51yr old male with raised alp 140, raised serum phosphorus 6.14 & serum chloride 97 high triglycerides.History of diabetes, hba1c 8.0 , rbs 200. Possible causes
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
elevated alkaline phosphatase hyperphosphatemia diabetes mellitus
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Searching PubMed
\"alkaline phosphatase\" AND \"metabolic syndrome\" OR \"diabetes mellitus\"
Reading File
Finding Sources
Finding Sources
Loading Image
Loading Image
I now have comprehensive data to provide a full clinical synthesis. Here is the complete answer:
Clinical Analysis: 51yr Male - Raised ALP, Hyperphosphatemia, Hypertriglyceridemia + Poorly Controlled Diabetes
Lab Summary at a Glance
| Parameter | Patient Value | Interpretation |
|---|---|---|
| ALP | 140 U/L | Mildly elevated (normal ~40-129 U/L in adult males) |
| Serum Phosphorus | 6.14 mg/dL | Hyperphosphatemia (normal 2.5-4.5 mg/dL) |
| Serum Chloride | 97 mEq/L | Low-normal / borderline (normal 98-106 mEq/L) |
| Triglycerides | Raised | Dyslipidemia |
| HbA1c | 8.0% | Poorly controlled T2DM |
| RBS | 200 mg/dL | Hyperglycemia |
Most Likely Unifying Diagnosis: Diabetic Nephropathy / Chronic Kidney Disease (CKD)
This is the single most important diagnosis to consider here because it explains nearly all the abnormalities simultaneously.
Mechanism:
- Diabetes mellitus is one of the most common causes of CKD. As GFR declines, the kidney loses its ability to excrete phosphate, leading directly to hyperphosphatemia (serum phosphorus >4.5 mg/dL, and this patient's value of 6.14 is significantly elevated). - Brenner and Rector's The Kidney, Table 73.18
- Reduced renal phosphate excretion is the most common cause of hyperphosphatemia in clinical practice. - Miller's Anesthesia, 10e
- CKD-related secondary hyperparathyroidism and disordered mineral metabolism also drive elevated bone-specific ALP through increased osteoblastic activity (renal osteodystrophy). - Harrison's Principles, 22e
- Insulin resistance in CKD/T2DM drives hypertriglyceridemia via reduced lipoprotein lipase activity and increased VLDL synthesis. - Katzung's Basic & Clinical Pharmacology, 16e
The low-normal chloride (97 mEq/L) fits with a hyperchloremic metabolic acidosis pattern seen in early CKD or diabetic renal tubular acidosis (type IV RTA), where bicarbonate repletion reduces chloride relative to expected, or the modest reduction could represent a mixed acid-base picture with phosphate retention shifting anion balance.
Possible Causes - Organized by Likelihood
1. Metabolic Syndrome / Poorly Controlled Type 2 Diabetes (MOST LIKELY)
This patient has a textbook metabolic syndrome cluster:
- Hypertriglyceridemia is a hallmark of T2DM and insulin resistance - patients with type 2 DM "frequently have hypertriglyceridemia." - Rosen's Emergency Medicine
- Hypertriglyceridemia itself can cause spurious hyperphosphatemia - hyperlipidemia interferes with phosphate measurement colorimetrically. This is important: the raised phosphorus may partly be a laboratory artefact from hypertriglyceridemia. - Brenner and Rector's The Kidney (diagnostic workup note)
- Poor glycemic control (HbA1c 8.0%) promotes hepatic fat deposition (NAFLD/NASH), which can mildly raise ALP.
2. Non-Alcoholic Fatty Liver Disease (NAFLD) / Steatohepatitis
- Common in T2DM and metabolic syndrome; a 51-year-old male diabetic with hypertriglyceridemia has high risk.
- NAFLD/NASH causes intrahepatic cholestasis pattern with mild-to-moderate ALP elevation.
- The ALP isoform (liver vs. bone) should be differentiated using GGT - if GGT is also raised, hepatic origin is confirmed. - Yamada's Textbook of Gastroenterology, 7e
3. Causes of Raised ALP - Full Differential
The table from Yamada's (Table 39.6) lists:
Hepatobiliary:
- Intrahepatic cholestasis: medications/toxins, NAFLD/alcoholic hepatitis, infiltrative lesions, sarcoidosis, lymphoma, amyloidosis, liver metastases, hepatocellular carcinoma
- Biliary obstruction: choledocholithiasis, biliary strictures, cholangiocarcinoma, pancreatic cancer
Extrahepatic (bone):
- Paget's disease - "one of the most common causes of a raised bone alkaline phosphatase in adults" - Quick Compendium of Clinical Pathology, 5e
- Osteomalacia / Vitamin D deficiency
- Bone metastases
- Renal osteodystrophy (fits with CKD context here)
Physiologic/Other:
- Post-meal state (intestinal isoform) - repeat fasting sample
- Medications (anticonvulsants, oral contraceptives)
Here is the diagnostic approach to elevated ALP:
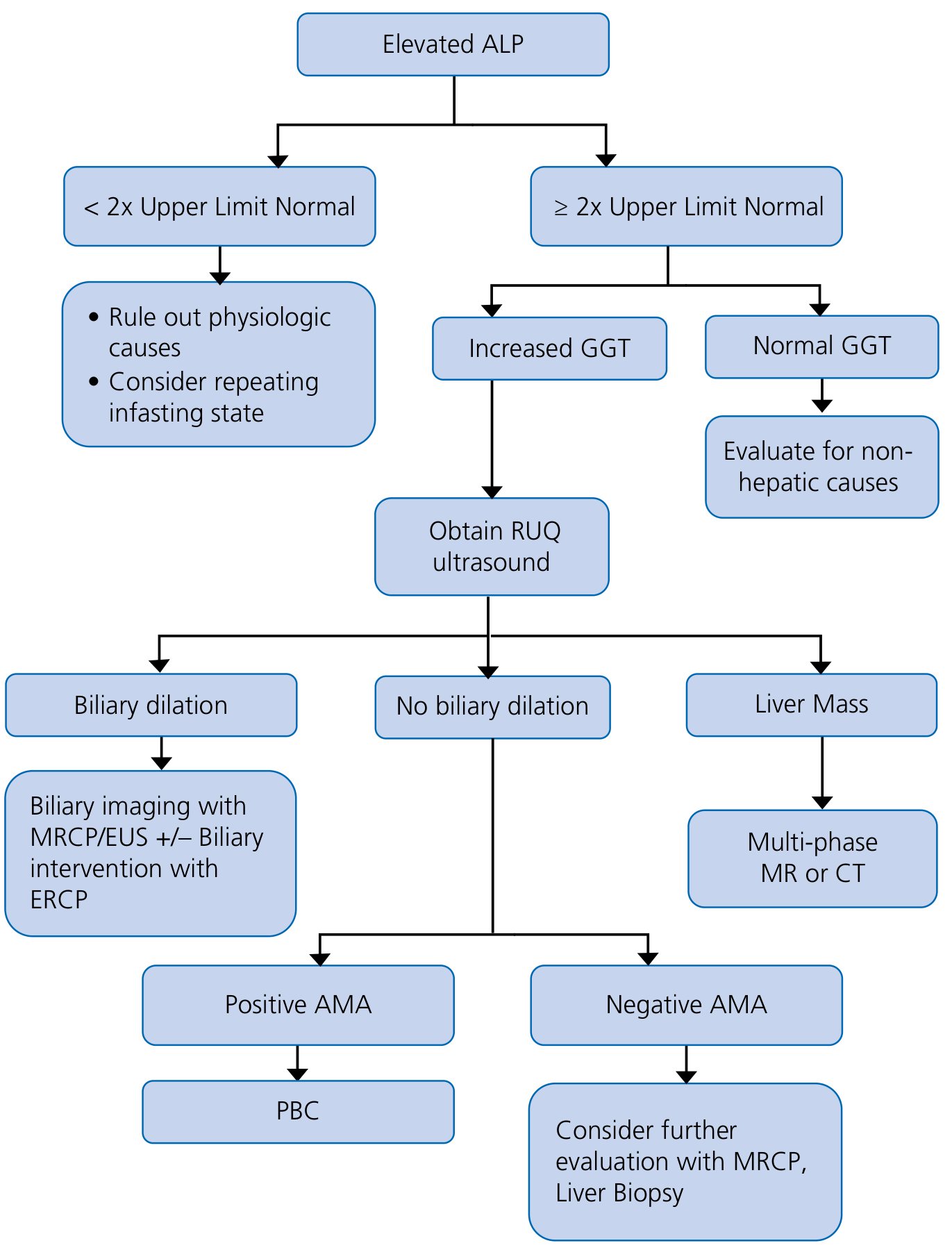
4. Causes of Hyperphosphatemia - Full Differential
The hyperphosphatemia algorithm from Brenner and Rector:
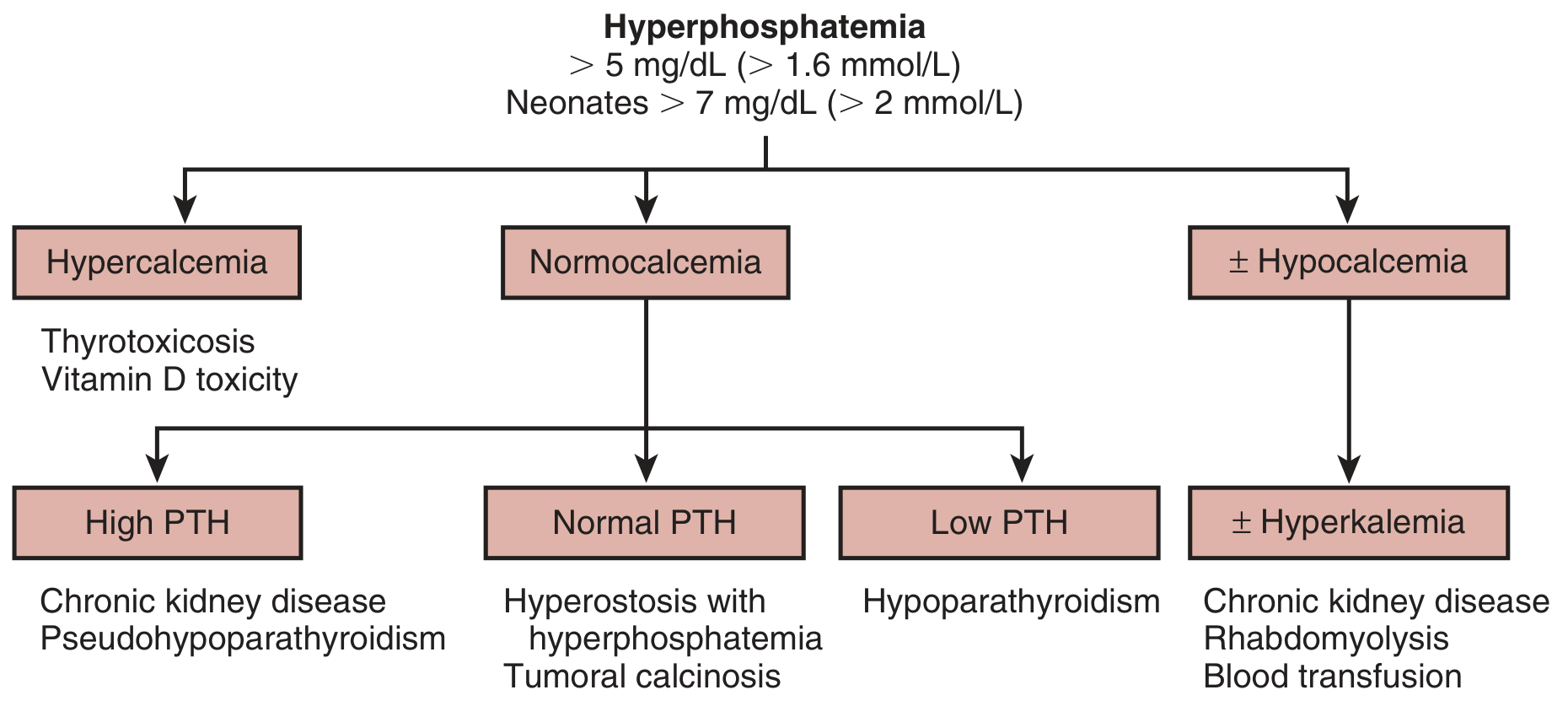
The key diagnostic branches are:
| Associated Calcium | PTH | Leading Diagnosis |
|---|---|---|
| Normocalcemia | High PTH | CKD / Pseudohypoparathyroidism |
| Normocalcemia | Normal PTH | Hyperostosis, tumoral calcinosis |
| Hypocalcemia | Low PTH | Hypoparathyroidism |
| Hypercalcemia | -- | Thyrotoxicosis, Vit D toxicity |
Other causes from the table (Brenner and Rector, Table 73.18):
- Transcellular shift: DKA (cellular shift), metabolic acidosis, rhabdomyolysis, tumor lysis, crush injury
- Increased intake: Phosphate-containing laxatives/enemas, excessive Vitamin D
- Miscellaneous: Acromegaly, tumoral calcinosis, heparin use
Integrating the Full Picture - Key Working Diagnoses
Priority order for this patient:
-
Diabetic nephropathy / CKD - explains hyperphosphatemia, secondary hyperparathyroidism raising bone ALP, hypertriglyceridemia, and borderline chloride. Check serum creatinine, eGFR, urine albumin-creatinine ratio, and PTH immediately.
-
NAFLD/MASH (Metabolic-associated steatohepatitis) - explains mild ALP rise in a diabetic male with hypertriglyceridemia. Check GGT, liver ultrasound.
-
Laboratory artefact - hypertriglyceridemia can falsely elevate measured phosphorus. Re-check phosphorus in fasting state and with lipemia correction.
-
Hypoparathyroidism - if calcium is found to be low, this must be ruled out. However, calcium would typically be low-normal or low if PTH is deficient.
-
Paget's disease of bone - if ALP origin is bone (GGT normal), this is the leading bone cause in a 51-year-old male. Check bone-specific ALP and X-ray of pelvis/spine/skull.
-
Metabolic acidosis (DKA-related or chronic) - can cause transcellular shift of phosphate out of cells, raising serum phosphorus.
Recommended Initial Workup
| Test | Rationale |
|---|---|
| Serum creatinine + eGFR | Screen for CKD |
| Urine albumin:creatinine ratio | Diabetic nephropathy |
| Serum calcium (total + ionized) | Classify hyperphosphatemia |
| PTH (intact) | Secondary vs. primary hyperparathyroidism |
| GGT | Differentiate hepatic vs. bone ALP |
| Liver ultrasound | NAFLD, biliary dilation |
| LFTs (AST, ALT, bilirubin) | Pattern of liver injury |
| Fasting phosphorus | Rule out lab artefact from lipemia |
| 25-OH Vitamin D | Exclude Vit D toxicity |
| Bone-specific ALP (if GGT normal) | Evaluate bone source |
| HCO3 / Blood gas | Assess acid-base status |
Bottom line: In this clinical profile, CKD secondary to diabetes (with renal phosphate retention) combined with NAFLD/metabolic syndrome is the most parsimonious explanation. Laboratory artefact from hypertriglyceridemia causing a spuriously elevated phosphorus must be excluded first before extensive investigation. - Brenner and Rector's The Kidney; Yamada's Textbook of Gastroenterology, 7e; Rosen's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.