Clotting factors in detail for 20 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
Reading File
Finding Sources
Finding Sources
Searching PubMed
"coagulation cascade" AND "clotting factors" AND "recent advances"
Finding Sources
Finding Sources
Searching PubMed
"coagulation" AND "cell based model" AND hemostasis
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Searching the Web
clotting factors coagulation RGUHS ENT otolaryngology 20 marks question answer
Loading Image
Loading Image
Finding Sources
Loading Image
Finding Sources
Searching PubMed
"tissue factor pathway" AND coagulation AND hemostasis
CLOTTING FACTORS - Detailed Answer (20 Marks)
RGUHS Standard | Sources: Robbins Pathology, Basic Medical Biochemistry, Harrison's, Scott-Brown's, Cummings Otolaryngology, with Recent Advances
1. INTRODUCTION
Hemostasis is the process by which bleeding from injured blood vessels is arrested. It is maintained through a tightly coordinated interplay between the vascular wall, platelets, and the plasma coagulation factors. The coagulation cascade is a series of amplifying enzymatic reactions that culminate in the deposition of an insoluble fibrin clot.
In ENT surgery, disorders of hemostasis are clinically important in procedures such as tonsillectomy, adenoidectomy, septoplasty, FESS, and neck dissection. Understanding clotting factors is therefore essential for the ENT surgeon.
(References: Scott-Brown's Otorhinolaryngology Head & Neck Surgery; Cummings Otolaryngology Head and Neck Surgery; Dhingra's Diseases of Ear, Nose and Throat; Hazarika - ENT Surgery; Stell and Maran's Head & Neck Surgery)
2. OVERVIEW OF HEMOSTASIS
Hemostasis occurs in three overlapping phases:
VASCULAR INJURY
|
v
PRIMARY HEMOSTASIS
(Vasoconstriction + Platelet plug)
|
v
SECONDARY HEMOSTASIS
(Coagulation cascade -> Fibrin clot)
|
v
FIBRINOLYSIS
(Plasmin -> Clot dissolution)
3. CLOTTING FACTORS - COMPLETE LIST
| Factor | Name | Function / Active Form | Site of Synthesis |
|---|---|---|---|
| I | Fibrinogen | Converted to Fibrin (structural) | Liver |
| II | Prothrombin | Serine protease (Thrombin) | Liver (Vit K dependent) |
| III | Tissue Factor (Thromboplastin) | Receptor and cofactor for VIIa | Subendothelial cells |
| IV | Calcium (Ca²+) | Essential cofactor in multiple steps | Dietary/bone |
| V | Proaccelerin / Labile factor | Cofactor in prothrombinase complex | Liver + platelets |
| VI | Not assigned (= Va, obsolete) | - | - |
| VII | Proconvertin | Serine protease (extrinsic) | Liver (Vit K dependent) |
| VIII | Antihemophilic factor A | Cofactor in tenase complex | Liver + endothelium |
| IX | Christmas factor / AHF-B | Serine protease (intrinsic tenase) | Liver (Vit K dependent) |
| X | Stuart-Prower factor | Serine protease (prothrombinase) | Liver (Vit K dependent) |
| XI | Plasma thromboplastin antecedent | Serine protease (contact/intrinsic) | Liver |
| XII | Hageman factor | Serine protease (contact activation) | Liver |
| XIII | Fibrin-stabilizing factor | Ca²+-dependent transglutaminase | Liver + platelets |
| - | von Willebrand factor (vWF) | Platelet adhesion + carrier for VIII | Endothelium |
| - | Protein C | Anticoagulant serine protease | Liver (Vit K dependent) |
| - | Protein S | Cofactor for activated Protein C | Liver (Vit K dependent) |
| - | TFPI | Inhibits TF-VIIa-Xa complex | Endothelium |
| - | Antithrombin III | Inhibits thrombin, Xa, IXa | Liver |
(Sources: Basic Medical Biochemistry - A Clinical Approach, 6e, Table 43.2; Robbins Pathologic Basis of Disease; Harrison's Principles of Internal Medicine 22E)
4. THE COAGULATION CASCADE
DIAGRAM 1 - Classic Two-Pathway Model (Laboratory & In Vivo)
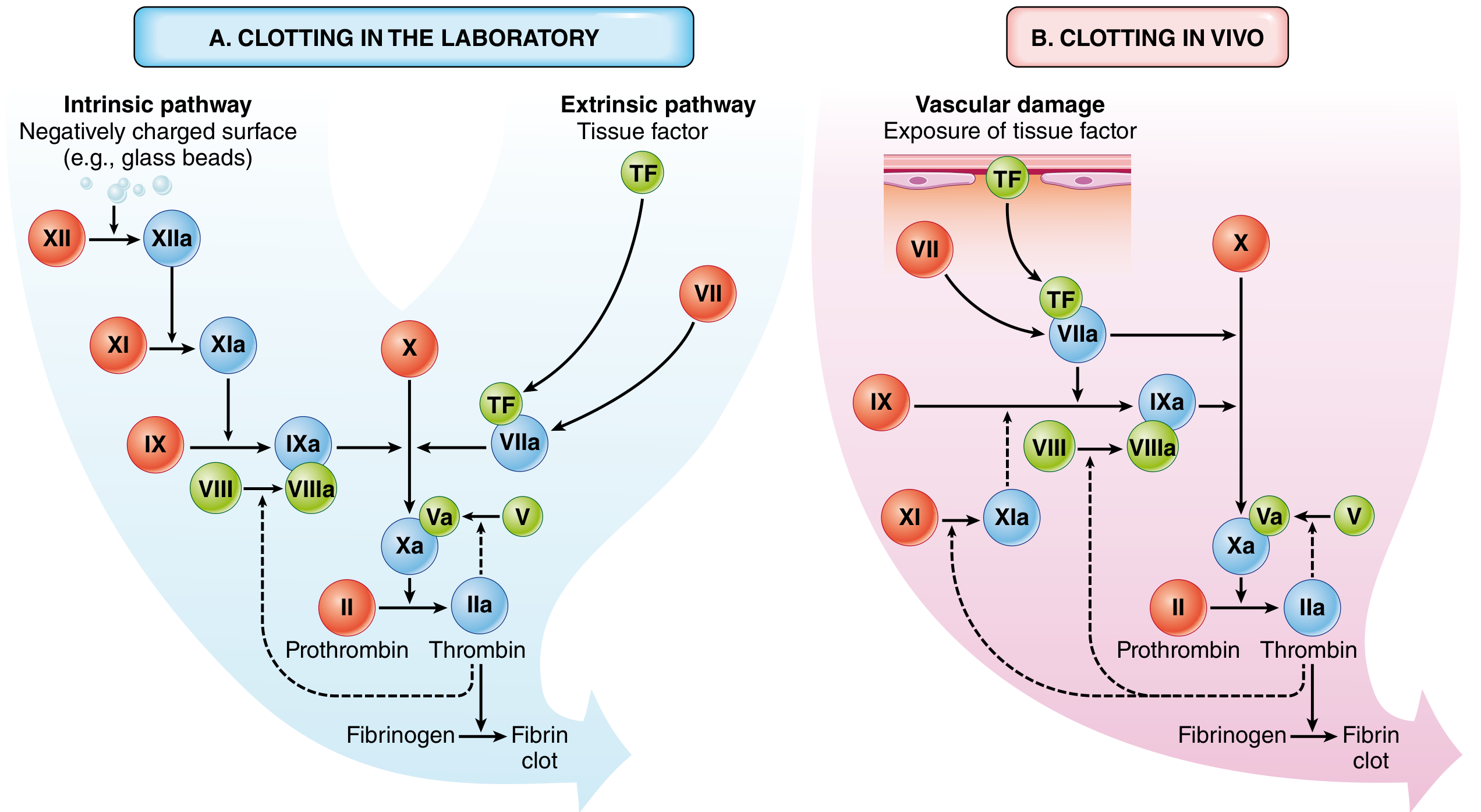
Fig. 4.6 - The coagulation cascade in the laboratory and in vivo. (A) Clotting in the laboratory is initiated by either negatively charged surface (intrinsic pathway) or tissue factor (extrinsic pathway). (B) In vivo, tissue factor is the major initiator; thrombin provides positive feedback (dotted lines). Red = inactive factors, Blue = active factors. Source: Robbins, Cotran & Kumar - Pathologic Basis of Disease.
DIAGRAM 2 - Detailed Cascade with Phospholipid/Calcium Complexes
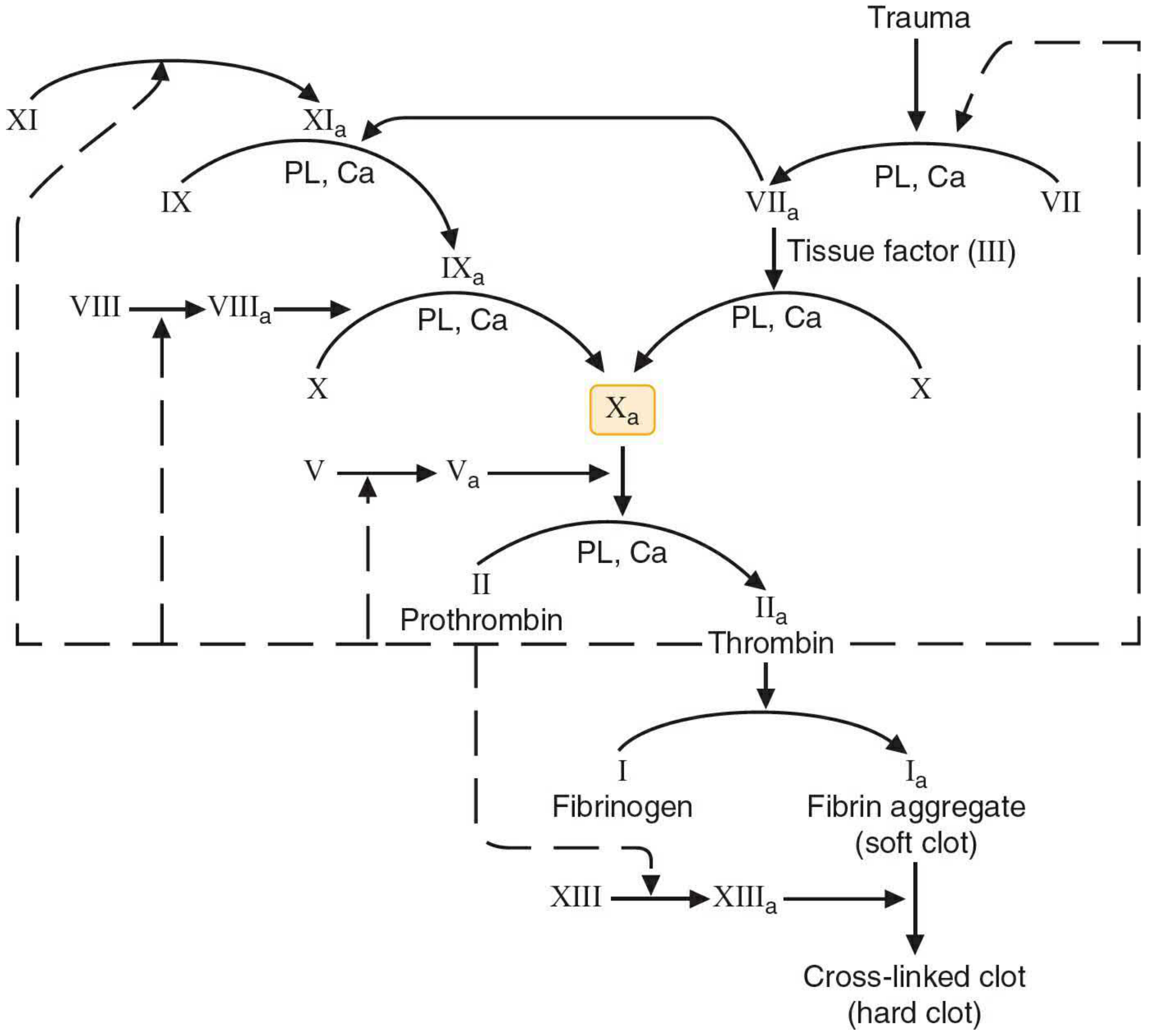
Fig. 43.3 - The blood coagulation cascade. Intrinsic pathway activated by thrombin-driven Factor XIa; extrinsic pathway by tissue factor. All membrane-bound steps (PL, Ca) shown. Dashed lines = positive feedback of thrombin. Source: Basic Medical Biochemistry - A Clinical Approach, 6e.
5. FLOWCHART OF THE COAGULATION PATHWAYS
A. EXTRINSIC PATHWAY (Tissue Factor Pathway - Major in vivo initiator)
Vascular Injury
|
v
Tissue Factor (Factor III) exposed
|
v
Factor VII binds TF --> Factor VIIa (autocatalytic activation)
|
+---> Factor X --> Factor Xa (direct activation)
|
+---> Factor IX --> Factor IXa (cross-activation into intrinsic)
B. INTRINSIC PATHWAY (Contact Activation Pathway)
Negatively charged surface (collagen, glass)
|
v
Factor XII --> Factor XIIa [+ HMWK + Prekallikrein]
|
v
Factor XI --> Factor XIa [also activated by Thrombin - positive feedback]
|
v
Factor IX --> Factor IXa [requires Ca²+]
|
Factor IXa + Factor VIIIa + PL + Ca²+ = TENASE COMPLEX
|
v
Factor X --> Factor Xa
C. COMMON PATHWAY
Factor Xa + Factor Va + PL + Ca²+ = PROTHROMBINASE COMPLEX
|
v
Prothrombin (Factor II) --> Thrombin (Factor IIa)
|
v
Fibrinogen (Factor I) --> Fibrin monomers (soft clot)
|
Factor XIIIa (activated by Thrombin + Ca²+)
|
v
Cross-linked Fibrin (HARD CLOT - stable)
6. ROLE OF THROMBIN - THE MASTER REGULATOR
Thrombin is the central enzyme of hemostasis. Its functions include:
DIAGRAM 3 - Thrombin's Multiple Roles
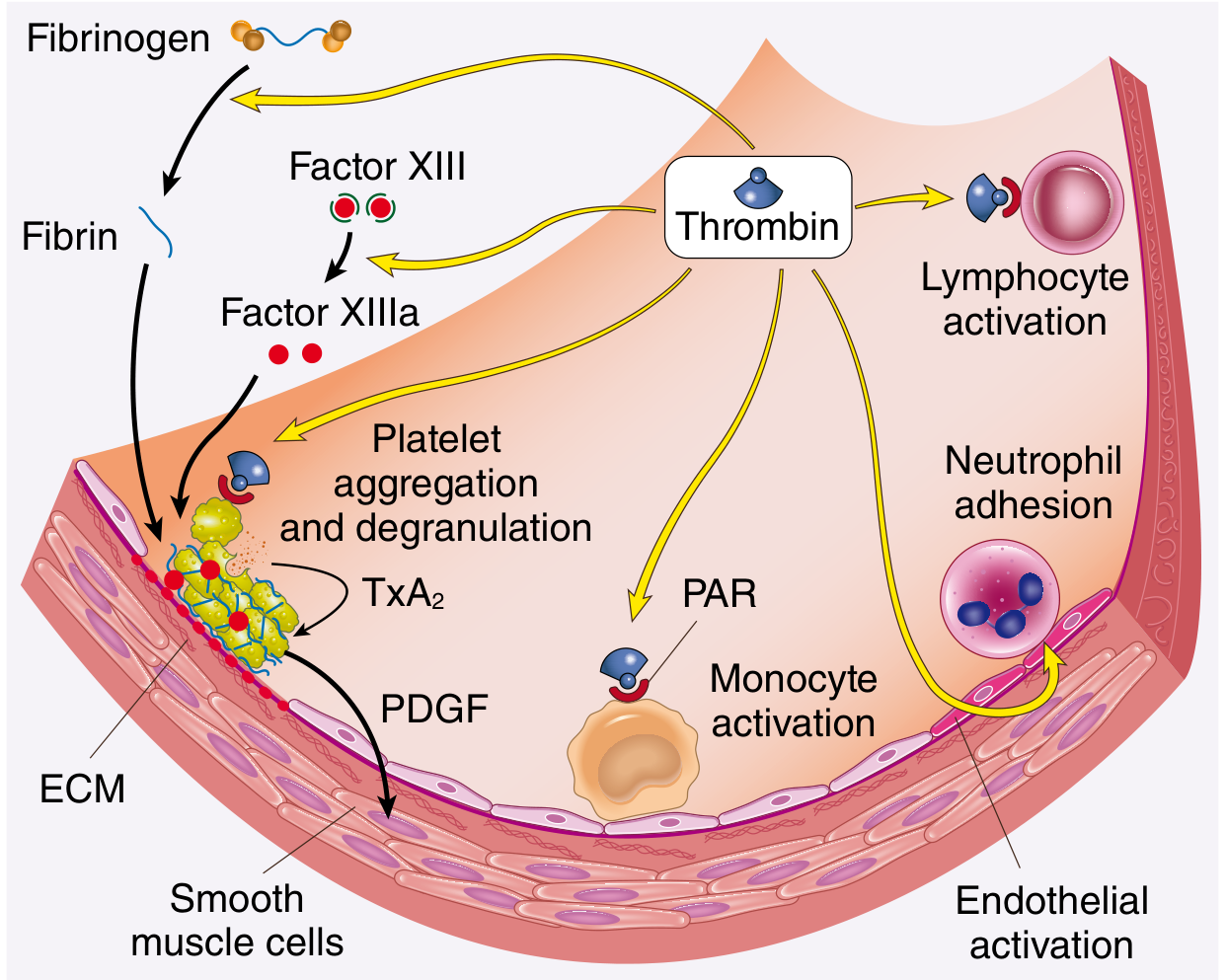
Fig. 4.8 - Role of thrombin in hemostasis and cellular activation. Source: Robbins, Cotran & Kumar - Pathologic Basis of Disease.
Thrombin actions:
- Cleaves fibrinogen to fibrin (structural clot)
- Activates Factor XIII (fibrin cross-linking)
- Activates Factors V, VIII, XI (positive feedback amplification)
- Induces platelet aggregation via PAR receptors
- Activates Protein C (anticoagulant - negative feedback via thrombomodulin)
- Stimulates TxA2 and serotonin release (vasoconstriction)
(Robbins Pathologic Basis of Disease, p. 122-123)
7. FLOWCHART - VITAMIN K DEPENDENT FACTORS
Dietary Vitamin K (K1) / Gut bacteria (K2)
|
v
Vitamin K Epoxide Reductase (VKORC1)
|
v
Reduced Vitamin K (active form)
|
v
Gamma-carboxylation of glutamic acid residues
|
v
Factors II, VII, IX, X + Protein C + Protein S
(now able to bind Ca²+ and assemble on platelet membrane)
|
WARFARIN blocks VKORC1 -> inhibits all above factors
8. ANTICOAGULANT MECHANISMS
FLOWCHART - Natural Anticoagulants
Activated Protein C (APC)
+ Protein S (cofactor)
|
v
Inactivates Factors Va and VIIIa
(Limits amplification of cascade)
Antithrombin III (AT-III)
|
v
Inhibits Thrombin (IIa), Factor Xa, IXa, XIa, XIIa
(Heparin potentiates AT-III 1000-fold)
Tissue Factor Pathway Inhibitor (TFPI)
|
v
Inhibits TF-VIIa-Xa complex
(Limits initiation of extrinsic pathway)
Thrombomodulin (endothelial receptor)
|
v
Binds Thrombin --> Activates Protein C
(Switches thrombin from procoagulant to anticoagulant)
(Harrison's Principles of Internal Medicine 22E, p. 2405)
9. FIBRINOLYSIS PATHWAY
Plasminogen
|
t-PA (tissue plasminogen activator) - synthesized by endothelium
| [potentiated when bound to fibrin]
v
Plasmin (active enzyme)
|
v
Cleaves Fibrin --> Fibrin Degradation Products (FDPs)
--> D-dimers (clinical marker of thrombosis)
|
Counterregulation:
alpha-2-plasmin inhibitor (inhibits free plasmin)
PAI-1 (inhibits t-PA)
10. LABORATORY TESTS OF COAGULATION
| Test | Pathway Assessed | Factors Tested | Normal Value |
|---|---|---|---|
| Prothrombin Time (PT) | Extrinsic | VII, X, V, II, I | 11-13 sec |
| INR | Extrinsic (standardized) | Same as PT | 0.8 - 1.2 |
| aPTT | Intrinsic | XII, XI, IX, VIII, X, V, II, I | 25-35 sec |
| Thrombin Time (TT) | Common (final step) | Fibrinogen | 14-16 sec |
| Bleeding Time | Primary hemostasis | Platelets + vWF | 2-7 min |
| Fibrinogen assay | Common | Factor I | 200-400 mg/dL |
| D-dimer | Fibrinolysis | - | < 0.5 mcg/mL |
(References: Henry's Clinical Diagnosis and Management by Laboratory Methods)
11. CLINICAL RELEVANCE IN ENT SURGERY
ENT-Specific Bleeding Disorders (Scott-Brown, Cummings, Dhingra, Hazarika, Stell & Maran)
Post-tonsillectomy hemorrhage:
- Primary (within 24 hours): surgical bleeding
- Secondary (day 5-10): due to slough of eschar - fibrinolytic excess
- Association with vWD (most common inherited bleeding disorder) and hemophilia
Pre-operative screening relevant to ENT:
- History of easy bruising, prolonged bleeding after dental extraction
- Family history of bleeding
- Routine PT/aPTT before major ENT surgery
- Platelet count, bleeding time
Disorders commonly affecting ENT patients:
| Disorder | Deficient Factor | ENT Manifestation |
|---|---|---|
| Hemophilia A | Factor VIII | Post-op hemorrhage, epistaxis |
| Hemophilia B (Christmas disease) | Factor IX | Post-op hemorrhage |
| von Willebrand Disease | vWF (+/- FVIII) | Epistaxis, post-tonsillectomy bleed |
| Vitamin K deficiency | II, VII, IX, X | Post-op coagulopathy |
| DIC | Multiple | Massive ENT hemorrhage |
| Warfarin therapy | II, VII, IX, X | Elevated PT, peri-op risk |
12. CELL-BASED MODEL OF COAGULATION (Modern Concept)
The classical two-pathway model is an in vitro construct. The cell-based model (Hoffman & Monroe, 2001) better reflects in vivo hemostasis:
FLOWCHART - Cell-Based Model
INITIATION PHASE (on Tissue Factor-bearing cells)
|
TF-bearing cells (fibroblasts, smooth muscle) exposed after injury
|
Factor VII binds TF --> VIIa
|
VIIa-TF activates: Factor X --> Xa (small amount)
Factor IX --> IXa
|
Small thrombin burst (insufficient for clot, but activates platelets)
|
v
AMPLIFICATION PHASE (on platelet surface)
|
Thrombin activates:
- Platelets (release of ADP, TxA2, serotonin)
- Factor V --> Va
- Factor VIII from vWF-FVIII complex --> VIIIa
- Factor XI --> XIa
|
v
PROPAGATION PHASE (on activated platelet surface)
|
IXa + VIIIa + PL + Ca²+ = Intrinsic Tenase
|
Massive activation of Factor X --> Xa
|
Xa + Va + PL + Ca²+ = Prothrombinase
|
Massive Thrombin burst
|
Fibrinogen --> STABLE FIBRIN CLOT
(Recent advance: Yong J & Toh CH, Blood, 2023 [PMID: 37890148] - proposed further refinement linking innate immune activation to coagulation in the convergent model)
13. RECENT ADVANCES IN COAGULATION (2021-2026)
A. Convergent Model of Coagulation
Yong & Toh (2023, Blood) proposed rethinking coagulation as a convergent process integrating enzymatic cascades, cell-based reactions, and innate immune activation. Pattern recognition (DAMPs, PAMPs) triggers both coagulation and complement pathways simultaneously. [PMID: 37890148]
B. Procoagulant Phospholipids on Circulating Blood Cells
Protty et al. (2022, Open Biology) demonstrated that circulating blood cells (platelets, red cells, microparticles) carry procoagulant phospholipids (especially phosphatidylserine) that amplify tenase and prothrombinase complex activity. [PMID: 35440201]
C. Non-Factor Replacement Therapies in Hemophilia
- Emicizumab (Hemlibra): A bispecific antibody that bridges FIXa and FX, mimicking FVIIIa activity - used in Hemophilia A with and without inhibitors (approved FDA)
- Fitusiran: Anti-antithrombin siRNA - reduces AT-III to rebalance hemostasis
- Marstacimab: Anti-TFPI antibody - Phase 3 trial (BASIS trial, Blood 2025) showed significant reduction in annual bleeding rate in hemophilia A/B [PMID: 40608864]
- Concizumab: Anti-TFPI antibody, Phase 3 trial 2023 [PMID: 37646676]
D. Gene Therapy for Hemophilia
- Valoctocogene roxaparvovec (Roctavian): AAV5-based gene therapy for Hemophilia A approved by FDA (2023)
- Etranacogene dezaparvovec (Hemgenix): For Hemophilia B, AAV5-FIX gene therapy - longest follow-up data available
- Review: Chernyi et al., Biomolecules 2024 [PMID: 39062568]
E. DIC - Molecular Mechanisms
Gong et al. (2025, MedComm) - reviewed DIC pathogenesis, highlighting TF overexpression, neutrophil extracellular traps (NETs), complement activation, and endothelial dysfunction as key triggers. [PMID: 39822757]
F. Damage-Associated Molecular Patterns (DAMPs) and Coagulation
Yong & Toh (Br J Haematol, 2026) - DAMPs released during trauma, infection, or ischemia directly activate coagulation independent of the classical TF pathway. [PMID: 41243330]
14. MNEMONICS FOR EXAM
Vitamin K dependent factors: "1972"
- Factors II, VII, IX, X = 2, 7, 9, 10 (and Protein C, S)
Intrinsic pathway factors: "12, 11, 9, 8"
- Factor 12 (Hageman) --> 11 --> 9 --> 8 --> common pathway
Common pathway: "10, 5, 2, 1"
- Factor 10 + 5 --> Thrombin (2) --> Fibrin (1)
PT tests "EXTRINSIC": factors VII, X, V, II, I
aPTT tests "INTRINSIC": factors XII, XI, IX, VIII, X, V, II, I
15. SUMMARY TABLE - FACTOR DEFICIENCIES AND DISORDERS
| Coagulation Factor | Disorder | Lab Finding | Clinical Effect |
|---|---|---|---|
| Factor I (Fibrinogen) | Afibrinogenemia | Elevated PT + aPTT | Severe bleeding |
| Factor II (Prothrombin) | Hypoprothrombinemia | Elevated PT | Bleeding (rare) |
| Factor V | Parahemophilia (Owren disease) | Elevated PT + aPTT | Moderate bleeding |
| Factor VII | Factor VII deficiency | Elevated PT only | Variable bleeding |
| Factor VIII | Hemophilia A | Elevated aPTT | Severe bleeding (X-linked) |
| Factor IX | Hemophilia B | Elevated aPTT | Severe bleeding (X-linked) |
| Factor X | Stuart-Prower deficiency | Elevated PT + aPTT | Moderate bleeding |
| Factor XI | Hemophilia C (Rosenthal) | Elevated aPTT | Mild bleeding |
| Factor XII | Hageman factor deficiency | Elevated aPTT | NO bleeding (but thrombosis risk) |
| Factor XIII | FSF deficiency | Normal PT + aPTT | Delayed bleeding, poor wound healing |
| vWF | von Willebrand Disease | Prolonged bleeding time | Mucous membrane bleeding, epistaxis |
SOURCES / REFERENCES
- Robbins, Cotran & Kumar - Pathologic Basis of Disease (Robbins Pathology) - Chapter 4: Hemostasis and Coagulation Cascade (pp. 121-124)
- Basic Medical Biochemistry - A Clinical Approach, 6e - Chapter 43: Blood Coagulation Cascade (Table 43.2, Fig. 43.3)
- Harrison's Principles of Internal Medicine, 22E - Chapter 122: Overview of the Coagulation Cascade and Venous Thrombosis (pp. 2397-2405)
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery - Perioperative management and bleeding disorders
- Cummings Otolaryngology Head and Neck Surgery - Hemostasis in ENT
- Dhingra's Diseases of Ear, Nose and Throat - Pre-operative workup, bleeding disorders in ENT
- Hazarika - ENT Surgery - Surgical hemostasis
- Stell and Maran's Head & Neck Surgery - Operative bleeding management
- Yong J & Toh CH. Rethinking coagulation: from enzymatic cascade and cell-based reactions to a convergent model involving innate immune activation. Blood. 2023 Dec 21. [PMID: 37890148]
- Gong F et al. Disseminated intravascular coagulation: cause, molecular mechanism, diagnosis, and therapy. MedComm. 2025 Feb. [PMID: 39822757]
- Chernyi N et al. Recent Advances in Gene Therapy for Hemophilia. Biomolecules. 2024 Jul. [PMID: 39062568]
- Matino D et al. Marstacimab prophylaxis in hemophilia: BASIS trial. Blood. 2025. [PMID: 40608864]
- Park S & Park JK. Back to basics: the coagulation pathway. Blood Res. 2024 Oct. [PMID: 39466528]
Exam Tip for RGUHS: For a 20-mark answer, structure as: Introduction (2) + Clotting factors list/table (3) + Extrinsic pathway flowchart (3) + Intrinsic pathway flowchart (3) + Common pathway + Thrombin (2) + Natural anticoagulants (2) + Lab tests table (2) + Clinical relevance in ENT/bleeding disorders (2) + Recent advances (1). Always draw Diagram 1 (classic cascade) and Diagram 2 (detailed with PL/Ca complexes) - examiners expect both.
This is a shared conversation. Sign in to Orris to start your own chat.