Renal cell carcinoma
Reading File
Finding Sources
Searching PubMed
"renal cell carcinoma"[MeSH Terms] AND treatment
Reading File
Reading File
Reading File
Searching PubMed
"renal cell carcinoma" AND immunotherapy
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have everything needed for a thorough, well-sourced response.
Renal Cell Carcinoma (RCC)
Overview
RCC is the most lethal of the common urologic cancers, accounting for 80-85% of all primary malignant renal neoplasms and 2-3% of all adult cancers. It is not a single entity but a group of morphologically and genetically distinct tumors, each with different biology, prognosis, and treatment response.
- ~75,000 new cases/year in the United States; ~14,000 deaths annually
- Sixth most common cancer in men, ninth in women
- Male:female ratio approximately 2-3:1
- Peak incidence: 6th-7th decade of life; increasing in those under 40
- Highest incidence in Black Americans; lowest in Asian/Pacific Islanders
- Goldman-Cecil Medicine, p. 2070; Campbell-Walsh Wein Urology, p. 2846
Histologic Subtypes
| Subtype | Frequency | Key Feature | Prognosis |
|---|---|---|---|
| Clear cell | 65-80% | VHL loss, golden yellow, hypervascular | Most aggressive; 90% of metastases |
| Papillary | 10-15% | MET mutations; bilateral/multifocal | Variable (type 1 indolent, type 2 poor) |
| Chromophobe | 3-5% | Hale colloidal iron+; "plant cell" look | Most indolent (except sarcomatoid variant) |
| Oncocytoma | ~10% | Benign; mahogany brown | Benign |
- Robbins & Kumar Basic Pathology, p. 531-536; Campbell-Walsh, p. 2860
Clear Cell RCC - Molecular Pathogenesis
The hallmark is loss/inactivation of both VHL alleles on chromosome 3p25 (sporadic mutation + deletion, or germline in von Hippel-Lindau disease). Without functional VHL protein, hypoxia-inducible factor (HIF) is not degraded and accumulates even in normoxia. HIF then drives transcription of:
- VEGF - promotes tumor angiogenesis (the basis for anti-VEGF/anti-VEGFR therapies)
- Metabolic reprogramming via MYC collaboration
- Additional frequent mutations: PBRM1, SETD2, BAP1 (epigenome regulators)
- Robbins Basic Pathology, p. 531
Papillary RCC
- Type 1: MET proto-oncogene activating mutations; associated with Hereditary Papillary RCC Syndrome (autosomal dominant, chromosome 7q31); multifocal/bilateral; indolent
- Type 2: Higher grade, eosinophilic cells, associated with HLRCC (hereditary leiomyomatosis and RCC); poor prognosis
Chromophobe RCC
- Derived from distal convoluted tubule
- Massive chromosomal losses (chromosomes 1, 2, 6, 10, 13, 17)
- Perinuclear "halo" on histology; stains + for Hale colloidal iron
- Associated with Birt-Hogg-Dube (BHD) syndrome
- Poor outcome only when sarcomatoid dedifferentiation occurs
- Campbell-Walsh, p. 2860
Risk Factors
- Cigarette smoking
- Obesity (risk rises with BMI)
- Hypertension / diuretic use
- Chronic renal failure / hemodialysis (30-fold increased risk with acquired cystic disease)
- Pre-existing renal conditions: polycystic kidney disease, horseshoe kidney
- Occupational cadmium exposure
- Familial: VHL disease, hereditary papillary RCC syndrome, BHD syndrome, HLRCC (~4-6% of all RCC is familial)
Clinical Presentation
The classic triad of flank pain, hematuria, and palpable flank mass is now seen in fewer than 10% of patients (late presentation). Today, >50% of RCCs are discovered incidentally on abdominal CT or MRI done for other reasons.
Symptoms when present:
- Gross or microscopic hematuria (most common presenting symptom)
- Dull flank/back pain
- Palpable mass (late finding)
- Constitutional: fatigue, weight loss, fever
Paraneoplastic syndromes (occur in ~20% of patients):
- Polycythemia (ectopic EPO)
- Hypercalcemia (PTHrP)
- Hypertension (renin secretion)
- Stauffer syndrome (non-metastatic hepatic dysfunction - reverses after nephrectomy)
- Amyloidosis
Metastatic disease (present in ~25-30% at diagnosis):
- Lung (most common)
- Bone (osteolytic)
- Liver, adrenal, brain
- RCC has a marked tendency to invade the renal vein and IVC (tumor thrombus) - seen in ~4-10% of cases
Imaging and Diagnosis
MRI of RCC mass:
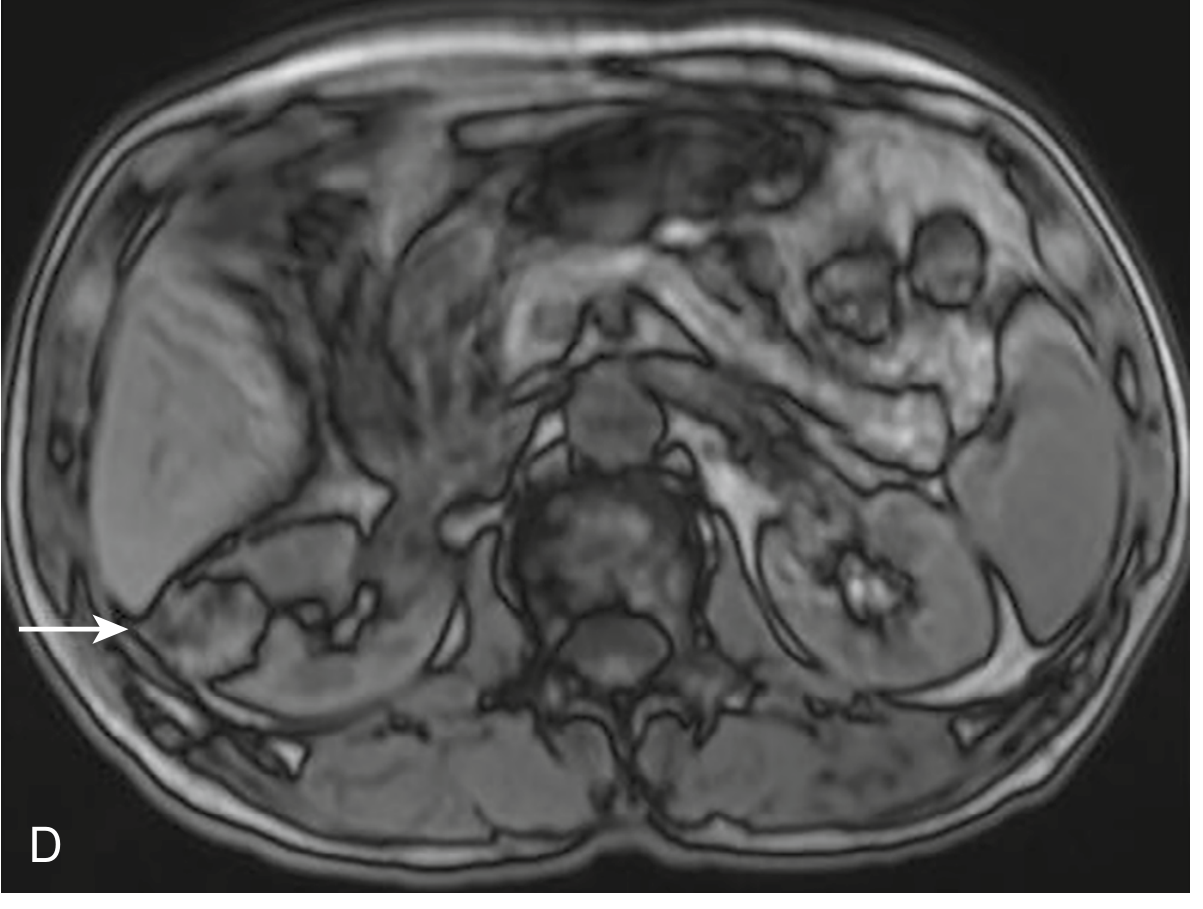
Axial MRI showing a right-sided renal mass (arrow) - National Kidney Foundation Primer, p. 78
- Ultrasound: Low sensitivity for small lesions; can be solid, cystic, or mixed echogenicity
- Multiphasic contrast CT (gold standard): Demonstrates enhancement (key feature distinguishing from cysts). Clear cell RCC shows avid corticomedullary enhancement that becomes hypoenhancing in the nephrographic phase
- MRI: Superior for venous involvement, complex cysts, subtraction imaging; chromophobe RCC enhances avidly in corticomedullary phase (less than clear cell); papillary RCC is hypointense on T2 and hypoenhancing on all phases
- Bosniak classification: Used to stratify cystic renal masses (I-IV) for malignancy risk; Bosniak III-IV lesions require surgical evaluation
- CT chest/abdomen/pelvis: Staging workup; bone scan if symptoms suggest osseous involvement
- National Kidney Foundation Primer, p. 78; Goldman-Cecil, p. 2072
Staging (TNM / AJCC)
| Stage | Description | 5-year Survival |
|---|---|---|
| I | Tumor ≤7 cm, confined to kidney | ~95% |
| II | Tumor >7 cm, confined to kidney | ~75% |
| III | Extends into major veins/perinephric tissue, or regional nodes | ~50-60% |
| IV | Invades beyond Gerota fascia or distant metastases | ~12% |
Treatment
Localized Disease (Stages I-III)
Radical nephrectomy is the standard for large or complex tumors (>7 cm, central, or multiple):
- Laparoscopic or robotic approach now preferred for suitable anatomy
- Includes ipsilateral adrenal (if suspicious), regional lymph nodes
Partial nephrectomy (nephron-sparing surgery):
- Standard of care for T1a tumors (≤4 cm) and strongly preferred for T1b (4-7 cm) when technically feasible
- Equivalent oncologic outcomes with better renal functional preservation
Ablative therapies (cryoablation, radiofrequency ablation):
- For small (<3 cm), peripheral tumors
- Higher local recurrence than surgery; appropriate for poor surgical candidates
Active surveillance: Option for small (<2 cm), incidentally detected masses in elderly or co-morbid patients; growth rate typically slow (~0.3 cm/year)
Adjuvant Therapy
- Pembrolizumab (anti-PD-1): FDA-approved adjuvant therapy for high-risk clear cell RCC after nephrectomy (KEYNOTE-564 trial); significantly improves disease-free survival
- Sunitinib failed to show overall survival benefit in the adjuvant setting
Metastatic / Advanced Disease
RCC is resistant to conventional chemotherapy. Treatment is systemic targeted therapy or immunotherapy:
First-line options (clear cell RCC):
| Drug Class | Agents | Mechanism |
|---|---|---|
| VEGFR TKIs | Sunitinib, Pazopanib, Cabozantinib | Block VEGFR, PDGFR, MET, AXL |
| mTOR inhibitors | Temsirolimus, Everolimus | Block mTOR pathway (HIF suppression) |
| Anti-VEGF antibody | Bevacizumab + IFN-α | Neutralizes VEGF |
| ICI combinations | Nivolumab + ipilimumab (anti-PD1 + anti-CTLA4) | T-cell checkpoint blockade |
| ICI + TKI | Pembrolizumab + axitinib; Nivolumab + cabozantinib; Lenvatinib + pembrolizumab | Dual pathway inhibition |
- Nivolumab + ipilimumab (CheckMate 214): Improved OS vs. sunitinib in intermediate/poor-risk patients - now a preferred first-line option
- Cabozantinib: Multi-kinase inhibitor (VEGFR, MET, AXL); superior PFS vs. sunitinib in intermediate/poor-risk patients (CABOSUN trial)
- Temsirolimus: Particularly beneficial in poor-risk metastatic RCC
- Everolimus: Second-line after TKI failure
mTOR pathway rationale: VHL loss → HIF accumulation → VEGF/mTOR upregulation - both pathways are druggable and clinically validated.
- Campbell-Walsh Urology, p. 2855
Cytoreductive nephrectomy: Removal of the primary tumor before systemic therapy; benefits selected patients with good performance status, especially before TKI therapy (less clear benefit before ICI-based regimens)
Non-clear cell RCC: Less data; MET-directed therapy (cabozantinib, savolitinib) for papillary; everolimus/temsirolimus for chromophobe; clinical trials preferred
Prognosis Factors
Favorable: Clear cell histology (responds to targeted therapy), low IMDC/MSKCC risk score, good performance status, early stage
Unfavorable:
- Sarcomatoid differentiation (any subtype)
- High Fuhrman/ISUP nuclear grade
- Venous invasion, necrosis
- IMDC poor-risk features (anemia, hypercalcemia, thrombocytosis, neutrophilia, KPS <80%, <1 year from diagnosis to treatment)
- BAP1 mutation (vs. PBRM1, which is more favorable)
Hereditary Syndromes
| Syndrome | Gene | Chromosome | Associated RCC |
|---|---|---|---|
| Von Hippel-Lindau | VHL | 3p25 | Clear cell (bilateral, multiple) |
| Hereditary Papillary RCC | c-MET | 7q31 | Type 1 papillary (bilateral, multifocal) |
| HLRCC | FH (fumarate hydratase) | 1q43 | Type 2 papillary (aggressive) |
| Birt-Hogg-Dube | FLCN (folliculin) | 17p11.2 | Chromophobe, oncocytoma |
Key Takeaways
- RCC = cortical tumor from tubular epithelium; 3 main subtypes with distinct molecular drivers
- Classic triad is rare today; most found incidentally on imaging
- VHL/HIF/VEGF axis is the molecular core of clear cell RCC and the basis of most targeted therapies
- Surgical resection (partial or radical nephrectomy) is curative for localized disease
- Metastatic RCC is treated with ICI combinations +/- TKIs; mTOR inhibitors for poor-risk or second-line
- CAR T-cell therapy targeting CD70 is an emerging investigational approach (Phase I data, PMID 38583184)
Sources: Robbins & Kumar Basic Pathology (9780323790185); Campbell-Walsh Wein Urology (9780323546423); Goldman-Cecil Medicine (9780323930345); National Kidney Foundation Primer on Kidney Diseases (9780323791229)
This is a shared conversation. Sign in to Orris to start your own chat.