Jugular veins are jugular veins, pressures are connected directly to the right atrium because why is an upward deflection in the jugular venous pressure, like for example, an A wave is forming because when the right atrium is contracting, contracting, the pressure is going into it's one, when the tricuspid is open, it will be going to the right ventricle and one backward pressure which is going into the neck veins and passing the A deflection. That's why in conditions where there is a problem with tricuspid then or the atrial contraction occurs before the tricuspid opens as in the case of AV dissociations as in maybe AV or block degree 3, there we have complete dissociation between atria and ventricles. Hence there will be cannon A waves because another closed tricuspid valve more back pressure happens and we have a large cannon shaped A waves. So this concept of JVP, why a deflection is coming and how we are measuring and where we are measuring and how are these jugular veins related to the atrium. So the JVP pressures are talking only about the right atrial pressures and the right atrium connecting to the jugular vein or it also happens in the left atrium.
Why JVP Reflects Only Right Atrial Pressure (Not Left)
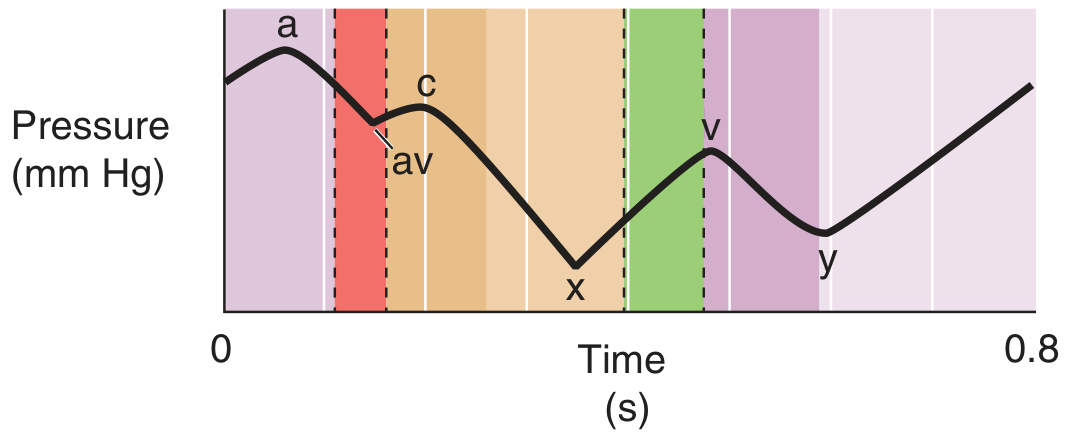
The JVP Waveform - Why Each Deflection Occurs
| Wave | Mechanism |
|---|---|
| a peak | Right atrial contraction - pressure is generated, pushes blood forward into RV (through open tricuspid), and backward into jugular veins |
| av trough | Right atrial relaxation + tricuspid valve closure |
| c peak | Early RV systole causes the tricuspid valve (now closed) to bulge back into the right atrium, causing a small pressure rise |
| x descent | RV contracts and shortens, pulling the tricuspid annulus downward - this physically elongates the atrium and veins, lowering their pressure |
| v peak | Venous return continues to fill the right atrium while the tricuspid is still closed during ventricular systole - pressure builds passively |
| y descent | Tricuspid valve opens - blood rushes from right atrium into right ventricle, RA pressure falls rapidly |
The A Wave in Detail - Your Question's Core
- Forward - through the open tricuspid valve into the right ventricle (the majority)
- Backward - up the superior vena cava into the jugular veins (this is what you see as the a wave)
How Measuring JVP Works
JVP (cmH₂O) = vertical height of jugular pulsation above the sternal angle + 5 cm
Cannon A Waves - Why They Occur
- Complete (3rd degree) AV block - complete dissociation of atria and ventricles means the atrium randomly contracts whenever it wants, sometimes right when the ventricle has just fired and the tricuspid is closed. These cannon waves are intermittent and irregular (because the dissociation is random).
- Junctional/ventricular tachycardia with retrograde P waves - here the atrium contracts at the same time as the ventricle every beat → cannon waves are regular.
- Ventricular pacing with AV dissociation
- Premature ventricular contractions (PVCs) causing occasional cannon waves
Tricuspid Stenosis - Giant "a" Waves (Different Mechanism)
Summary Table
| Situation | a wave | Mechanism |
|---|---|---|
| Normal | Normal upstroke | RA contracts, some pressure goes back into jugular |
| Tricuspid stenosis | Giant a wave | RA contracts hard against narrow valve |
| Complete AV block | Irregular cannon a waves | RA randomly contracts against closed tricuspid |
| VT or junctional tach | Regular cannon a waves | RA + RV contract simultaneously every beat |
| Atrial fibrillation | Absent a wave | No organized atrial contraction |
| Pulmonary hypertension | Large a wave | RV diastolic dysfunction requires forceful atrial kick |
Why JVP Reflects Only Right Atrial Pressure (Not Left) The internal jugular veins drain directly into the superior vena cava, which empties into the right atrium. There are no valves between the internal jugular vein and the right atrium. This means the right atrium's pressure changes are transmitted directly and freely backward into the jugular veins - they act as a simple fluid column connected to the right atrium. The left atrium has no such direct connection to any visible superficial vein. Its pressures are assessed indirectly via the pulmonary capillary wedge pressure (a catheterization technique), or by echocardiography. So yes - JVP = right atrial pressure only. (Fuster and Hurst's The Heart, 15th Ed.) this as any ultra ultra short note
have a one small ultra short yield and I mean ultra short and high yield line stating that an increase in intrathoracic pressure as in this Valsalva maneuver or continuous positive airway ventilation will have a decrease in venous rhythm. And if you see on the other hand, for normal inspiration, we're gonna decrease the intrathoracic pressure because it's becoming more negative. So venous return will increase and hence P2 closure is delayed. That's the reason why the pulmonary valve usually closes a bit late. So that is the physiological splitting of S2 is more pronounced in case of inspiration.
This is hypertensive cardiomyopathy or hypertensive obstructive cardiomyopathy and HCM or HOCM both same
-
HCM / HOCM = Hypertrophic (Obstructive) Cardiomyopathy - genetic (sarcomere mutation), asymmetric septal hypertrophy, young patients, family history.
-
Hypertensive Cardiomyopathy = heart muscle thickening secondary to chronic high blood pressure - concentric LV hypertrophy, older patients, known hypertension.
Can you give me some nice memories that I can remember forever? On that pressure overload is nothing but left ventricular hypertrophy, which is concentric hypertrophy, and if it's volume overload, it's eccentric hypertrophy. Then it's eccentric hypertrophy.