coat hypertension (consider ambulatory BP monitoring).
Step 1: Initial Assessment
Before any treatment decision, obtain:
| Test | Purpose |
|---|---|
| CBC, CMP (electrolytes, creatinine, eGFR) | Baseline, detect CKD |
| Fasting glucose / HbA1c | Rule out diabetes |
| Lipid panel | Calculate ASCVD risk |
| TSH | Rule out secondary (thyroid) cause |
| Urine albumin-to-creatinine ratio | Early kidney damage |
| 12-lead ECG | Left ventricular hypertrophy |
| Uric acid | If considering diuretics |
Screen for secondary causes (especially important in patients under 40):
- Primary aldosteronism (serum aldosterone/renin ratio)
- Renovascular hypertension (renal artery Doppler)
- Sleep apnea (STOP-BANG questionnaire) - 2024 ESC specifically recommends sleep apnea screening first in young obese adults
- Pheochromocytoma (24-hour urine metanephrines if symptomatic)
Step 2: CVD Risk Stratification (The Key Decision Point)
Calculate his 10-year ASCVD risk using the ACC/AHA Pooled Cohort Equations (PCE calculator). At 35 years old, the 10-year risk is often low, but lifetime risk can be substantial.
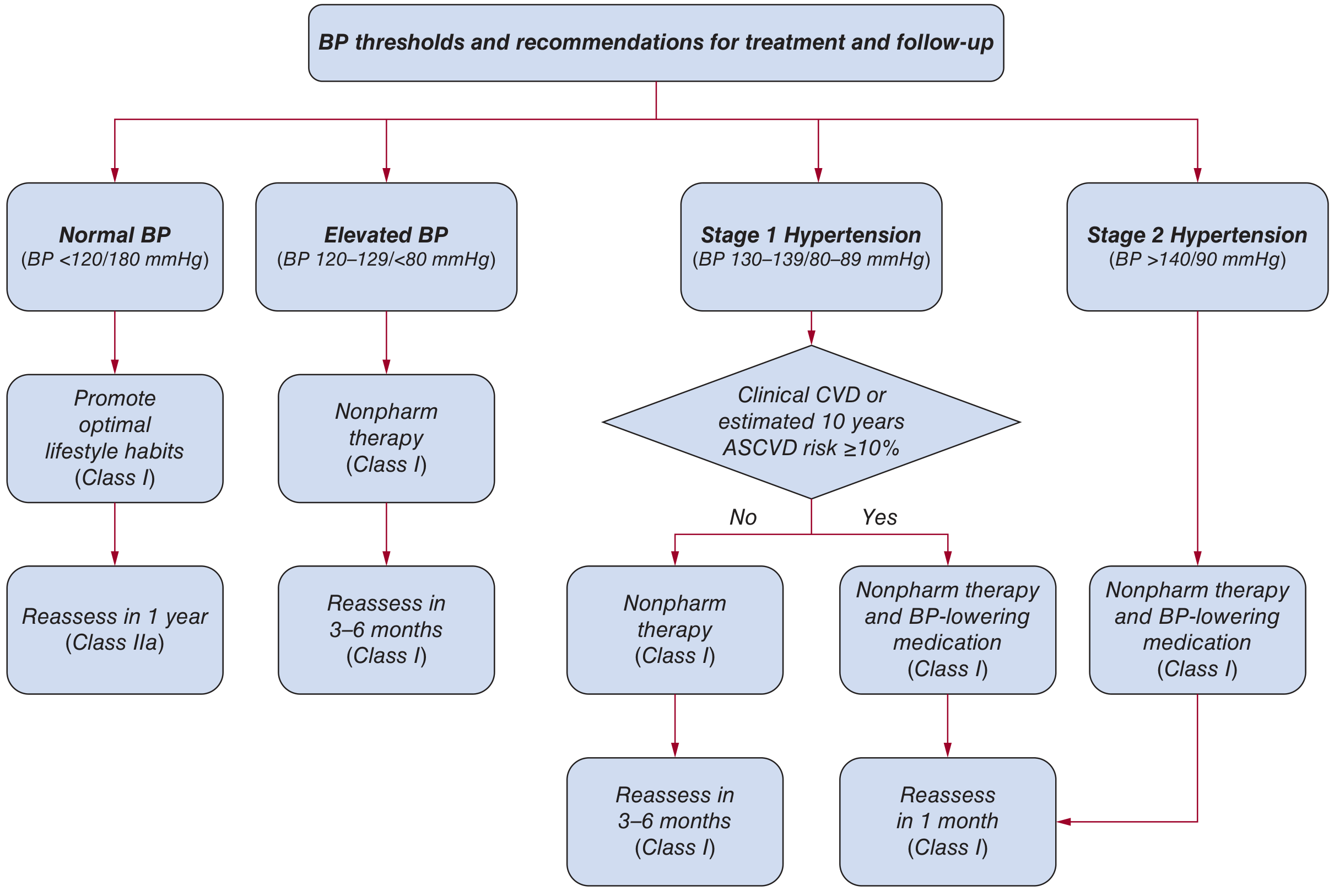
Two paths based on risk:
Path A - Low CVD Risk (10-year ASCVD < 10%, no DM, no CKD, no CVD history)
- Start with nonpharmacologic therapy alone
- Reassess in 3-6 months
- Add medication if BP remains ≥130/80 after 6 months of lifestyle changes (especially given his high lifetime risk as a young adult)
Path B - High CVD Risk (10-year ASCVD ≥ 10%, OR has DM/CKD/known CVD)
- Nonpharmacologic therapy + antihypertensive medication immediately
- Reassess in 1 month
Step 3: Lifestyle (Nonpharmacologic) Interventions
These are mandatory regardless of whether medications are started and can reduce SBP by 5-15+ mmHg when combined.
| Intervention | Goal | Expected SBP Reduction |
|---|---|---|
| Weight loss (if overweight/obese) | ~1 mmHg per 1 kg lost; target ideal BMI | -5 mmHg |
| DASH diet | Rich in fruits, vegetables, low-fat dairy, reduced saturated fat | -4 to 11 mmHg |
| Sodium restriction | Target <1500 mg/day; minimum reduction of 1000 mg/day | -5 to 6 mmHg |
| Increased potassium intake | >3400 mg/day via food (fruits, vegetables) | -4 to 5 mmHg |
| Aerobic exercise | 90-150 min/week at 65-75% heart rate reserve (brisk walking, swimming, cycling) | -5 to 7 mmHg |
| Limit alcohol | ≤2 standard drinks/day for men | -4 mmHg |
| Smoking cessation | Complete cessation | Cardiovascular risk reduction |
Combined interventions can achieve SBP reductions >10 mmHg - Harrison's Principles of Internal Medicine 22E, p. 2186
Step 4: Pharmacotherapy (if indicated)
When to Start Medications at This BP Level
- Immediately if high CVD risk, DM, CKD, established CVD, or target organ damage
- After 6 months of lifestyle trial if low-risk but BP still ≥130/80 mmHg
- At 35 years old, even with low 10-year risk, his high lifetime ASCVD risk is a valid argument for earlier pharmacotherapy
First-Line Drug Classes (choose based on comorbidities)
| Class | Examples | Key Notes |
|---|---|---|
| Thiazide-like diuretics | Chlorthalidone 12.5-25 mg/day; Indapamide | "Best in class" per meta-analyses for CVD prevention; preferred over HCTZ (longer half-life, better nighttime control) |
| ACE Inhibitors | Lisinopril 10-40 mg/day; Ramipril | Preferred if DM or proteinuria; dry cough in ~10-15% |
| ARBs | Losartan, Valsartan, Olmesartan | Use if ACEI cough; do NOT combine ACEI + ARB |
| Calcium channel blockers | Amlodipine 5-10 mg/day | Excellent for stroke prevention; good add-on agent |
Beta-blockers are NOT first-line for uncomplicated primary hypertension - they have been inferior to other classes (especially for stroke prevention) in head-to-head RCTs. Reserve for compelling indications (angina, post-MI, HFrEF, rate control).
Drug Selection Considerations for a 35-Year-Old Male
- Black race: Thiazide diuretics or CCBs preferred (ACEIs/ARBs are less effective as monotherapy in Black patients)
- Active/athletic: Avoid beta-blockers (reduce exercise capacity)
- Sexually active: Be aware thiazides and beta-blockers can cause sexual dysfunction
- Planning parenthood: Avoid ACEIs/ARBs (teratogenic - relevant if partner is or could become pregnant; counsel accordingly)
BP Target
- < 130/80 mmHg per ACC/AHA guidelines
Step 5: Follow-Up
| Scenario | Reassessment |
|---|---|
| Lifestyle only | 3-6 months |
| Started medication | 1 month |
| At target BP | Every 3-6 months ongoing |
At each visit: check BP in both arms (seated after 5 min rest), assess adherence, side effects, lifestyle progress, and repeat relevant labs (electrolytes, creatinine) after starting/adjusting medications.
Summary Decision Algorithm for This Patient
- Confirm hypertension with repeat measurements / ambulatory BP monitoring
- Order baseline labs + ECG
- Screen for secondary causes (he is <40 years old)
- Calculate 10-year ASCVD risk (PCE calculator)
- If low risk: Start lifestyle modifications, reassess in 3-6 months - add medication if not at target
- If high risk: Start lifestyle modifications + a thiazide, ACEI, ARB, or CCB simultaneously
- BP target: <130/80 mmHg
Sources: Harrison's Principles of Internal Medicine 22E (2025), p. 2186-2190; Fuster and Hurst's The Heart, 15th Ed., p. 248-249; 2024 ESC Guidelines (ACC.org); AHA Scientific Statement on Young Adult Hypertension
This is a shared conversation. Sign in to Orris to start your own chat.