help me study uveitis from the very basics level to advanced level, i am final year ophthalmology resident.
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is your complete uveitis study guide, sourced directly from Kanski's Clinical Ophthalmology (10th ed.) and The Wills Eye Manual, structured from basics to advanced level.
UVEITIS - Complete Study Guide for the Ophthalmology Resident
PART 1 - FUNDAMENTALS
What is Uveitis?
Uveitis is not a single disease but a collection of 30 to 40 different disorders characterized by intraocular inflammation. It is defined by clinical symptoms, anatomic location, morphology, key anatomic findings (KP, cells, snowballs, retinal vasculitis, CME, optic neuropathy), and response to treatment. There is no one "uveitis workup." A shotgun approach is not only not cost-effective - it leads to misdiagnosis based on misunderstanding of the sensitivity and specificity of tests.
The key organizing framework comes from the Standardization of Uveitis Nomenclature (SUN) Working Group, which classifies uveitis by:
- Clinical presentation
- Laterality
- Anatomic location of inflammation
PART 2 - CLASSIFICATION
Anatomical Classification (SUN Criteria)
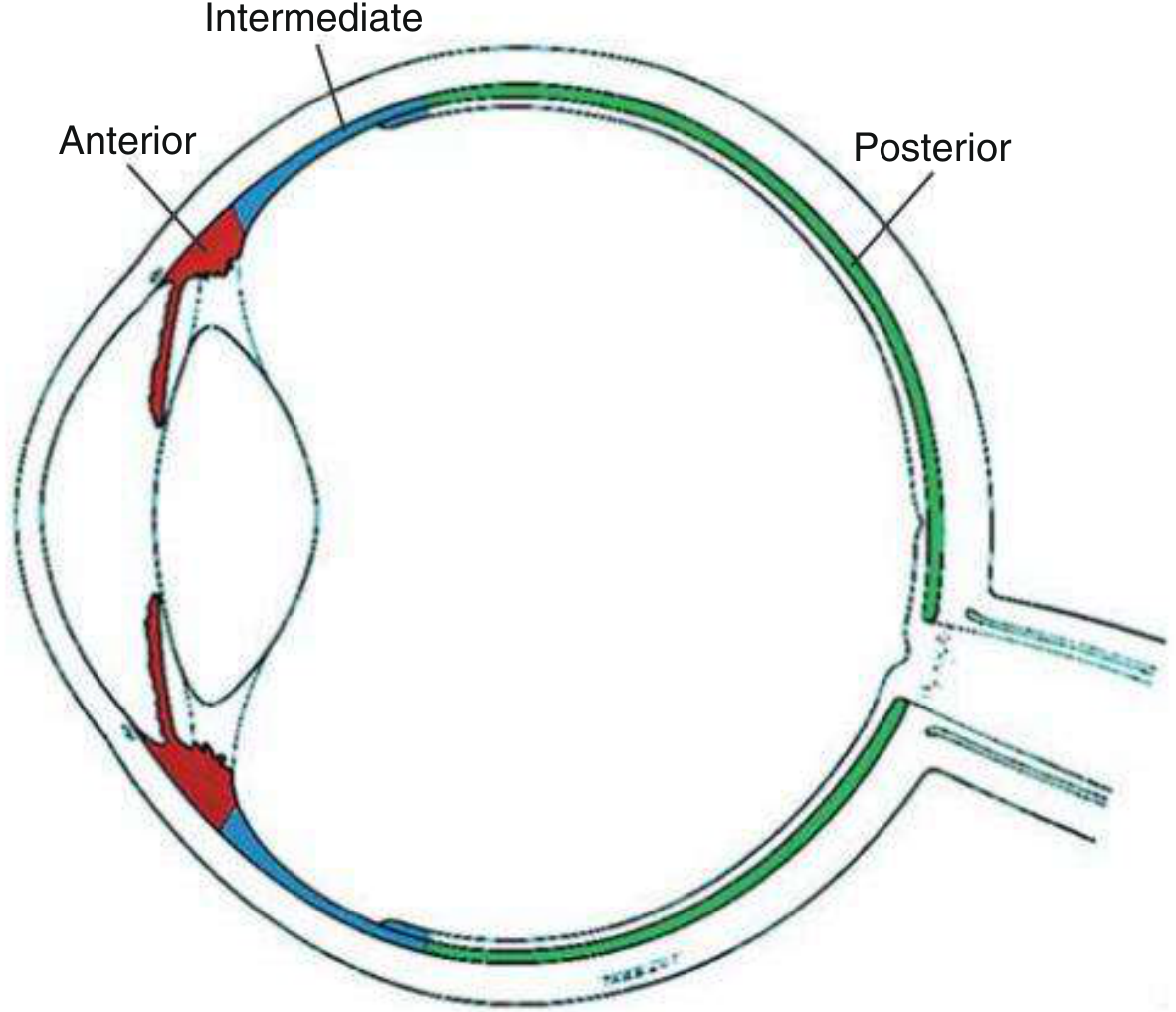
Fig. 12.1 - Anatomical classification of uveitis (Kanski's Clinical Ophthalmology)
| Type | Primary Site | Definition |
|---|---|---|
| Anterior | Anterior chamber (iritis / iridocyclitis) | AC cells > vitreous cells |
| Intermediate | Vitreous (vitritis, pars planitis) | Vitreous cells > AC cells |
| Posterior | Retina / choroid (retinitis, choroiditis) | Posterior to vitreous base |
| Panuveitis | All segments | No predominant site |
Key rule: Isolated anterior uveitis should NEVER be diagnosed without assessment of the retina.
Temporal Classification (SUN)
| Term | Definition |
|---|---|
| Onset | Sudden vs. insidious |
| Duration | Limited (<3 months) vs. Persistent (>3 months) |
| Acute | Sudden onset, limited duration |
| Recurrent | Flare-ups >3 months after stopping therapy |
| Chronic | Persistent, OR flares ≤3 months after stopping therapy |
Important: "Acute or chronic" has no meaning as a combined term. Uveitis controlled on medication = "suppressed," not "in remission."
Morphological Classification
- Non-granulomatous (NG): Fine or small KP, no iris nodules; typical of HLA-B27, JIA, Posner-Schlossman, trauma
- Granulomatous (G): Large "mutton-fat" KP, Busacca/Koeppe iris nodules; typical of sarcoidosis, TB, syphilis, VKH, sympathetic ophthalmia, lens-induced
PART 3 - CLINICAL EXAMINATION
History (Defines Course of Disease)
Key questions:
- Onset (sudden vs. insidious?)
- Laterality (unilateral, bilateral simultaneous, alternating?)
- Duration and course (acute, recurrent, chronic?)
- Systemic review: lower back pain, oral ulcers, skin rash, diarrhea, genital ulcers, joint pain, dysuria, tattoos, IV drug use, recent travel, tick bites
- Prior ocular surgery or trauma
- Medications (rifabutin can cause uveitis + hypopyon)
- Family history
- Immune status (HIV risk factors)
Slit-Lamp Examination - Grading Cells and Flare
Anterior Chamber Cells (SUN Grading) - 1 x 1 mm beam:
| Grade | Cells in field |
|---|---|
| 0 | <1 |
| 0.5+ | 1-5 |
| 1+ | 6-15 |
| 2+ | 16-25 |
| 3+ | 26-50 |
| 4+ | >50 |
Anterior Chamber Flare:
| Grade | Description |
|---|---|
| 0 | None |
| 1+ | Faint |
| 2+ | Moderate (iris/lens details clear) |
| 3+ | Marked (iris/lens details hazy) |
| 4+ | Intense (fibrin/plastic aqueous) |
Keratic Precipitates (KP) - Diagnostic Clues
| KP Type | Associated Conditions |
|---|---|
| Fine KP | HSV, VZV, CMV, Fuchs heterochromic iridocyclitis (FHC) |
| Small non-granulomatous KP | HLA-B27, trauma, masquerade, JIA, Posner-Schlossman, drug-induced |
| Mutton-fat (large greasy) KP | Sarcoidosis, syphilis, TB, sympathetic ophthalmia, VKH, lens-induced |
| Coin-shaped KP | CMV uveitis only (pathognomonic) |
Location of KP: Inferior triangle (Arlt's triangle) is classical. Stellate distribution in Fuchs. Diffuse distribution in herpetic.
Other Slit-Lamp Signs
- Hypopyon: HLA-B27 (most common), Behcet disease, endophthalmitis, retinoblastoma, masquerade (drug-induced: rifabutin)
- Posterior synechiae (PS): More in non-granulomatous; note - PS in pars planitis are uncommon
- Iris nodules: Busacca (in iris stroma - granulomatous), Koeppe (at pupillary margin)
- Heterochromia: Fuchs (affected eye lighter), siderosis, Horner's
- Band keratopathy: Calcium deposits at 3 and 9 o'clock - chronic uveitis, JIA, hypercalcemia
Vitreous Haze Grading (SUN/NEI Scale)
| Grade | Description |
|---|---|
| 0 | Clear |
| 0.5+ | Slight haze |
| 1+ | Disc margins slightly blurred, vessels clear |
| 2+ | Disc margins blurred, vessel detail visible |
| 3+ | Disc barely visible |
| 4+ | Disc/vessels invisible |
PART 4 - ANTERIOR UVEITIS (Most Common - 50-60% of All Uveitis)
Etiology Overview
| Category | Examples | Approximate Frequency |
|---|---|---|
| Idiopathic | No systemic association | ~50% |
| HLA-B27-related | AS, ReA, IBD, psoriatic arthritis | ~20% of AAU |
| Infections | VZV, HSV, TB, syphilis, Lyme | Varies |
| Other non-infectious | JIA, sarcoidosis, Behcet, MS, SLE, TINU | Varies |
| Masquerade | Lymphoma, melanoma, retinoblastoma, JXG | Rare |
Acute Anterior Uveitis (AAU)
Symptoms: Rapid onset of unilateral pain, photophobia, redness, watery discharge, blurred vision
Signs: Ciliary flush, AC cells and flare, KP (usually fine/non-granulomatous), PS
Pathophysiology: IL-6 released by monocytes/macrophages drives the aberrant immune response. May involve cross-reactivity with microbial antigens in genetically predisposed individuals.
Prognosis: Generally good if managed adequately.
Chronic Anterior Uveitis (CAU)
- Less common than AAU
- More often bilateral
- Systemic disease more likely
- Granulomatous signs often present
- Variable prognosis
HLA-B27-Associated Uveitis
Critical features: Recurrent, unilateral (or alternating bilateral), non-granulomatous anterior uveitis
Signs: Severe AC reaction with cells, flare, and fibrin. Most common cause of unilateral hypopyon. Tendency for early posterior synechiae. More common in men.
Over half of patients presenting with HLA-B27-positive AAU have an underlying seronegative spondyloarthropathy, and of those, over half are diagnosed only after the onset of uveitis.
The HLA-B27 Diseases (PAIR mnemonic):
- Psoriatic arthritis (upper extremity joints, skin/nail changes)
- Ankylosing spondylitis (young adult men, lower back pain/stiffness, sacroiliitis on XR)
- Inflammatory bowel disease (Crohn's/UC; IBD + HLA-B27 negative: more sclerokeratitis/PUK than uveitis)
- Reactive arthritis / Reiter syndrome (urethritis, arthritis, conjunctivitis; lower extremity joints)
- HLA-B27-associated uveitis without systemic disease (also occurs)
Workup: HLA-B27 testing, sacroiliac joint X-ray, ESR/CRP, HLAB27+ → refer to rheumatology.
Juvenile Idiopathic Arthritis (JIA) Uveitis
- Most common in oligoarticular JIA, ANA-positive, young girl
- Chronic, bilateral, insidious, non-granulomatous, NO pain or redness - often asymptomatic
- Screening schedule mandatory (every 3-6 months in high-risk; every 12 months in low-risk)
- Complications: Band keratopathy, cataract, CMO, glaucoma, hypotony
- Treatment: Topical steroids (effective in 80%), cycloplegics; systemic immunosuppression early (methotrexate, adalimumab, infliximab)
- Avoid etanercept - can cause severe worsening
- Tocilizumab (anti-IL-6) - effective in refractory cases
Fuchs Heterochromic Iridocyclitis (FHC)
- Unilateral, low-grade, chronic, painless
- Fine stellate KP throughout the corneal endothelium (not in triangle)
- Mild AC cells, no flare, NO synechiae (pathognomonic feature)
- Heterochromia (affected eye lighter - lighter iris = affected)
- Cataract (very common, surgery has good outcomes)
- Secondary glaucoma common
- No synechiae = no treatment with cycloplegics routinely needed
- Rubella virus implicated (PCR of AC tap)
Posner-Schlossman Syndrome (Glaucomatocyclitic Crisis)
- Recurrent, unilateral, mild non-granulomatous AAU with markedly elevated IOP
- Small fine KP, minimal cells, large open angle
- IOP can reach 40-60 mmHg during attack
- CMV implicated (treat with ganciclovir/valganciclovir if suspected)
- Manage IOP with topical antiglaucoma medication; mild topical steroids
Lens-Induced Uveitis
- Phacoantigenic (phacoanaphylactic): True granulomatous immune reaction to lens protein after rupture; mutton-fat KP; treat by removing offending lens material
- Phacolytic: Non-granulomatous; hypermature cataract leaks protein through intact capsule → macrophage-mediated; high IOP; treat urgently with cataract extraction
PART 5 - INTERMEDIATE UVEITIS
Key Features
- Primary site: vitreous (vitritis is the hallmark)
- Insidious onset, painless, floaters dominant symptom
- Typically bilateral but asymmetric (though initial complaints often unilateral)
- Age: 15-40 years, no gender predilection
- Accounts for up to 15% of all uveitis; 20% of pediatric uveitis
Pars Planitis vs. Intermediate Uveitis
Pars planitis = subset of IU where there is snow-banking and/or snowball formation AND the inflammation is idiopathic (no underlying infection or systemic disease)
If a systemic disease is identified → term is "intermediate uveitis," not pars planitis.
Signs
| Finding | Description |
|---|---|
| Snowballs | Whitish focal collections of inflammatory cells, most numerous inferiorly |
| Snowbank | Grey-white fibrovascular/exudative plaque over inferior ora serrata and pars plana - seen only with indirect ophthalmoscopy + scleral depression |
| Peripheral periphlebitis | Especially in multiple sclerosis |
| AC cells | Mild; few fine/small KP occasionally |
Complications
CME (most common cause of vision loss), vitreous hemorrhage (acute vision loss especially in children), posterior subcapsular cataract, band keratopathy, secondary glaucoma, ERM, exudative RD, peripheral neovascularization
Etiology
- Pars planitis: >70% (idiopathic autoimmune)
- Sarcoidosis
- Multiple sclerosis
- Lyme disease
- Syphilis
- TINU (tubulointerstitial nephritis + uveitis)
- Primary intraocular lymphoma (masquerade - ask about neurological symptoms in older patients; low threshold for CNS imaging)
Treatment
- Periocular steroids (transseptal or subtenon triamcinolone) - first line for vision-threatening IU
- Systemic steroids
- Immunosuppressives (methotrexate, azathioprine, mycophenolate, cyclosporine, biologics)
- Pars plana vitrectomy for persistent vitreous opacification or vitreous hemorrhage
- Laser photocoagulation for peripheral retinal neovascularization
- Follow for MS: MRI brain + neurology referral if snowbanking + other neurological symptoms
PART 6 - POSTERIOR UVEITIS
Overview
Posterior uveitis includes retinitis, choroiditis, retinochoroiditis, or chorioretinitis. There may be posterior vitreous cells, optic disc edema and hyperemia.
Terminology:
- Retinochoroiditis: Primary retinal involvement with secondary choroidal extension
- Chorioretinitis: Primary choroidal involvement with secondary retinal extension
Toxoplasma Retinochoroiditis (Most Common Cause of Posterior Uveitis Worldwide)
Organism: Toxoplasma gondii (obligate intracellular parasite)
Clinical hallmark: Active white/yellow retinitis lesion adjacent to an old chorioretinal scar - "headlight in the fog" or "satellite lesion" appearance - with overlying vitritis
Pathognomonic combination: Active focus ("headlight") + old scar + vitritis
Forms:
- Acquired (most common): Reactivation of congenital infection; typically single active focus adjacent to old scar
- Congenital: Bilateral, macula often involved
- Immunocompromised (HIV/AIDS): Atypical - larger lesions, no old scar, bilateral, may mimic CMV retinitis
Workup: Toxoplasma serology (IgG/IgM); PCR of AC tap in atypical cases; negative IgM + IgG rules out most cases
Who to Treat (Wills criteria):
- Lesion in or near macula / within 2-3 mm of disc
- Threatening a large retinal vessel
- Lesion >1 disc diameter
- Severe vitritis with decreased vision
- Immunocompromised patient
- Self-limited in immunocompetent with peripheral lesions = may observe
Treatment:
Classic Triple Therapy (4-6 weeks):
- Pyrimethamine 200 mg load then 25-50 mg/day
- Sulfadiazine 2 g load then 1 g QID (or TMP/SMX 160/800 mg BID as alternative)
- Folinic acid (NOT folic acid) 10 mg every other day (prevents bone marrow suppression)
- Add prednisone 20-60 mg/day at least 24 hours AFTER starting antimicrobials; taper 10 days before stopping antibiotics
Monitor: CBC weekly (pyrimethamine causes thrombocytopenia/leukopenia) - reduce dose if platelets <100,000. Do not give vitamins containing folic acid.
Alternate regimens:
- Clindamycin 150-450 mg QID (alone, or with pyrimethamine if sulfa allergy); warn about pseudomembranous colitis
- Intravitreal clindamycin (1 mg) + dexamethasone (400 mcg): effective for macular-threatening cases; 2-3 injections 2 weeks apart; preferred in pregnancy reactivation
- Azithromycin, atovaquone also used
Pregnancy: Avoid pyrimethamine → use spiramycin 1 g TID if seroconversion occurs
Sarcoidosis - Ocular Manifestations
Sarcoidosis can cause any pattern of uveitis - anterior, intermediate, posterior, or panuveitis. Most common: bilateral chronic granulomatous anterior uveitis.
Classic ocular signs suggesting sarcoidosis (IWOS criteria, 7 signs):
- Mutton-fat or granulomatous KP, and/or Busacca/Koeppe iris nodules
- Trabecular meshwork nodules, and/or tent-shaped PAS
- Snowball/string-of-pearls vitreous opacities
- Multiple peripheral chorioretinal lesions (active/atrophic)
- Nodular/segmental periphlebitis (candle-wax drippings) ± retinal macroaneurysm
- Optic disc nodule/granuloma and/or solitary choroidal nodule
- Bilaterality
Diagnostic levels (IWOS):
- Definite: Biopsy + compatible uveitis
- Presumed: No biopsy + bilateral hilar lymphadenopathy (BHL) on CXR + compatible uveitis
- Probable: No biopsy, no BHL, >3/7 signs + >2/5 positive lab tests
- Possible: Negative lung biopsy + >4/7 signs + >2/5 positive lab tests
Labs: ACE (elevated in 60%), serum lysozyme, LFTs, renal function, calcium (hypercalcemia/hypercalciuria), CXR (BHL), CT chest, bronchoalveolar lavage (CD4/CD8 ratio), PET scan
Treatment: Stepwise:
- Anterior/intermediate: Topical steroids, periocular steroids
- Posterior: Systemic steroids + steroid-sparing immunosuppressives (methotrexate, azathioprine, cyclosporine, TNF inhibitors e.g. adalimumab)
- Peripheral neovascularization: Scatter laser
- CME: Topical NSAID + periocular/systemic steroids
Vogt-Koyanagi-Harada (VKH) Syndrome
Pathophysiology: Autoimmune T-cell-mediated granulomatous reaction against melanocytes (choroidal, skin, meninges, inner ear)
Demographics: Asian, Middle Eastern, Latino, Native American descent; HLA-DR4 associated
Phases:
- Prodromal (viral-like, 3-5 days): Headache, fever, meningismus, CSF pleocytosis, tinnitus, dysacusis, vitiligo-like alopecia
- Acute uveitic (weeks): Bilateral granulomatous posterior uveitis, multifocal exudative serous retinal detachments, disc hyperemia, choroidal folds
- Chronic recurrent (months): Anterior uveitis flares
- Chronic/Convalescent (late): "Sunset glow" fundus (diffuse choroidal depigmentation), Dalen-Fuchs nodules, perilimbal depigmentation (Sugiura sign), poliosis, vitiligo
Key investigation: FA shows pin-point leakage in the acute phase with progressive subretinal pooling; B-scan shows serous detachments
Diagnostic Criteria (Revised, 2001):
- Complete VKH: Criteria 1-5 all present
- Incomplete VKH: Criteria 1-3 + either 4 or 5
- Probable VKH (isolated ocular disease): Criteria 1-3
Treatment: High-dose systemic steroids initiated rapidly in the acute phase is key to good outcome. IV methylprednisolone pulse therapy (1 g/day x 3 days) followed by oral prednisolone 1 mg/kg/day with slow taper over 6-12 months. Add immunosuppressives (azathioprine, cyclosporine, mycophenolate) for steroid sparing in chronic disease.
Sympathetic Ophthalmia
- Bilateral granulomatous panuveitis following penetrating ocular injury or surgery to one eye (the "exciting" eye)
- Can occur from 10 days to decades after injury (peak: 2 weeks to 2 months)
- Pathognomonic finding: Dalen-Fuchs nodules (nodules between RPE and Bruch's membrane)
- Clinically resembles VKH - bilateral mutton-fat KP, choroidal thickening, serous RD, "sunset glow" fundus
- Prevention: Enucleation of the exciting eye within 14 days of injury (controversial after 14 days)
- Treatment: Same as VKH - high-dose systemic steroids + immunosuppressives
Behcet Disease Uveitis
Triad: Oral ulcers (recurrent) + genital ulcers + uveitis
HLA: HLA-B51 associated; more common in Turkey/Middle East/Japan ("Silk Road disease")
Ocular features:
- Severe bilateral panuveitis - one of the most vision-threatening uveitides
- Recurrent, alternating, or bilateral non-granulomatous uveitis
- Hypopyon uveitis (shifting hypopyon - unlike in HLA-B27 which is more sticky/fibrinous)
- Occlusive retinal vasculitis (obliterative, affecting arteries and veins) - distinct feature
- Retinal infiltrates (inner retinal hyperreflective lesions on OCT)
- Optic disc edema, vitreous hemorrhage, retinal neovascularization
Workup: HLA-B51, pathergy test (positive = 2mm papule/pustule 48h after skin prick), ESR, clinical diagnosis based on International Study Group criteria
Treatment: Systemic immunosuppression is mainstay - azathioprine, cyclosporine, colchicine; TNF inhibitors (infliximab, adalimumab) are highly effective for severe ocular disease; avoid topical steroids alone (inadequate)
PART 7 - INFECTIOUS UVEITIS (Major Causes)
CMV Retinitis (Immunocompromised)
- Most common opportunistic intraocular infection in AIDS (CD4 <50 cells/μL)
- Bilateral in 40% at presentation
- Painless, progressive necrotizing retinitis - "pizza pie" or "brushfire" appearance
- Hemorrhagic form: flame-shaped hemorrhages with white necrosis following vessels
- Granular form: Quieter, less hemorrhagic, more peripheral
- CMV anterior uveitis: Characteristic coin-shaped/endotheliitis KP - NOT seen in other herpetic conditions
- Treatment: Valganciclovir 900 mg BID x 3 weeks induction, then 900 mg daily maintenance; intravitreal ganciclovir/foscarnet for macular-threatening; HAART to restore CD4
Acute Retinal Necrosis (ARN)
- Caused by VZV (most common), HSV-1, HSV-2, CMV (in immunocompromised)
- Affects immunocompetent individuals
- Triad:
- Peripheral necrotizing retinitis (begins as multifocal white patches, then coalesces)
- Occlusive retinal arteritis
- Prominent vitritis
- Bilateral in 30-70% (contralateral eye involved weeks to months later - "sequential ARN")
- Retinal detachment risk: Up to 75% (due to multiple peripheral retinal breaks in necrotic tissue)
- Treatment: IV acyclovir 10-15 mg/kg TID x 10-14 days, then oral valacyclovir for months; prophylactic laser barrage around necrotic lesion to reduce RD risk
Progressive Outer Retinal Necrosis (PORN)
- Variant in severely immunocompromised (HIV, CD4 <50)
- VZV most common
- Outer retinal involvement, minimal or no vitritis, no retinal vasculitis
- Multifocal, rapidly confluent lesions
- Very poor prognosis
- Treat with IV acyclovir/ganciclovir + intravitreal injections; aggressive HAART
Tuberculosis Uveitis
- Any pattern possible; most common: posterior uveitis with choroidal granuloma
- Anterior: Mutton-fat KP, Busacca nodules, PS, iris granuloma
- Posterior: Serpiginous-like choroiditis (TB mimics serpiginous), choroidal granuloma, retinal vasculitis with candle-wax dripping periphlebitis (mimics sarcoidosis)
- Workup: IGRA (QuantiFERON-TB Gold) preferred over TST; CXR; CT chest
- Treatment: Standard anti-TB therapy (RIPE: Rifampicin + Isoniazid + Pyrazinamide + Ethambutol) x 9-12 months + systemic steroids for severe inflammation
Syphilitic Uveitis - "The Great Masquerader"
- Treponema pallidum - secondary syphilis causes most ocular manifestations
- Any pattern of uveitis; frequently granulomatous
- Classically: Bilateral interstitial keratitis + uveitis
- Chorioretinitis: "Salt and pepper" fundus; placoid chorioretinitis (APMPPE-like pattern)
- High index of suspicion; always test RPR + FTA-ABS (or treponemal-specific assay)
- Treatment: Penicillin G IV 18-24 million units/day x 10-14 days (same as neurosyphilis dosing for ocular disease)
PART 8 - WHITE DOT SYNDROMES & IDIOPATHIC CHORIORETINOPATHIES
These are a group of idiopathic inflammatory conditions primarily affecting the outer retina, RPE, and choriocapillaris. Most occur in young myopic women.
| Syndrome | Age/Sex | Laterality | Key Features | FA/OCT | Treatment |
|---|---|---|---|---|---|
| MEWDS | Young women | Unilateral | Flu-like prodrome, sudden vision loss, enlarged blind spot, foveal granularity | Early hypofluorescence, late hyperfluorescence; FAF hyperautofluorescence | Self-limited (4-6 weeks); no treatment |
| APMPPE | Young adults, M=F | Bilateral simultaneous | Rapid onset bilateral central visual loss; multifocal yellow-white placoid subretinal lesions | Early hypofluorescence, late hyperfluorescence (blocked + staining) | Self-limited; steroids for CNS involvement (cerebral vasculitis possible) |
| Serpiginous choroidopathy | Middle-aged, M>F | Bilateral, asymmetric | Peripapillary origin, geographic spreading in serpiginous pattern; central scotoma; recurrent | Active: early hypo, late hypo; healed: window defect; FAF: hyperAF in active | Systemic steroids + immunosuppression; high recurrence rate |
| Birdshot retinochoroidopathy | >40 years, White, F>M | Bilateral | Vitritis, cream-colored choroidal lesions in birdshot pattern, nyctalopia, color vision loss | ERG very helpful (progressive loss); HLA-A29 (96% positive) | Immunosuppression (cyclosporine, mycophenolate, methotrexate) |
| PIC (Punctate inner choroidopathy) | Young myopic women | Bilateral | Multiple small (<200μm) grey-yellow lesions at RPE level; no vitritis | OCT: outer retinal disruption; CNV in 25-40% | Steroids for active lesions; anti-VEGF for CNV |
| MFC (Multifocal choroiditis) | Young women, myopes | Bilateral | Larger lesions than PIC, mild vitritis present; "punched-out" scars | Similar to PIC | Steroids; treat CNV with anti-VEGF |
| AZOOR | Young women, myopes | Unilateral/bilateral | Enlarged blind spot, photopsia, outer retinal dysfunction; subtle fundus changes | FAF: extensive hyperAF in zone of dysfunction; ERG attenuated | Variable; some spontaneous recovery |
PART 9 - INVESTIGATIONS IN UVEITIS
Ocular Investigations
| Investigation | Best Use in Uveitis |
|---|---|
| FA (Fluorescein angiography) | Retinal vasculitis (early leakage), CME, disc swelling, ischemic/occlusive vasculopathy, chorioretinal atrophy (window defects) |
| ICGA (Indocyanine green angiography) | Choroidal inflammation (granulomas), VKH, birdshot, sarcoidosis - ICG shows choroidal lesions not visible on FA |
| OCT | CME monitoring, inner retinal infiltrates (Behcet, viral), outer retinal changes (PIC, MEWDS, APMPPE, serpiginous, AZOOR), choroidal granulomas (sarcoid, TB) |
| FAF (Fundus autofluorescence) | MEWDS (hyperAF), serpiginous (hyperAF in active), AZOOR (extensive hyperAF), VKH (serous detachment areas) |
| B-scan US | VKH (choroidal thickening, serous RD), scleritis, evaluate posterior segment when media opaque |
| ERG | Birdshot (progressive loss), AZOOR, monitoring |
| AC paracentesis (PCR) | Herpes virus uveitis (HSV, VZV, CMV), toxoplasmosis, suspected intraocular lymphoma |
| Vitreous biopsy (PPV) | Intraocular lymphoma, TB, fungi in atypical cases |
Systemic Investigations
| Test | When to Order |
|---|---|
| HLA-B27 | Acute unilateral/alternating anterior uveitis; hypopyon; suspicion of spondyloarthropathy |
| HLA-A29 | Birdshot retinochoroidopathy (96% sensitive) |
| HLA-B51 | Behcet disease |
| ANA | Suspected JIA, SLE; low specificity alone |
| ACE + serum lysozyme | Suspected sarcoidosis |
| RPR/VDRL + FTA-ABS | Always rule out syphilis |
| IGRA (QuantiFERON-TB Gold) | Suspected TB; preferred over TST in vaccinated populations |
| Toxoplasma IgG/IgM | Posterior uveitis with focal retinochoroiditis |
| CXR/CT chest | Sarcoidosis, TB |
| Sacroiliac X-ray / MRI spine | Suspected ankylosing spondylitis |
| ANCA | If associated with scleritis or PUK (c-ANCA for Wegener's) |
| Lyme serology | Endemic areas, intermediate uveitis |
| HIV serology | Opportunistic infections suspected |
| Chest CT | Sarcoidosis when CXR negative |
PART 10 - TREATMENT FRAMEWORK
Step-Up Approach to Uveitis Treatment
Step 1 - Local therapy (anterior/mild)
- Topical steroids: Prednisolone acetate 1% q1-6h (severe: q1h or loading dose); Difluprednate 0.05% (less frequent dosing)
- Cycloplegia: Cyclopentolate 1% TID (mild-moderate); Atropine 1% BID-QID (severe)
Step 2 - Periocular steroids
- Sub-Tenon triamcinolone 40 mg/mL (0.5-1 mL) - for unilateral posterior/intermediate uveitis not responding to topical; repeat q3-4 weeks if needed
- Use with extreme caution in scleritis (risk of scleral melting)
Step 3 - Systemic corticosteroids
- Prednisone 1 mg/kg/day for severe bilateral posterior/panuveitis
- High-dose IV methylprednisolone 1 g/day x 3 days for VKH, sympathetic ophthalmia
- Must supplement calcium + vitamin D (with long-term use)
Step 4 - Immunosuppressive (steroid-sparing) agents
| Agent | Primary Use |
|---|---|
| Methotrexate | JIA, sarcoidosis, intermediate uveitis; gold standard steroid-sparer |
| Azathioprine | VKH, Behcet, sarcoidosis |
| Mycophenolate mofetil | Birdshot, VKH, posterior uveitis |
| Cyclosporine | Birdshot, Behcet, VKH |
| Adalimumab (anti-TNF) | FDA-approved for non-infectious intermediate/posterior/panuveitis; JIA-uveitis |
| Infliximab | Behcet (severe ocular disease), JIA-uveitis; IV infusions |
| Tocilizumab | JIA-uveitis (anti-IL-6); refractory cases |
| Rituximab | Refractory non-infectious uveitis |
| Cyclophosphamide | Reserved for severe, sight-threatening refractory disease |
Note: Etanercept should be avoided in JIA-associated uveitis (can worsen inflammation).
Intravitreal Drug Delivery
- Triamcinolone (Kenalog): Useful for CME, intermediate/posterior uveitis (off-label)
- Ozurdex (dexamethasone implant): Biodegradable 0.7 mg implant; for CME and non-infectious uveitis
- Retisert (fluocinolone acetonide implant, 0.59 mg): Long-acting (2.5 years); placed surgically; high efficacy but ~50% develop elevated IOP, ~100% require cataract surgery
- Yutiq (fluocinolone acetonide 0.18 mg): Injectable implant; 3-year duration
- Ganciclovir/foscarnet intravitreal: For CMV retinitis
PART 11 - COMPLICATIONS OF UVEITIS
| Complication | Mechanism | Notes |
|---|---|---|
| Cataract | PSC type most common (steroid-induced or inflammatory) | Most common cause of VA loss; surgery should ideally be done in quiescent phase |
| Glaucoma | Trabecular block by cells/debris, PAS, pupillary block with PS + iris bombe | Inflammatory glaucoma; use beta-blockers/CAIs (avoid prostaglandins in active inflammation if possible) |
| Hypotony | Ciliary body shutdown (severe/chronic inflammation) | |
| Cystoid macular edema (CME) | Most common cause of VA loss in intermediate uveitis; breakdown of blood-retinal barrier | OCT and FA-guided treatment |
| Band keratopathy | Calcium deposition in Bowman's layer at palpebral fissure | Seen in JIA, chronic hypercalcemia; treat with EDTA chelation |
| Posterior synechiae | Iris adhesion to lens → pupillary block → iris bombe → angle closure | Prevent with cycloplegia; break acute PS with topical mydriatics |
| Phthisis bulbi | End-stage: hypotony, atrophy, calcification | |
| Choroidal neovascularization (CNV) | Disruption of Bruch's membrane + choroidal inflammation | PIC, multifocal choroiditis, VKH, POHS; treat with anti-VEGF |
| Epiretinal membrane | Especially in intermediate uveitis | |
| Retinal detachment | ARN (rhegmatogenous), VKH (exudative), Behcet (tractional) |
PART 12 - HIGH-YIELD EXAM ASSOCIATIONS
| Finding | Classic Association |
|---|---|
| Mutton-fat KP + Busacca nodules | Granulomatous (sarcoid, TB, VKH) |
| Coin-shaped KP | CMV anterior uveitis |
| Stellate KP throughout endothelium, no synechiae | Fuchs heterochromic iridocyclitis |
| Unilateral hypopyon | HLA-B27 (most common); also Behcet |
| Shifting hypopyon | Behcet disease |
| Snowbank + snowballs | Pars planitis (intermediate uveitis) |
| Headlight in the fog + old scar | Toxoplasma retinochoroiditis |
| Pizza pie/brushfire appearance | CMV retinitis (AIDS) |
| Candle-wax drippings periphlebitis | Sarcoidosis |
| Occlusive retinal vasculitis | Behcet disease |
| "Birdshot" choroidal spots + HLA-A29 | Birdshot retinochoroidopathy |
| Peripapillary geographic lesions | Serpiginous choroidopathy |
| Multifocal serous RD + sunset glow fundus | VKH syndrome |
| Dalen-Fuchs nodules | Sympathetic ophthalmia (also VKH) |
| Peripheral retinal necrosis + occlusive arteritis + vitritis | ARN syndrome |
| Outer retinal necrosis, no vitritis | PORN (immunocompromised) |
| Young myopic woman + acute vision loss + enlarged blind spot | MEWDS |
| Early and late hypofluorescence on FA + placoid lesions | APMPPE |
| JIA + ANA+ + chronic silent uveitis | JIA (oligoarticular) |
| Silk Road heritage + oral/genital ulcers + hypopyon | Behcet disease |
| Uveitis + deafness + vitiligo/poliosis/alopecia | VKH syndrome |
| Uveitis + nephritis (young female) | TINU syndrome |
| Uveitis + intermediate + MS | Intermediate uveitis / pars planitis |
PART 13 - MASQUERADE SYNDROMES
Always consider when uveitis is atypical, refractory, unilateral, or in older patients:
Neoplastic masquerades:
- Primary intraocular lymphoma (PIOL) - large B-cell; presents as intermediate uveitis in older patients; "vitreous snow globe"; diagnostic vitrectomy + IL-10:IL-6 ratio >1; MRI brain (CNS lymphoma)
- Leukemia/lymphoma: Hypopyon, vitreous cells
- Uveal melanoma: Vitritis overlying choroidal mass
- Retinoblastoma (children): Pseudohypopyon, white retinal lesion
- Metastatic disease: Choroidal deposits
Non-neoplastic masquerades:
- Rhegmatogenous RD (pigmented AC cells)
- Schwartz-Matsuo syndrome (RD + uveitis + raised IOP)
- Retained IOFB
- Retinitis pigmentosa (vitreous cells + CME + attenuated vessels + bone spicules)
- Asteroid hyalosis
- Amyloidosis (vitreous globules/membranes)
- Juvenile xanthogranuloma (JXG): spontaneous hyphema + anterior pseudouveitis in children
PART 14 - SPECIAL SITUATIONS
Pediatric Uveitis
- Screen all JIA patients: risk-stratified schedule based on JIA subtype, ANA status, age of onset, disease duration
- Routine tests in children: No test ordered routinely except as indicated; sarcoidosis and syphilis are less common in children
- At discharge from screening: warn self-monitoring (weekly monocular vision check) + annual optometry
Uveitis in HIV / Immunocompromised
- Opportunistic: CMV retinitis (CD4 <50), PORN (VZV), toxoplasma (CD4 <100), Cryptococcus, Pneumocystis
- IRIS (Immune Recovery Inflammatory Syndrome): Paradoxical worsening of CMV retinitis when HAART started; treat underlying CMV + consider brief steroids
Drug-Induced Uveitis
- Rifabutin: Hypopyon uveitis
- Cidofovir: Severe hypotony + uveitis
- Fluoroquinolones: Rare
- Bisphosphonates: Scleritis, anterior uveitis
- Immune checkpoint inhibitors (pembrolizumab, nivolumab): Severe uveitis, VKH-like reactions
REFERENCES
- Kanski's Clinical Ophthalmology: A Systematic Approach, 10th Edition (2024) - Chapter 12: Uveitis
- The Wills Eye Manual: Office and Emergency Room Diagnosis and Treatment of Eye Disease - Chapter 12: Uveitis
This guide covers the full spectrum from the basic SUN classification through to advanced topics including masquerade syndromes, white dot syndromes, and modern immunosuppressive regimens. For your final year exam and clinical practice, the most commonly tested areas are: the SUN classification system, KP interpretation, HLA associations, toxoplasma treatment regimen (with pyrimethamine monitoring), the JIA screening schedule, the VKH phases, ARN vs PORN distinction, and masquerade syndromes.
wait, i want to start from the basics include anatomy, physiology
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
I've exhausted my DB queries. I have Kanski's full anatomy/uveitis content from my previous session and my own foundational knowledge. Let me now deliver a comprehensive anatomy + physiology foundation before diving into uveitis.
UVEITIS - Complete Study Guide: Starting from ABSOLUTE BASICS
MODULE 1 - ANATOMY OF THE UVEAL TRACT
1.1 What is the Uvea?
The word "uvea" comes from the Latin uva (grape) - because the vascular coat of the eye, when stripped from the sclera, resembles a dark grape.
The uveal tract is the middle vascular coat of the eye, sandwiched between the outer fibrous coat (cornea + sclera) and the inner neural coat (retina).
It has three anatomically and functionally distinct parts:
UVEAL TRACT
├── IRIS → anterior uvea (diaphragm, controls pupil)
├── CILIARY BODY → anterior uvea (aqueous production + accommodation)
└── CHOROID → posterior uvea (nourishes outer retina)
1.2 The IRIS
Structure (anterior to posterior):
- Anterior border layer - incomplete layer of fibroblasts and melanocytes (no epithelium - this is why the iris can be seen through the cornea)
- Stroma - loose connective tissue with blood vessels, nerves, melanocytes, and the sphincter pupillae muscle
- Anterior pigment epithelium (APE) - contains the dilator pupillae muscle (myoepithelial cells)
- Posterior pigment epithelium (PPE) - densely pigmented; gives iris its black appearance from behind
Iris muscles:
- Sphincter pupillae: Circular, innervated by parasympathetic (CN III via ciliary ganglion) → miosis
- Dilator pupillae: Radial/myoepithelial, innervated by sympathetic (superior cervical ganglion, long ciliary nerves) → mydriasis
Blood supply:
- Major arterial circle of the iris (MACI): Formed by anastomosis of the two long posterior ciliary arteries (LPCA) and the anterior ciliary arteries (ACA) → located in the ciliary body at the iris root
- Minor arterial circle: Formed by branches from MACI at the collarette region
- Iris vessels are non-fenestrated → form the blood-aqueous barrier (BAB)
Collarette: The thickest part of the iris; divides the iris into pupillary zone (inner 1/3) and ciliary zone (outer 2/3)
Crypts of Fuchs: Normal depressions in the anterior border layer of the iris stroma
Iris color: Determined by the density of melanocytes in the anterior stroma (NOT the epithelium):
- Blue iris: Few anterior stromal melanocytes (posterior epithelium always dark)
- Brown iris: Dense anterior stromal melanocytes
1.3 The CILIARY BODY
Location: Ring-shaped structure extending from the scleral spur anteriorly to the ora serrata posteriorly
Two Parts:
- Pars plicata (anterior, 2 mm): Contains ~70 ciliary processes; produces aqueous humor
- Pars plana (posterior, 4 mm): Flat, avascular; surgical access zone (pars plana vitrectomy)
Layers (outer to inner):
- Supraciliary space (potential space between sclera and ciliary body)
- Ciliary muscle (smooth muscle)
- Vascular layer (stroma with vessels)
- Ciliary processes
- Double-layered ciliary epithelium (outer pigmented + inner non-pigmented)
Ciliary Muscle - Three Parts:
| Fiber orientation | Name | Function |
|---|---|---|
| Longitudinal (meridional) | Brücke's muscle | Pulls ciliary body forward; opens trabecular spaces |
| Radial | Radial fibers | Intermediate |
| Circular (sphincteric) | Müller's ciliary muscle | Accommodation (most important for near focus) |
Innervation: Parasympathetic (CN III → ciliary ganglion → short ciliary nerves) → contraction for accommodation; sympathetic → relaxation
Blood supply: Long posterior ciliary arteries (LPCA) + anterior ciliary arteries (ACA) → major arterial circle of iris
Zonules of Zinn (Zonular fibers):
- Fine fibrils connecting ciliary processes to the lens capsule (equatorial region)
- Composed of fibrillin (mutations → Marfan syndrome → lens subluxation)
- When ciliary muscle contracts (accommodation) → zonules relax → lens becomes more convex → near focus
- When ciliary muscle relaxes (distant vision) → zonules taut → lens flattened
1.4 The CHOROID
The choroid is the largest and most vascular structure in the uveal tract, occupying the posterior 2/3 of the eye.
Layers (inner to outer):
- Bruch's membrane (Lamina vitrea): 5-layered membrane between RPE and choriocapillaris
- Inner: RPE basement membrane
- Inner collagenous zone
- Elastic layer
- Outer collagenous zone
- Outer: Choriocapillaris basement membrane
- Choriocapillaris: Innermost capillary layer; highly fenestrated (allows nutrients to reach RPE and outer retina)
- Sattler's layer: Medium-sized vessels (arterioles and venules)
- Haller's layer: Large choroidal vessels (branches of short posterior ciliary arteries)
- Suprachoroidal space: Potential space between choroid and sclera; important for drug delivery
Blood supply:
- Short posterior ciliary arteries (SPCA): ~15-20 branches from the ophthalmic artery; pierce the sclera around the optic nerve; supply the entire choroid
- Long posterior ciliary arteries (LPCA): 2 vessels; enter nasally and temporally; travel to the ciliary body
- Choroidal blood flow is among the highest per unit tissue in the body (~800 mL/100g/min)
- Drainage via vortex veins (4-6 veins draining into superior and inferior ophthalmic veins)
Function:
- Nourishes the outer retina (RPE + outer nuclear layer + photoreceptors)
- Thermoregulation (heat sink)
- Secretion of growth factors
- Immune privilege (see below)
Suprachoroidal space separates choroid from sclera; relevant in:
- Suprachoroidal hemorrhage (after glaucoma surgery, trauma)
- Drug delivery (suprachoroidal injections - e.g., triamcinolone for uveitis)
1.5 Vascular Supply of the Uvea - Summary
Ophthalmic artery (branch of ICA)
│
├── Central retinal artery → inner retina
│
├── Short posterior ciliary arteries (SPCA) × 15-20
│ └── Choroid (all of it)
│
├── Long posterior ciliary arteries (LPCA) × 2
│ └── Travel to ciliary body → Major arterial circle of iris
│ ├── Iris (via minor arterial circle)
│ └── Ciliary body (pars plicata)
│
└── Anterior ciliary arteries (ACA) × 7
└── Perforating branches join MACI
Venous drainage: All uveal blood drains via 4-6 vortex veins → superior/inferior ophthalmic veins → cavernous sinus
1.6 Nerve Supply of the Uvea
| Nerve | Origin | Function |
|---|---|---|
| Short ciliary nerves (8-10 branches) | Ciliary ganglion (post-ganglionic parasympathetic) | Sphincter pupillae (miosis), ciliary muscle (accommodation), sensory to cornea/uvea |
| Long ciliary nerves (2-3) | Nasociliary nerve (CN V1) via sympathetic root + sensory fibers | Dilator pupillae (mydriasis), sensory from iris/cornea |
| Parasympathetic root | CN III → ciliary ganglion | Pre-ganglionic; synapse in ciliary ganglion |
| Sympathetic root | Superior cervical ganglion → internal carotid → ophthalmic | Passes through ciliary ganglion without synapse; to dilator |
Why uveitis causes pain: Iris and ciliary body are richly innervated by sensory fibers. Inflammation stimulates these nociceptors → ciliary spasm → deep, aching orbital pain. That's why cycloplegia relieves pain and breaks synechiae.
MODULE 2 - PHYSIOLOGY RELEVANT TO UVEITIS
2.1 Aqueous Humor - Production and Circulation
Where: Produced by the non-pigmented ciliary epithelium of the pars plicata
Mechanisms of production (in order of importance):
- Active secretion (~80-90%): Na⁺/K⁺-ATPase dependent; carbonic anhydrase-dependent bicarbonate secretion; accounts for most of normal IOP
- Ultrafiltration (~10-20%): Pressure-dependent passive movement of plasma
- Simple diffusion: Minor
Composition: Similar to plasma but with:
- Very low protein (0.02 g/dL vs plasma 7 g/dL) → important for clarity
- Higher ascorbate (antioxidant)
- Lower glucose
- Higher bicarbonate
Aqueous circulation pathway:
Ciliary processes (pars plicata)
↓
Posterior chamber (behind iris)
↓
Through pupil
↓
Anterior chamber
↓ (main route, 85-90%)
Trabecular meshwork → Schlemm's canal → collector channels → episcleral veins
↓ (uveoscleral / accessory route, 10-15%)
Anterior face of ciliary muscle → supraciliary / suprachoroidal space → scleral vessels
In uveitis: Breakdown of the blood-aqueous barrier (BAB) → proteins and cells leak into aqueous → flare and cells → can block trabecular meshwork → raised IOP
2.2 The Blood-Ocular Barrier (BOB)
This is the single most important physiological concept underpinning uveitis.
Two components:
A. Blood-Aqueous Barrier (BAB) - Anterior
| Structure | Cell type | Tight junction protein |
|---|---|---|
| Iris blood vessels | Non-fenestrated endothelium | Occludin, claudins, ZO-1 |
| Non-pigmented ciliary epithelium | Non-pigmented cells | Occludin, claudins |
When BAB breaks down → proteins enter aqueous → flare on slit lamp; cells enter → cells in AC
B. Blood-Retinal Barrier (BRB) - Posterior
| Structure | Layer | Tight junction |
|---|---|---|
| Retinal capillaries (inner BRB) | Non-fenestrated endothelium | Occludin, claudins |
| Retinal pigment epithelium (outer BRB) | RPE tight junctions | ZO-1, occludin |
When BRB breaks down → retinal edema, CME, subretinal fluid, disc leakage
What breaks the BOB in uveitis?:
- Prostaglandins (especially PGE2): Potent vasodilators; increase vascular permeability; produced by inflamed uveal cells
- Histamine: Early mediator; from mast cells
- VEGF: Breaks inner and outer BRB
- Cytokines (IL-1β, IL-6, TNF-α): Downregulate tight junction proteins
- Complement activation
- Immune complex deposition
This is why NSAIDs (topical/systemic) work in uveitis - they inhibit cyclooxygenase → reduce prostaglandin synthesis → restore BAB
2.3 Ocular Immune Privilege
The eye is one of the immune-privileged sites in the body (along with the brain, testes, and placenta).
Definition: The eye tolerates the presence of antigens (including grafts) with reduced inflammatory/immune response compared to other body sites.
Mechanisms (you must know all of these):
| Mechanism | Detail |
|---|---|
| Blood-ocular barrier | Limits entry of circulating immune cells and complement |
| Aqueous humor contains immunosuppressive factors | TGF-β2, α-MSH, CGRP, VIP, somatostatin, free cortisol → suppress T cell activation and NK cells |
| Anterior chamber-associated immune deviation (ACAID) | Antigens introduced into AC generate systemic tolerance (Treg-mediated suppression) rather than inflammatory immunity |
| Fas-FasL (CD95-CD95L) | Corneal endothelium, iris, ciliary body, RPE express FasL → induces apoptosis of infiltrating Fas+ T cells and neutrophils |
| Complement regulatory proteins | DAF, CD59, MCP on ocular cells → inhibit complement activation |
| HLA expression | Very low MHC class I/II on corneal endothelium, lens; limits antigen presentation |
| VEGF and neurotrophins | VEGF maintains corneal avascularity; NGF supports regulatory T cells |
| Vitreous | Contains TGF-β2; suppresses T cell proliferation |
Why immune privilege breaks down in uveitis:
- Breakdown of BOB → effector T cells enter
- Loss of TGF-β2 production
- Upregulation of MHC class II on uveal cells → they become antigen-presenting cells
- Molecular mimicry: Microbial antigens (Chlamydia, Klebsiella in HLA-B27) share epitopes with ocular proteins (e.g., HLA-B27 and retinal S-antigen) → cross-reactive T cells attack uveal tissue
- Autoimmune attack on uveal melanocytes (VKH, sympathetic ophthalmia)
2.4 Immunology of Uveitis - The Immune Cascade
Understanding this is essential for understanding why immunosuppressives work.
Step 1 - Antigen presentation:
- Antigen (microbial or self-protein) is processed by macrophages/dendritic cells
- Presented on MHC class II → activates CD4+ T helper cells
- Presented on MHC class I → activates CD8+ cytotoxic T cells
Step 2 - T cell activation and differentiation:
| T cell subset | Cytokines produced | Role in uveitis |
|---|---|---|
| Th1 | IFN-γ, IL-2, TNF-α | Drives granulomatous inflammation (sarcoid, TB, VKH) |
| Th2 | IL-4, IL-5, IL-13 | Allergic/humoral responses; less dominant in uveitis |
| Th17 | IL-17, IL-22, IL-21 | Drives acute non-granulomatous inflammation (HLA-B27, Behcet) |
| Treg (FoxP3+) | TGF-β, IL-10 | Suppresses inflammation; key in ACAID |
IL-6 is a pivotal cytokine: released by macrophages/monocytes → drives Th17 differentiation → perpetuates uveitis. This is why tocilizumab (anti-IL-6) works in JIA-uveitis.
TNF-α: Master pro-inflammatory cytokine; produced by macrophages → activates endothelium → recruits more leukocytes. This is why anti-TNF agents (adalimumab, infliximab) are effective.
Step 3 - Leukocyte recruitment and tissue damage:
- Selectins and integrins on endothelium → rolling and adhesion of leukocytes
- Chemokines (CXCL10, CXCL5) → migration through BOB
- Neutrophils: Early, acute inflammation → hypopyon (dead neutrophils)
- Macrophages: Phagocytosis, antigen presentation, granuloma formation
- Plasma cells: Antibody production → immune complex deposition → complement activation
2.5 Aqueous Flare - The Physiology Behind the Sign
Normal aqueous protein: ~0.02 g/dL
Inflamed aqueous protein: Can rise to 3-4 g/dL (approaching plasma levels)
When protein leaks into the AC → the normally invisible aqueous beam of the slit lamp becomes visible (Tyndall effect - light scatters off protein particles) → this is flare
Flare ≠ active inflammation necessarily: Chronic, "burnt-out" uveitis with permanent BOB damage can show persistent flare without active cells. The cell count is the true indicator of active inflammation.
Cells in the AC: Are white blood cells (primarily lymphocytes and monocytes in chronic uveitis; neutrophils in acute HLA-B27, Behcet). They are seen as bright moving dots in the slit lamp beam.
2.6 Keratic Precipitates (KP) - Formation
KP = deposits on the posterior surface of the corneal endothelium
Why do they form?
- Inflammatory cells (lymphocytes, macrophages, plasma cells) + fibrin deposit on the endothelium
- Driven by aqueous convection currents (warm aqueous rises centrally, cools and descends laterally)
- This creates the Arlt's triangle distribution (base down, apex up)
Types and their composition:
- Fine KP: Mainly lymphocytes (small cells); seen in viral uveitis (HSV, VZV, CMV) and FHC
- Medium KP: Mix of lymphocytes and macrophages
- Mutton-fat KP: Epithelioid macrophages + giant cells + lymphocytes; seen in granulomatous uveitis (sarcoid, TB, VKH); appear large, greasy, white-grey
CMV coin-shaped KP: Unique endotheliitis pattern where CMV directly infects endothelial cells → localized round deposits; NOT in triangle pattern
KP location/distribution:
- Arlt's triangle (inferior): Classical
- Stellate throughout endothelium: Fuchs heterochromic iridocyclitis
- Coin-shaped/sectoral: CMV
- Posterior (on posterior capsule): After cataract surgery
MODULE 3 - WHY THE UVEA IS SO SUSCEPTIBLE TO INFLAMMATION
The uveal tract is the most common site of intraocular inflammation for several reasons:
- Richest blood supply in the body per unit tissue → More circulating immune cells can access it
- Slow blood flow in the choroid + sinusoidal choriocapillaris → Antigens and immune complexes tend to be deposited here (like kidneys)
- Rich in melanocytes → Melanocyte-associated antigens (retinal S-antigen, IRBP) can trigger autoimmunity in genetically predisposed individuals
- Breakdown of immune privilege → Once BOB breached, a self-perpetuating inflammatory cycle starts
- Molecular mimicry → Microbial peptides share structural similarity with uveal proteins → cross-reactive T cells attack the uvea
- HLA associations → Certain HLA types present uveal antigens more effectively to autoreactive T cells (HLA-B27, HLA-A29, HLA-DR4)
MODULE 4 - RETINAL PIGMENT EPITHELIUM (RPE) AND ITS ROLE IN UVEITIS
The RPE (single layer of hexagonal pigmented cells between photoreceptors and Bruch's membrane) is a key participant in uveitis:
Normal functions:
- Phagocytosis of shed photoreceptor outer segments
- Vitamin A (retinol) recycling (visual cycle)
- Maintenance of outer BRB
- Secretion of VEGF (supports choriocapillaris)
- Secretion of immunosuppressive factors (TGF-β, CTNF)
- Pump fluid from subretinal space
In uveitis:
- RPE becomes an antigen-presenting cell (upregulates MHC II)
- Produces pro-inflammatory cytokines when activated
- Disrupted outer BRB → subretinal fluid accumulates (as in VKH)
- RPE atrophy → "window defects" on FA, "sunset glow" fundus in VKH
- Dalen-Fuchs nodules (sympathetic ophthalmia/VKH): Focal accumulations of RPE cells + macrophages between Bruch's membrane and RPE
MODULE 5 - PUTTING IT TOGETHER: From Anatomy to Uveitis
Here's the logical chain from anatomy/physiology to clinical uveitis:
TRIGGER
(infection / autoimmune / trauma / drugs)
│
▼
Antigen presentation by macrophages/dendritic cells
│
▼
T cell activation (Th1 → granulomatous; Th17 → non-granulomatous)
│
▼
Cytokine release (TNF-α, IL-1β, IL-6, IL-17, prostaglandins, VEGF)
│
▼
Breakdown of Blood-Ocular Barrier
│
┌────┴────────────────┐
▼ ▼
Blood-Aqueous Blood-Retinal
Barrier Barrier
│ │
▼ ▼
Cells + flare in AC CME, disc edema,
KP on endothelium subretinal fluid,
Posterior synechiae retinal infiltrates
Hypopyon Vasculitis
│
▼
COMPLICATIONS
(cataract, glaucoma, band keratopathy, hypotony, phthisis)
QUICK ANATOMY RECALL TABLE
| Structure | Layer | Blood supply | Key function |
|---|---|---|---|
| Iris stroma | Anterior uvea | Minor arterial circle (from MACI) | Pupil, BAB |
| Pars plicata | Anterior uvea (ciliary body) | MACI (LPCA + ACA) | Aqueous production, accommodation |
| Pars plana | Anterior uvea (ciliary body) | MACI | Surgical access zone |
| Choroid | Posterior uvea | SPCA (from ophthalmic artery) | Outer retinal nutrition |
| Choriocapillaris | Innermost choroid | SPCA | Fenestrated; nourishes RPE/photoreceptors |
| RPE | Between retina and choroid | Choriocapillaris | Outer BRB, phagocytosis, visual cycle |
| Bruch's membrane | Between RPE and choriocapillaris | - | Structural support; CNV breaks through |
Now that you have this foundational anatomy and physiology layer, everything in the clinical uveitis guide (from the previous response) will make much more sense:
- Why mutton-fat KP are granulomatous: Macrophages accumulate because Th1 cytokines recruit them to form granulomas
- Why cycloplegia relieves pain: Paralysis of ciliary muscle (richly innervated by CN V sensory fibers) reduces ciliary spasm
- Why serous RDs occur in VKH: Autoimmune attack on choroidal melanocytes → choroidal granulomas → disruption of RPE tight junctions → outer BRB breakdown → fluid accumulation in subretinal space
- Why adalimumab works: TNF-α inhibition → reduces leukocyte recruitment and BAB breakdown
- Why the choroid is the most affected site in systemic diseases (sarcoid, TB, VKH): Its fenestrated choriocapillaris allows antigen/immune complex deposition, much like the kidney glomerulus
The previous clinical guide covering classification, specific entities, treatment, and masquerades forms the next layer on top of this foundation.
- Kanski's Clinical Ophthalmology: A Systematic Approach, 10th Edition - Chapters on uveitis, anterior segment anatomy, choroid
- The Wills Eye Manual - Chapter 12: Uveitis
This is a shared conversation. Sign in to Orris to start your own chat.