Inj mgso4 and kesol syrup
Reading File
Finding Sources
Searching the Web
Kesol syrup potassium chloride uses dose
Reading File
Finding Sources
Reading Web Page
https://www.1mg.com/otc/kesol-syrup-otc256565
Reading File
Reading File
Here is a complete clinical overview of both drugs:
Inj. Magnesium Sulfate (MgSO4)
Drug Class
Magnesium salt / electrolyte / anticonvulsant / tocolytic
Available Formulations
- Injection: 500 mg/mL (4 mEq/mL) - must be diluted before use
- Prediluted IV solutions: 40 mg/mL, 80 mg/mL (in sterile water); 10 mg/mL (in D5W)
- Oral granules (Epsom salts): ~40 mEq Mg per 5 g
Equivalence: 500 mg MgSO4 = 49.3 mg elemental Mg = 4.1 mEq Mg 9.9% elemental magnesium
Indications & Doses
| Indication | Dose |
|---|---|
| Hypomagnesemia / Hypocalcemia | 25-50 mg/kg/dose IV/IM Q4-6 hr x 3-4 doses; max single dose 2 g |
| Oral (hypomagnesemia) | 100-200 mg/kg/dose QID PO |
| Asthma / Reactive airway (child) | 25-75 mg/kg/dose (max 2 g) x 1 IV over 20 min |
| Asthma / Reactive airway (adult) | 2 g x 1 IV over 20 min |
| Parenteral nutrition maintenance | 30-60 mg/kg/24 hr IV; max 1 g/24 hr |
| Cathartic (child) | 0.25 g/kg/dose PO Q4-6 hr |
| Cathartic (adult) | 10-30 g/dose PO Q4-6 hr |
| Tetanus (autonomic dysfunction) | Maintain plasma level 2-4 mmol/L IV |
Max IV Infusion Rates
- Emergent: 1 mEq/kg/hr (125 mg/kg/hr)
- Asymptomatic hypomagnesemia: 0.1 mEq/kg/hr (12.5 mg/kg/hr)
Toxicity (Serum Level Dependent)
| Level | Effect |
|---|---|
| >3 mg/dL | CNS depression |
| >5 mg/dL | Decreased deep tendon reflexes, flushing, somnolence |
| >12 mg/dL | Respiratory paralysis, heart block |
Key Warnings
- IV administration risk: hypotension, bradycardia, respiratory depression, complete heart block, hypermagnesemia
- Antidote: Calcium gluconate IV - must be kept available
- Use caution in renal insufficiency (monitor Mg levels)
- Use caution with digoxin
- Pregnancy category A (doses up to 400 mg/24 hr); category D if used >5-7 days for preterm labor (neonatal hypocalcemia, osteopenia, fractures reported)
Kesol Syrup (Potassium Chloride 20% Oral Solution)
Drug Class
Electrolyte supplement - potassium replenishment
Formulation
- KCl 20% oral solution (Potassium Chloride Oral Solution USP)
- Manufacturer: Eisen Pharmaceutical Co. Pvt. Ltd. (Pune)
- Available as sugar-free, raspberry-flavoured solution (200 mL bottle)
Indication
Treatment and prevention of hypokalemia (low serum potassium)
Dose
- Standard oral dose: 40-100 mmol/day of KCl
- Typical: 1 teaspoonful (5 mL) THREE times a day with meals
- Must be diluted in water or juice before administration to reduce GI irritation
- Dose adjusted based on severity and ongoing losses
Clinical Use Context
- Oral KCl is preferred over IV whenever feasible
- If K+ > 3 mEq/L: oral replacement sufficient
- If K+ < 3 mEq/L or symptomatic: may need IV KCl in a monitored setting
- Chloride salt is preferred as it also corrects concomitant metabolic alkalosis
- Avoid glucose-containing solutions alongside KCl (insulin-mediated intracellular shift worsens hypokalemia)
- If hypomagnesemia is present, it must be corrected as well - magnesium depletion causes ongoing urinary K+ wasting
Side Effects
- GI irritation (nausea, vomiting, diarrhea) - give with food and diluted
- Hyperkalemia if overdosed (especially in renal impairment)
- Cardiac arrhythmias (with rapid or excessive dosing)
Contraindications / Cautions
- Renal impairment (risk of hyperkalemia)
- High-risk patients (elderly, liver disease, cardiac disturbances) need monitoring
- IV KCl rate must not exceed 10-20 mmol/hour for standard patients; use monitored setting for higher rates
Clinical Note - These Two Drugs Together
These two are commonly co-prescribed because hypomagnesemia and hypokalemia frequently coexist. Magnesium deficiency causes persistent urinary potassium wasting, so replacing potassium alone (with Kesol) without correcting low magnesium (with Inj. MgSO4) will result in refractory hypokalemia. Correcting Mg first or simultaneously is standard practice.
Sources: - The Harriet Lane Handbook 23rd ed. | Goldman-Cecil Medicine International Edition
Achlasia Cardia
Reading File
Finding Sources
Searching the Web
achalasia cardia pathophysiology management 2024 guidelines
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Here is a comprehensive clinical overview of Achalasia Cardia:
Achalasia Cardia
Definition
Achalasia is a primary esophageal motility disorder characterized by:
- Impaired lower esophageal sphincter (LES) relaxation with swallowing
- Aperistalsis in the smooth muscle esophagus
The name "achalasia" comes from Greek, meaning "failure to relax."
Pathophysiology
The underlying defect is neurogenic degeneration of the myenteric (Auerbach) plexus in the smooth muscle segment of the esophagus and LES.
Key changes:
- Loss of ganglion cells, surrounded by mononuclear inflammatory infiltrate (cytotoxic T cells - suggesting autoimmune etiology in genetically susceptible individuals)
- The degree of ganglion cell loss parallels disease duration
- Inhibitory neurons (using NO and VIP as neurotransmitters) are predominantly lost - these are responsible for LES relaxation and deglutitive inhibition
- Result: unopposed excitatory (cholinergic) tone keeps the LES contracted; no peristaltic propagation in the esophageal body
- Achalasia esophagus lacks NO synthase and shows marked reduction of VIP-staining neurons at the GEJ
- CCK paradoxically increases LES pressure in achalasia (normally it relaxes the LES via inhibitory neurons)
Disease Progression:
EGJ outflow obstruction → Type II achalasia → Type I achalasia → End-stage (sigmoid esophagus)
Chicago Classification - HRM Subtypes
| Type | Manometric Pattern | Key Feature |
|---|---|---|
| Type I (Classic) | No pressurization; aperistalsis | Low intraesophageal pressure; dilated, atonic esophagus |
| Type II | Pan-esophageal pressurization | Compartmentalized pressurization; best treatment response |
| Type III (Spastic) | Premature/spastic contractions | Unique pathogenesis; myenteric inflammation but not destruction |
Clinical Features
Symptoms:
- Dysphagia - universal; affects both solids AND liquids (hallmark - distinguishes from mechanical obstruction which starts with solids only)
- Regurgitation - of undigested food from hours/days earlier; nonbilious, nonacid, mixed with saliva
- Chest pain - present in ~2/3 of patients early in disease; may spontaneously improve over time (thought to be from esophageal spasm)
- Hiccups, halitosis
- Weight loss
- Aspiration pneumonia - in up to 10% of advanced cases
- Apparent "heartburn" - actually from fermentation of retained food, NOT true GERD; ambulatory pH studies show no discrete reflux events
Important Note: 29% of patients with achalasia are misdiagnosed as GERD and treated with PPIs for an average of 29 months before the correct diagnosis is made.
Investigations
1. Endoscopy (EGD) - First test
- Normal in ~40% of patients
- Retained food, saliva, stasis esophagitis, or Candida infection in others
- Tight, "puckered" GEJ - pops open with gentle pressure (distinguishes from malignancy)
- Mandatory to rule out pseudoachalasia (carcinoma at GEJ)
2. Barium Swallow
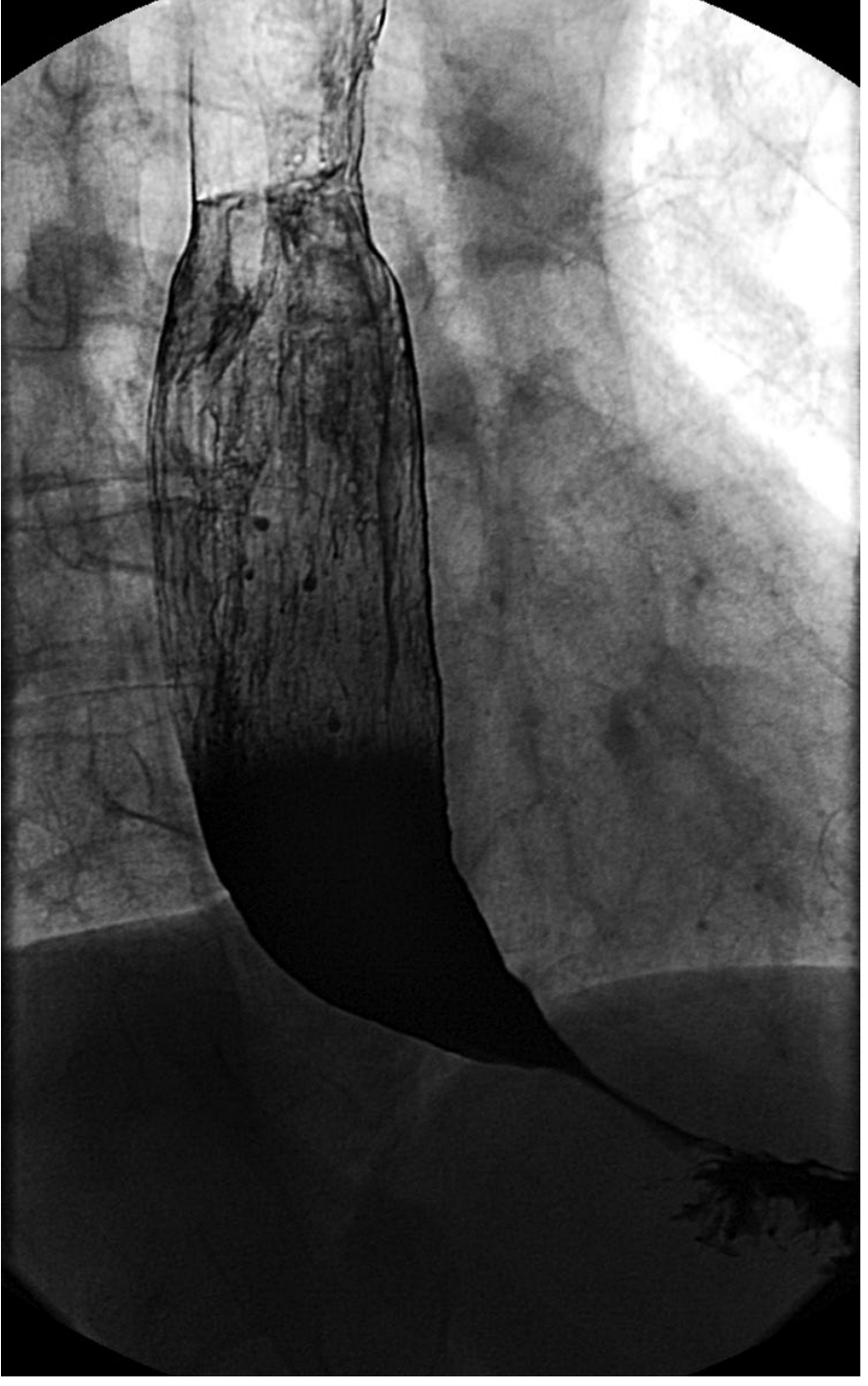
Barium swallow in achalasia: dilated esophagus with distal narrowing, air-fluid level, slow emptying, tertiary contractions
- Classic finding: "Bird-beak" or "rat-tail" appearance at the GEJ
- Dilated esophagus, air-fluid level
- Slow/absent emptying of contrast into stomach
- Tertiary contractions
- Normal in ~30% of early cases
- Important: defines esophageal axis (straight vs. sigmoid) for surgical planning
3. High-Resolution Esophageal Manometry (HRM) - Gold Standard
- Elevated LES resting pressure (>45 mmHg)
- Absent or incomplete LES relaxation (elevated integrated relaxation pressure - IRP)
- Aperistalsis in the esophageal body
- Defines subtype (I, II, or III) - critical for treatment selection
4. Ambulatory pH Monitoring
- Reserved for patients complaining of heartburn
- Differentiates true GERD from fermentative acidification
5. EndoFLIP (Functional Lumen Imaging Probe) - Newer tool
- Measures EGJ distensibility
- Useful when HRM is inconclusive; shows reduced EGJ distensibility in achalasia
Treatment
Since the underlying neuropathology cannot be reversed, all treatment aims to reduce LES pressure to improve esophageal emptying by gravity.
1. Pharmacologic (Temporizing only)
| Drug | Mechanism | Notes |
|---|---|---|
| Isosorbide dinitrate (sublingual) | Smooth muscle relaxant - reduces LES pressure | Limited efficacy; headache common |
| Nifedipine 30-40 mg/day sublingual before meals | Calcium channel blocker | Good in 70% short-term; placebo crossover showed minimal benefit |
| Sildenafil 50 mg | PDE-5 inhibitor → ↑ cGMP → NO-mediated relaxation | Peak at 15-20 min, lasts <1 hr; limited practical use |
2. Botulinum Toxin Injection (Endoscopic)
- 80 units injected into 4 quadrants of LES via sclerotherapy catheter
- Mechanism: blocks ACh release from presynaptic cholinergic terminals
- 66% improve at 6 months; minimal efficacy at 1 year
- Repeat injections cause fibrosis - limits future myotomy
- Best reserved for elderly/frail patients who are poor surgical candidates
- Doses >100 units do not improve efficacy
3. Pneumatic Dilation (PD)
- Requires dilation to ≥3 cm diameter to disrupt LES circular muscle
- Rigiflex balloons: 3.0, 3.5, and 4.0 cm sizes - passed over guidewire fluoroscopically
- Outpatient procedure under conscious sedation
- Risk of esophageal perforation: ~1%
- Overall efficacy ~90%
- Type II achalasia: 100% response with PD vs. 93% with Heller myotomy
- Type III achalasia: Only 40% success with PD (vs. 86% with myotomy)
4. Laparoscopic Heller Myotomy (LHM)
- Division of LES circular muscle fibers
- Usually combined with partial fundoplication (Dor or Toupet) to prevent post-op reflux
- Overall ~90% efficacy
- Best for Type III achalasia
- Both LHM and PD are comparably effective for Types I and II
5. Per-Oral Endoscopic Myotomy (POEM) - Modern preferred option
- Endoscopic submucosal tunnel technique
- 92% clinical remission at 1 year vs. 70% with PD (p < 0.01)
- More effective than LHM for Type III achalasia (longer myotomy extends into esophageal body)
- Major limitation: very high incidence of pathological reflux (OR 9.31 for erosive esophagitis compared to LHM)
- 2024 SAGES guidelines updated recommendations for POEM use
6. Esophageal Resection (Last resort)
- Reserved for end-stage/refractory achalasia
- Indications: unresolvable obstruction, malnutrition, chronic aspiration, perforation during dilation, cancer, mega-esophagus
- Gastric pull-up or colon/small bowel interposition
- Mortality ~4%
Treatment Selection by Subtype
| Subtype | Preferred Treatment |
|---|---|
| Type I | PD or LHM or POEM (comparable) |
| Type II | Pneumatic dilation preferred (100% efficacy); POEM also excellent |
| Type III | POEM or LHM (PD only 40% effective) |
| Elderly/frail | Botulinum toxin injection |
Complications
- Aspiration pneumonia - from nocturnal regurgitation
- Squamous cell carcinoma - 17x increased risk vs. age-matched controls; develops in dilated, stasis-affected esophagus. Incidence ~0.15%/year
- Candida esophagitis - from stasis
- Airway compromise - rare; dilated esophagus compresses membranous trachea
- Esophageal perforation - ~1% risk with pneumatic dilation
- Post-treatment GERD - especially after POEM
Pseudoachalasia
Must always be excluded - carcinoma of the GEJ can mimic achalasia clinically and manometrically. Endoscopy + CT are mandatory. Clues to pseudoachalasia: age >60, weight loss >15 lbs, symptom onset <6 months, suboptimal response to dilation.
Sources: - Sleisenger and Fordtran's Gastrointestinal and Liver Disease | Sabiston Textbook of Surgery 8th ed. | Current Surgical Therapy 14th ed.
This is a shared conversation. Sign in to Orris to start your own chat.