Wernickes encephalopathy clinical approach
Reading File
Finding Sources
Finding Sources
Searching PubMed
Wernicke encephalopathy diagnosis treatment thiamine
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the material needed for a thorough clinical answer. Here is the complete synthesis:
Wernicke's Encephalopathy - Clinical Approach
Overview
Wernicke's encephalopathy (WE) is an acute, life-threatening neuropsychiatric emergency caused by thiamine (vitamin B1) deficiency. Carl Wernicke first described the syndrome in 1881, noting mental confusion, ophthalmoplegia, and gait ataxia alongside periventricular hemorrhages at autopsy. It is preventable and treatable, yet autopsy studies show it is diagnosed during life in only ~20% of cases - a major clinical failure.
Pathophysiology
Thiamine is a co-factor for key enzymes in glucose and lipid metabolism (pyruvate dehydrogenase, alpha-ketoglutarate dehydrogenase, transketolase). Deficiency impairs cerebral energy metabolism, producing cytotoxic and vasogenic edema preferentially in periventricular structures. The resulting lesions are symmetrical and involve:
- Periaqueductal grey matter
- Medial thalami
- Mammillary bodies
- Walls of the third ventricle
- Tectal plate
- Pons, medulla, and cerebellar vermis (less common)
- Cranial nerve nuclei III, VI, VIII (responsible for eye signs)
- Hypothalamic/brainstem autonomic pathways (responsible for hypothermia and postural hypotension)
Key precipitant: IV glucose or carbohydrate loading in a thiamine-depleted patient can acutely precipitate WE by exhausting remaining thiamine stores.
Etiology and Risk Factors
Alcoholism is the most common cause, but WE occurs in any state of nutritional compromise:
| Category | Examples |
|---|---|
| Alcohol-related | Chronic alcoholism with poor diet and malabsorption |
| GI causes | Bariatric surgery, prolonged vomiting, malabsorption syndromes |
| Obstetric | Hyperemesis gravidarum |
| Oncological | Systemic malignancy, prolonged IV feeding without thiamine |
| Renal | Hemodialysis or peritoneal dialysis |
| Other | Anorexia nervosa, AIDS, refeeding after prolonged starvation, digitalis poisoning |
High-risk features in alcohol-dependent patients (Maudsley Guidelines): acute withdrawal, malnourishment, decompensated liver disease, homelessness, peripheral neuropathy, prior history of WE, memory disturbance, emergency department attendance.
Clinical Presentation
The Classic Triad (Wernicke's Triad)
- Confusion - most common sign; inattention, apathy, disorientation, memory loss; develops over days to weeks; stupor/coma is rare but possible
- Ophthalmoplegia - bilateral lateral rectus palsy most common; also conjugate gaze palsy and nystagmus (horizontal on lateral gaze, vertical on upgaze); pupillary abnormalities including light-near dissociation
- Gait ataxia - truncal ataxia predominates (limb ataxia is less prominent); reflects cerebellar, neuropathic, and vestibular components
Critical point: The full triad is present in fewer than 30-40% of cases. In a large Spanish retrospective study (n=468), the triad was present in only 39% of alcoholic and 29% of non-alcoholic patients. Never withhold treatment awaiting the complete triad.
Additional signs: Hypothermia, postural hypotension, peripheral neuropathy, signs of decompensated liver disease.
Diagnostic Criteria
Caine Criteria (recommended - higher sensitivity)
Diagnosis requires any 2 of 4 features:
- Dietary deficiency (underweight, thiamine deficiency, abnormal dietary history)
- Oculomotor abnormalities (ophthalmoplegia, nystagmus, or gaze palsy)
- Cerebellar ataxia
- Altered mental state or memory impairment
This captures 85% of autopsy-confirmed cases, though specificity is lower.
Differential Diagnosis
| Condition | Distinguishing features |
|---|---|
| Delirium tremens | Preceded by minor withdrawal; adrenergic overactivity (hypertension, tachycardia, fever); fluctuating course |
| Hepatic encephalopathy | WE can coexist and is a particularly difficult diagnostic challenge in this setting |
| Korsakoff syndrome | Follows repeated/inadequately treated WE; amnesia + confabulation + personality change; largely irreversible |
| Septic encephalopathy | Systemic infection, no specific MRI pattern |
Investigations
MRI Brain (Investigation of Choice)
MRI is the primary neuroimaging tool. CT is much less sensitive and should only be used if MRI is unavailable.
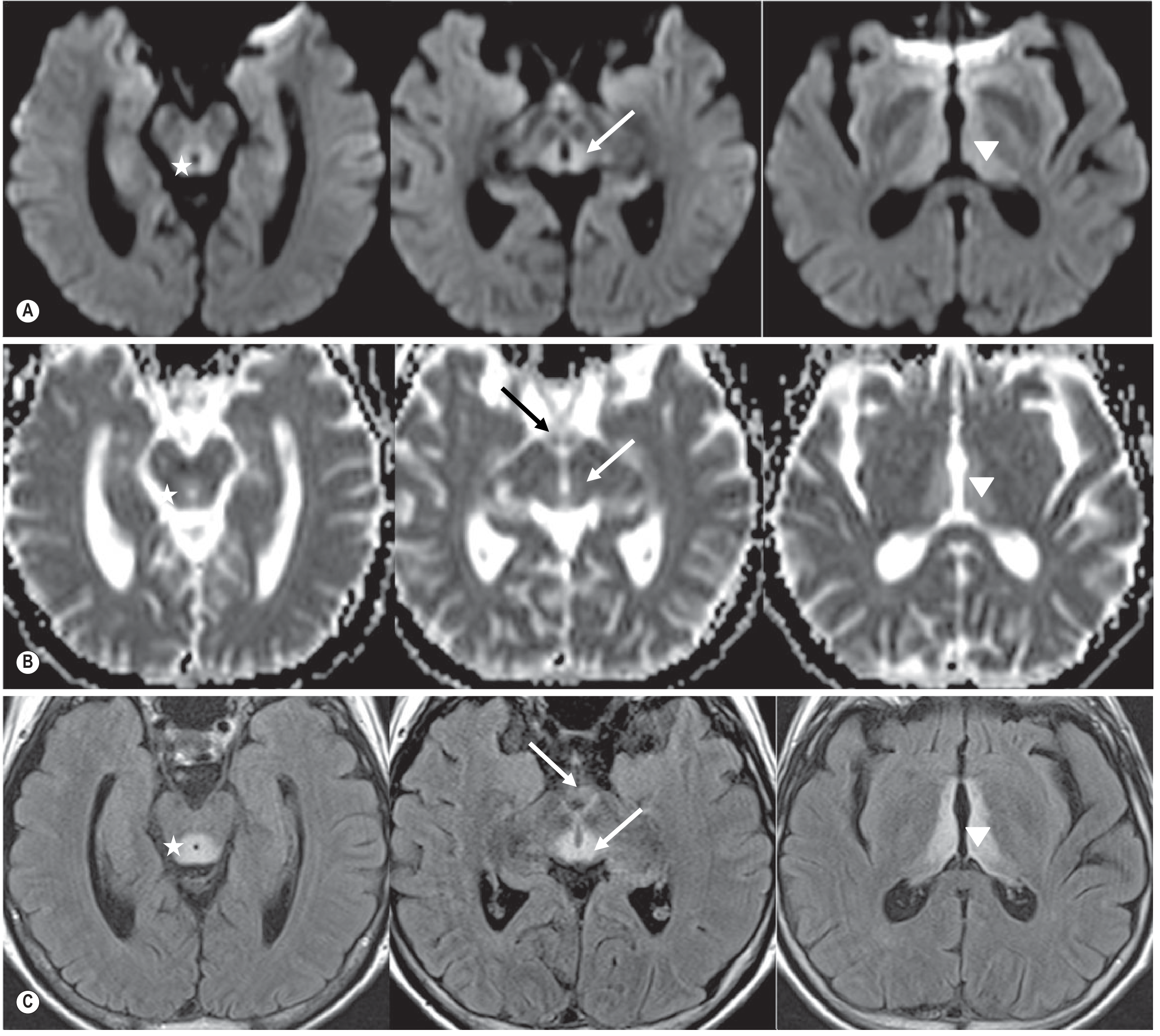
Fig. 58.60 - Wernicke Encephalopathy. Axial DWI (A), ADC maps (B), and T2-FLAIR (C) showing periaqueductal grey (), hypothalamic, mammillary bodies, colliculi (arrows), and mid-thalamic (arrowheads) hyperintensities without restricted diffusivity. (Grainger & Allison's Diagnostic Radiology)*
MRI findings:
- T2/FLAIR hyperintensity in the periaqueductal regions, medial thalami, mammillary bodies, tectal plate
- DWI: restricted diffusion from cytotoxic edema (sometimes increased signal due to vasogenic component)
- Contrast enhancement: present in ~50% of periaqueductal lesions; mammillary body enhancement in ~80% - considered highly specific, even before T2 changes appear
- SWI/gradient echo: microbleeds in thalami and mammillary bodies (indicates poor outcome)
- Chronic changes: brain atrophy, especially mesencephalon and mammillary bodies; shrunken mammillary bodies as late residual finding
- With prompt treatment: signal abnormalities typically resolve completely
Pathology
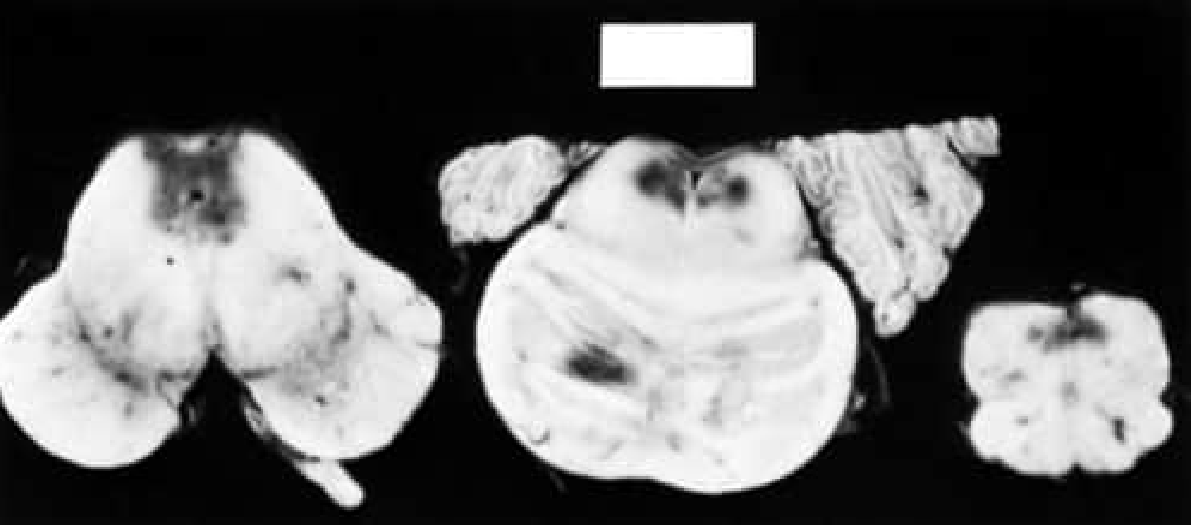
Fig. 85.3 - Acute Wernicke Disease. Hemorrhagic areas adjacent to the fourth ventricle and aqueduct in the medulla, pons, and midbrain. (Bradley & Daroff's Neurology)
Macroscopic: congestion, petechial hemorrhages, shrinkage, discoloration around the aqueduct and third/fourth ventricles. Chronic lesions show glial proliferation and myelin pallor.
Blood Tests
- Serum thiamine level - may be depressed
- Erythrocyte transketolase activity - decreased (more sensitive but less available)
- Serum pyruvate - elevated
- CSF: normal or mild protein elevation
- Note: Do not delay treatment waiting for results
Treatment
Thiamine - Parenteral Route is Preferred
Oral thiamine is not appropriate for suspected or confirmed WE because intestinal absorption is unreliable in malnourished and alcoholic patients. Parenteral administration is mandatory.
Treat before giving glucose. Always give thiamine before any glucose-containing IV fluids to avoid precipitating or worsening WE.
Dosing (Active WE)
| Source | Regimen |
|---|---|
| Bradley & Daroff | 500 mg IV in the acute stage, then 100 mg TDS for the first week |
| Maudsley Guidelines | Transfer to medical unit; IV thiamine; if WE is suspected in hospital, treat immediately |
| Symptom to Diagnosis | 100 mg IV thiamine prior to glucose-containing fluids; continue until symptoms resolve |
Prophylactic Thiamine (High-Risk Patients)
- Community setting: IM thiamine 200-300 mg once daily for at least 3 days
- Hospital setting: IM or IV thiamine 200-300 mg once daily for 3-5 days with daily review
- Low-risk patients (no neuropsychiatric complications, adequate diet): oral thiamine 300 mg daily during assisted withdrawal
NICE (UK) recommends prophylactic parenteral thiamine for harmful/dependent drinkers who are malnourished or have decompensated liver disease AND attend an emergency department or are admitted acutely.
Outcomes and Prognosis
| Feature | Prognosis |
|---|---|
| Ocular signs | Resolve within hours of thiamine administration |
| Horizontal nystagmus | Persists in ~60% even after treatment |
| Gait ataxia | Resolves slowly; abnormal in >1/3 of cases even months after treatment |
| Confusion/encephalopathy | Reverses with treatment |
| Korsakoff syndrome | Follows inadequate treatment; largely irreversible; requires long-term social support |
| Mortality | 10-20% even with thiamine treatment (early studies) |
The Korsakoff syndrome is characterized by amnesia (anterograde >> retrograde), confabulation, relatively intact attention, and personality change. Treatment is limited to social support; acetylcholinesterase inhibitors and memantine have not shown consistent benefit in controlled studies.
Key Clinical Pearls
- Do not wait for the full triad - treat empirically in any at-risk patient with 2/4 Caine criteria
- Always give thiamine before glucose - IV dextrose without thiamine can precipitate or worsen WE
- Non-alcoholic cases are underrecognized - bariatric surgery, hyperemesis gravidarum, malignancy, dialysis patients are all at risk
- Parenteral over oral - GI absorption is unreliable in this population
- Mammillary body enhancement on MRI is highly specific even before T2 changes appear
- Autopsy studies reveal a 5-10x higher prevalence than clinical diagnosis rates, confirming massive underdiagnosis
Recent Evidence
Three relevant systematic reviews (2023-2024):
- Wernicke's in hyperemesis gravidarum - systematic review emphasizing "time is brain" in obstetric cases (PMID 37322816, 2023)
- WE in kidney disease - highlights dialysis patients as a consistently underrecognized risk group (PMID 37838073, 2024)
- Diagnosis and treatment systematic review - General Hospital Psychiatry 2024 (PMID 38306946) - supports early empirical treatment without awaiting lab confirmation
Sources: Bradley & Daroff's Neurology in Clinical Practice; Maudsley Prescribing Guidelines in Psychiatry, 15th ed.; Grainger & Allison's Diagnostic Radiology; Symptom to Diagnosis, 4th ed.; Kaplan & Sadock's Comprehensive Textbook of Psychiatry
This is a shared conversation. Sign in to Orris to start your own chat.