Dry pericarditis, pericardial effusion
Reading File
Finding Sources
Finding Sources
Searching PubMed
"pericarditis" AND "pericardial effusion"
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Searching Images
pericarditis ECG diffuse ST elevation PR depression
Reading File
Searching Images
pericardial effusion echocardiogram cardiac tamponade
I now have comprehensive material. Let me compose the full response.
Dry Pericarditis & Pericardial Effusion
PART 1 — DRY (FIBRINOUS) PERICARDITIS
Definition & Pathophysiology
Pericarditis is inflammation of the pericardium caused by granulocytic and lymphocytic infiltration. "Dry" or fibrinous pericarditis refers to the form without significant fluid accumulation — the exudate is fibrinous, depositing on the pericardial surface and creating the characteristic shaggy, bread-and-butter appearance on gross pathology. It accounts for ~5% of all non-ischemic chest pain presentations.
Etiology
| Category | Examples |
|---|---|
| Infectious (viral/idiopathic) | Coxsackievirus, echovirus, influenza, EBV, HIV; 80–90% labeled idiopathic in Western countries |
| Post-cardiac injury | Acute MI (early), Dressler syndrome (weeks later — anti-myocardial antibodies), post-cardiac surgery, radiation |
| Systemic inflammatory | SLE, RA, SSc, rheumatic fever, sarcoidosis, amyloidosis |
| Uremia | Most common systemic disorder associated with pericarditis |
| Malignancy | Metastatic (lung, breast, lymphoma); primary cardiac tumors |
| Drugs | High-dose anthracyclines, cyclophosphamide, hydralazine, isoniazid, clozapine |
| Other | Trauma (blunt/penetrating), aortic dissection, fungal/parasitic infection, TB (common in developing countries) |
Clinical Features
- Chest pain: sharp, pleuritic, retrosternal; radiates to trapezius ridge or back; relieved by leaning forward, worsened by lying flat, deep inspiration, or swallowing — the single most characteristic feature
- Pericardial friction rub: best heard at the lower left sternal border with diaphragm of stethoscope, patient leaning forward in full expiration; triphasic (atrial systole + ventricular systole + early diastole); intermittent and migratory — may disappear as effusion develops
- Fever and myalgias: common, especially in viral/idiopathic cases
- Classic chest pain and ECG patterns are seen in only ~two-thirds of patients
ECG Changes — Four Stages
The ECG is the most reliable diagnostic tool. It evolves through classic stages:
| Stage | Timing | ECG Findings |
|---|---|---|
| Stage 1 | Hours to days | Diffuse concave ("saddle-shaped") ST elevation in nearly all leads; PR depression (most sensitive early sign) in all leads except aVR (reciprocal PR elevation in aVR); Spodick's sign (downsloping TP segment) |
| Stage 2 | Days | ST and PR normalize; T waves flatten |
| Stage 3 | 1–3 weeks | Deep, symmetric T-wave inversion across leads |
| Stage 4 | Weeks–months | ECG returns to normal (T-wave inversions may persist) |
Key ECG differences from STEMI:
- ST elevation is concave up (not convex/dome-shaped)
- Diffuse across multiple vascular territories, not regionalised
- No reciprocal ST depression (except aVR/aVL)
- No Q-wave development
- Simultaneous T-wave inversion does NOT occur during ST elevation
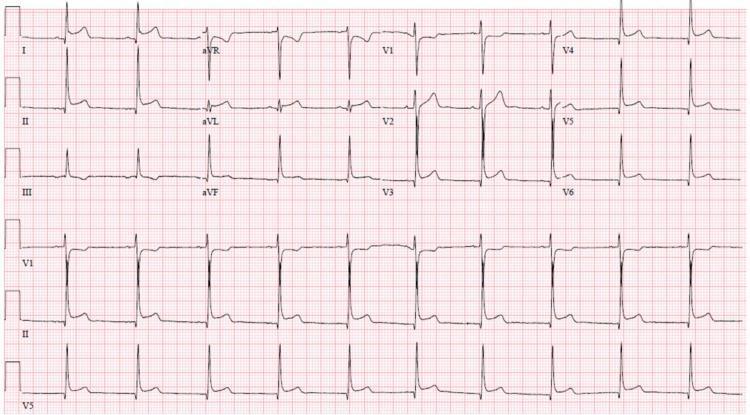
Classic Stage 1 pericarditis ECG: diffuse concave ST elevation, PR depression in inferior/lateral leads, reciprocal PR elevation and ST depression in aVR, and Spodick's sign (downsloping TP segment).
Diagnostic Criteria
Diagnosis requires ≥2 of 4:
- Typical pleuritic chest pain (worse supine, relieved sitting forward)
- Pericardial friction rub
- New widespread ST elevation / PR depression on ECG
- New or worsening pericardial effusion
Investigations
- ECG: staged changes as above
- Echo (POCUS): up to 60% have an effusion; a normal echo does not exclude pericarditis
- CRP: elevated (useful to guide treatment duration)
- CBC: elevated WBC (non-specific)
- Troponin: if elevated → concurrent myopericarditis
- Targeted workup for non-idiopathic causes: ANA, ANCA, dsDNA, RF, TSH, urea/creatinine, HIV serology, Quantiferon-TB
- Cardiac MRI: pericardial delayed gadolinium enhancement confirms active inflammation
Management
Acute pericarditis (aspirin/NSAID + colchicine backbone):
- NSAIDs (first-line): ibuprofen 600 mg QID or indomethacin 25–50 mg TID for 2 weeks; OR aspirin 650–1000 mg TID for 2 weeks
- Colchicine (add-on — halves recurrence rate): 0.5 mg OD (weight <70 kg) or 0.5 mg BD (weight ≥70 kg) for 3 months; start in ED if possible
- Corticosteroids (second-line, use only if NSAIDs/aspirin are contraindicated or ineffective): low-moderate dose prednisone 0.2–0.5 mg/kg/day; higher doses (≥1 mg/kg/day) associated with increased recurrence
- Activity restriction until asymptomatic + CRP normalized (athletes: 3 months minimum)
- If specific etiology found → treat underlying cause
Recurrent pericarditis: same NSAID + colchicine; consider IL-1 antagonists (anakinra, rilonacept) in colchicine-resistant cases
PART 2 — PERICARDIAL EFFUSION
Definition & Normal Values
The pericardial space normally contains 15–35 mL of ultrafiltrate. A pericardial effusion is any excess fluid accumulation in this space. The rate of accumulation matters more than volume — a rapidly accumulating 150 mL can cause tamponade, whereas a slowly developing 1–2 L may be tolerated.
Etiology
Most common: viral/idiopathic pericarditis, malignancy, uremia, trauma, radiation therapy. Less common: drug reactions, autoimmune diseases.
In cancer patients with effusion: ~40% are radiation-induced or idiopathic — only a minority are true malignant effusions. Most common associated cancers: lung, breast, lymphoma, gastrointestinal.
Classification by Size (Echo)
| Size | Volume |
|---|---|
| Small | <10 mm separation |
| Moderate | 10–20 mm |
| Large | >20 mm; requires 200–250 mL to show cardiomegaly on CXR |
Clinical Features
- Often asymptomatic unless large or rapidly accumulating
- Symptoms: cough, dyspnea, chest pain, fever
- Water-bottle sign on CXR: massive symmetric enlargement of cardiac silhouette (loss of normal contours), with obscured hilar vessels — distinguishes large effusion from cardiac chamber enlargement (where hilar structures are conspicuous)
- Posterior displacement of pericardial fat stripe on lateral CXR
Diagnosis
- POCUS/Echo: gold standard — anechoic space between visceral and parietal pericardium; differentiates fluid from chamber enlargement; assesses for tamponade physiology
- CT/MRI: when echo is technically limited; CT may detect purulent or loculated effusions; MRI characterizes fluid composition
- Minimum 200–250 mL needed to produce cardiomegaly on CXR
Pericardial Fluid Analysis
Indicated when infective pericarditis is suspected. Rarely useful otherwise. In autoimmune disease: immune complexes, ANA, anti-dsDNA may be detected in fluid but add little to serum testing.
Cardiac Tamponade
The critical complication — compression of the myocardium by pericardial contents.
Pathophysiology (three-stage continuum):
- Fluid fills pericardial recesses
- Fluid accumulates faster than pericardium can stretch
- Accumulation exceeds compensatory blood volume increase → ↑ intrapericardial pressure → ↓ ventricular compliance → ↓ diastolic filling → ↓ stroke volume → ↓ CO
- Heart compensates with tachycardia until late decompensation
Beck's Triad:
- Hypotension (↓ CO)
- Distended neck veins (↑ venous pressure)
- Muffled heart sounds
(May be absent if tamponade develops rapidly)
Additional findings:
- Pulsus paradoxus: >10 mmHg fall in systolic BP during inspiration (exaggerated ventricular interdependence)
- Kussmaul's sign: absent (differentiates from constrictive pericarditis)
ECG in tamponade:
- Low voltage (fluid attenuates electrical signal)
- Electrical alternans: alternating QRS axis beat-to-beat (pathognomonic — heart swinging in large effusion)
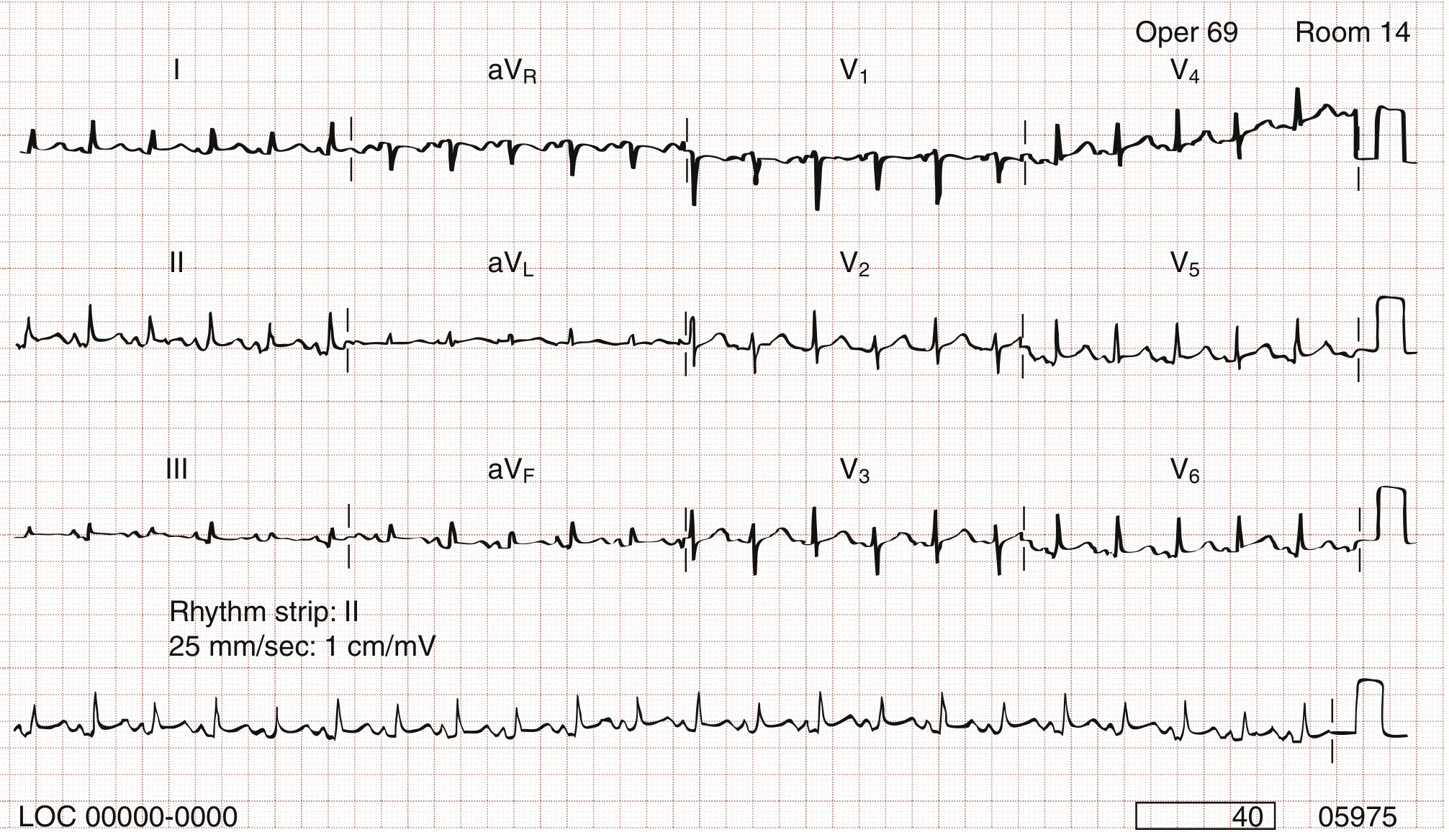
ECG showing electrical alternans — beat-to-beat alternation of QRS amplitude and axis, seen in large pericardial effusions causing cardiac tamponade.
Echo/POCUS in tamponade:
- Large anechoic circumferential space
- Right atrial collapse in late diastole (early sign)
- Right ventricular diastolic collapse (more specific)
- IVC plethora (>2.1 cm, <50% respiratory collapse)
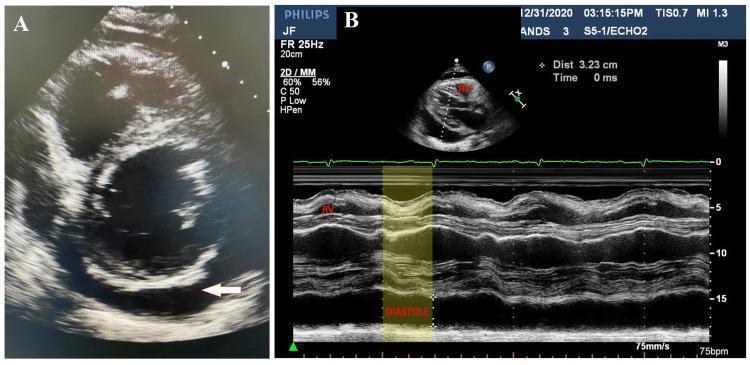
Parasternal short-axis echocardiogram (Panel A) showing large circumferential anechoic pericardial effusion; M-mode (Panel B) demonstrating early diastolic RV free wall collapse (yellow shading) — hallmark of cardiac tamponade physiology.
Hemodynamics: Equalization of right and left ventricular diastolic pressures on cardiac catheterization.
Management of Pericardial Effusion
| Scenario | Management |
|---|---|
| Small, asymptomatic | NSAIDs (ibuprofen 600 mg QID) + close follow-up |
| Moderate–large, symptomatic | Ultrasound-guided pericardiocentesis (diagnostic + therapeutic) |
| Cardiac tamponade | Emergency pericardiocentesis; initial IV fluids to ↑ right-sided filling pressure; avoid vasodilators/diuretics |
| Purulent pericarditis | Pericardiectomy or indwelling catheter + lavage + IV antibiotics ± fibrinolytics |
| Malignant effusion | Pericardiocentesis ± pericardial window/sclerosis; treat underlying malignancy |
Key Comparisons: Dry Pericarditis vs. Effusion vs. Tamponade vs. Constrictive
| Feature | Dry Pericarditis | Pericardial Effusion | Cardiac Tamponade | Constrictive Pericarditis |
|---|---|---|---|---|
| Mechanism | Fibrinous inflammation | Fluid accumulation | Pressure-mediated compression | Fibrotic encasement |
| JVP | Normal | Normal/↑ | ↑↑ | ↑↑ (Kussmaul's +) |
| Pulsus paradoxus | Absent | Absent unless large | Present (>10 mmHg) | Absent/mild |
| ECG | Staged ST/PR changes | Low voltage (if large) | Low voltage + electrical alternans | Normal/non-specific |
| Echo | Small/no effusion | Anechoic space | RV diastolic collapse | Pericardial thickening |
| Friction rub | Present | Disappears as fluid ↑ | Absent | Pericardial knock |
Sources: Rosen's Emergency Medicine 9e, p. 1121–1125; Robbins & Kumar Basic Pathology, p. 377; Braunwald's Heart Disease 12e; Goldman-Cecil Medicine, p. 446–447.
This is a shared conversation. Sign in to Orris to start your own chat.