Tell me about blood pressure
Reading File
Searching the Web
blood pressure regulation physiology hypertension 2025
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have excellent content from Robbins Pathology and Katzung's Pharmacology, plus the 2025 ACC/AHA guidelines from the web. Here is a thorough overview:
Blood Pressure: A Complete Overview
What Is Blood Pressure?
Blood pressure (BP) is the force that circulating blood exerts against the walls of arteries. It is expressed as two values in mmHg:
- Systolic BP - peak pressure during a heartbeat (heart contracting)
- Diastolic BP - pressure between beats (heart relaxing)
The fundamental equation is:
BP = Cardiac Output (CO) × Peripheral Vascular Resistance (PVR)
- Robbins & Kumar Basic Pathology, p. 309
Blood Pressure Categories (2025 ACC/AHA Guidelines)
| Category | Systolic (mmHg) | Diastolic (mmHg) |
|---|---|---|
| Low (hypotension) | < 90 | < 60 |
| Normal | 90-120 | 60-80 |
| Elevated | 120-129 | < 80 |
| Hypertension Stage 1 | 130-139 | 80-89 |
| Hypertension Stage 2 | ≥ 140 | ≥ 90 |
The 2025 ACC/AHA hypertension guidelines confirm these thresholds remain unchanged from 2017, and recommend initiating antihypertensive therapy when SBP ≥ 130 mmHg or DBP ≥ 80 mmHg for most adults.
How Blood Pressure Is Regulated
Here is a visual summary of the factors controlling BP:
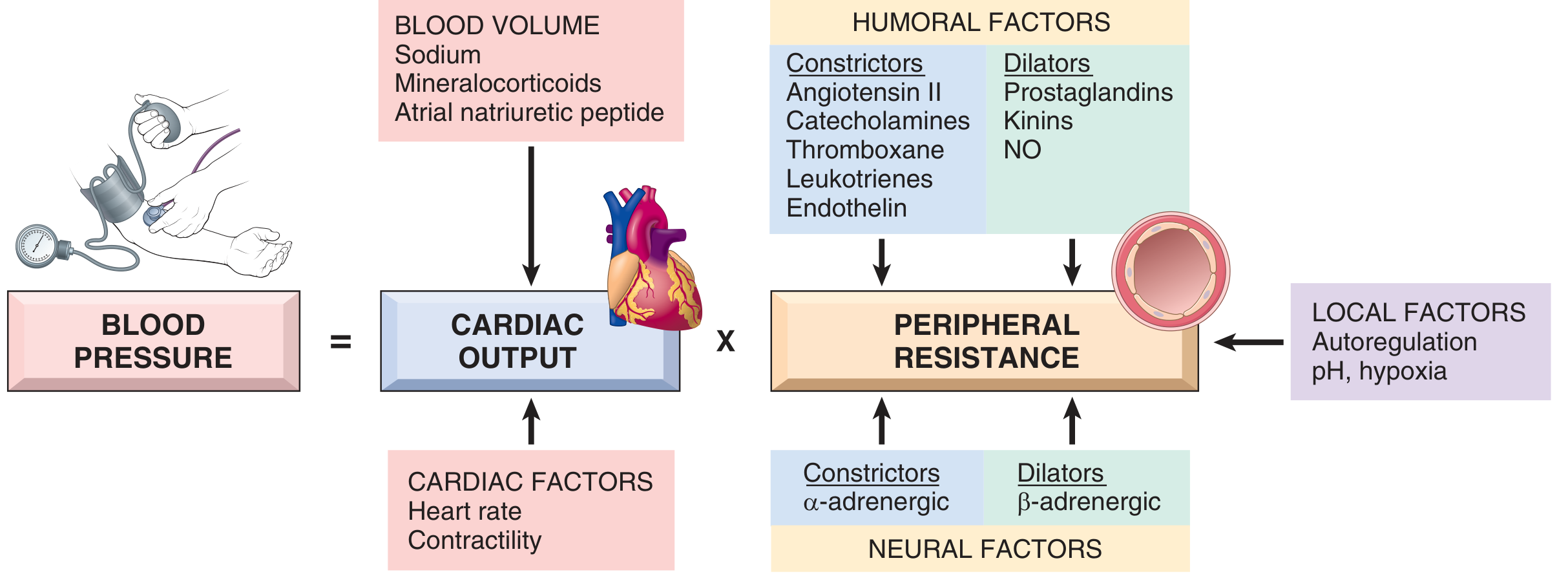
Cardiac Output
- Determined by stroke volume (influenced by filling pressure/preload) and heart rate
- Sodium homeostasis and blood volume regulate stroke volume
- Alpha and beta adrenergic systems control heart rate and contractility
Peripheral Vascular Resistance
Regulated at the arteriole level by a balance of:
| Vasoconstrictors | Vasodilators |
|---|---|
| Angiotensin II | Prostaglandins |
| Catecholamines | Kinins |
| Endothelin | Nitric Oxide (NO) |
| Thromboxane | |
| Leukotrienes |
Neural control: Alpha-adrenergic = constriction; Beta-adrenergic = dilation
Local factors: pH and hypoxia allow fine-tuning to meet metabolic demand
The Renin-Angiotensin-Aldosterone System (RAAS)
The kidneys play a central role:
- Low BP or low sodium triggers renin release from juxtaglomerular cells
- Renin converts angiotensinogen → angiotensin I → (ACE) → angiotensin II
- Angiotensin II causes vasoconstriction and stimulates aldosterone release
- Aldosterone promotes sodium (and water) retention via ENaC in the distal tubule, increasing blood volume and BP
Baroreflexes
Carotid baroreceptors sense stretch from arterial pressure. On standing up, BP briefly drops - baroreceptors detect less stretch, disinhibit sympathetic discharge, causing vasoconstriction and increased cardiac output to restore pressure. - Katzung's Basic and Clinical Pharmacology, 16th Ed., p. 270
Hypertension
Who Gets It?
- Essential (primary) hypertension: No identified cause, accounts for 85-90% of cases
- Secondary hypertension: Identifiable cause (10-15%); includes renal artery stenosis, primary aldosteronism, pheochromocytoma, Cushing's disease, aortic coarctation
Risk Factors
- Age, family history, obesity
- High sodium / low potassium intake
- Physical inactivity, alcohol
- Diabetes, dyslipidemia
- African American ethnicity (higher risk at any BP level)
- Psychological stress
Why It Matters
Starting at 115/75 mmHg, cardiovascular disease risk doubles with every 20/10 mmHg increment. Hypertension damages the heart, brain, kidneys, and blood vessels - often silently until end-organ damage appears. - Katzung's Basic and Clinical Pharmacology, 16th Ed., p. 268
2025 Guideline Updates
The 2025 ACC/AHA guidelines introduced several changes from 2017:
- PREVENT calculator replaces Pooled Cohort Equations for 10- and 30-year CVD risk
- ABPM/HBPM (ambulatory/home BP monitoring) now central to diagnosis - not just office readings
- Expanded screening for primary aldosteronism (regardless of potassium level)
- Renal denervation introduced as Class IIb option for resistant hypertension
- Expanded guidance for CKD, diabetes, pregnancy, and stroke patients
- Term "hypertensive urgency" replaced by "severe hypertension"
Treatment Overview
Lifestyle Modifications (First-line for all)
- Reduce sodium intake (target < 2.3 g/day)
- Increase potassium (fruits, vegetables, DASH diet)
- Regular aerobic exercise (≥ 150 min/week)
- Weight loss
- Limit alcohol
- Quit smoking
Antihypertensive Drug Classes
| Class | Examples | Primary Mechanism |
|---|---|---|
| ACE inhibitors | Lisinopril, enalapril | Block angiotensin II formation |
| ARBs | Losartan, valsartan | Block angiotensin II receptors |
| Calcium channel blockers | Amlodipine, nifedipine | Reduce vascular smooth muscle tone |
| Thiazide diuretics | Hydrochlorothiazide, chlorthalidone | Reduce blood volume |
| Beta-blockers | Metoprolol, atenolol | Reduce heart rate and output |
First-line agents per 2025 guidelines remain: thiazides, ACE inhibitors/ARBs, and CCBs. All antihypertensive drugs work by interfering with the normal regulatory mechanisms described above.
Hypotension (Low Blood Pressure)
- BP consistently below 90/60 mmHg
- Causes: dehydration, blood loss, heart failure, prolonged bed rest, certain medications
- Orthostatic hypotension: BP drops > 20/10 mmHg on standing, causing dizziness or syncope - common in the elderly
- Treatment depends on the cause
Key Takeaways
- BP = Cardiac Output × Peripheral Resistance - all treatments target one or both
- Hypertension is usually silent until it causes stroke, heart attack, or kidney failure
- The 2025 ACC/AHA guidelines emphasize home BP monitoring and refined risk stratification with the PREVENT calculator
- Even modest BP reductions significantly cut cardiovascular risk
This is a shared conversation. Sign in to Orris to start your own chat.