Shoulder joint biomechanics in detail
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Finding Sources
Finding Sources
Reading File
Finding Sources
Loading Image
Loading Image
Searching the Web
shoulder joint biomechanics glenohumeral stability kinematics force couples
I now have comprehensive material from multiple authoritative sources. Let me compile the full detailed answer.
Shoulder Joint Biomechanics
The shoulder is the most mobile joint in the human body, achieving this range of motion through a carefully coordinated interplay of four articulations, multiple stabilizing mechanisms, and precisely balanced muscle force couples. Understanding its biomechanics requires examining each component systematically.
1. The Four Articulations
The "shoulder joint" is not a single joint but a functional complex of four articulations that work in concert:
| Articulation | Type | Primary Function |
|---|---|---|
| Glenohumeral (GH) | Ball-and-socket synovial | Main motion joint; largest ROM |
| Scapulothoracic (ST) | Functional (not true synovial) | Scapular positioning and rotation |
| Acromioclavicular (AC) | Diarthrodial | Clavicle-scapula coupling |
| Sternoclavicular (SC) | Diarthrodial saddle | Axial skeleton linkage |
Together, they allow the shoulder to have the greatest range of motion of any joint in the body, and the relationship between these articulations must be considered when treating shoulder dysfunction.
- Campbell's Operative Orthopaedics 15th Ed 2026
2. Bony Architecture and the Stability-Mobility Trade-Off
The glenohumeral joint operates on a fundamental mechanical compromise: a large humeral head articulating with a shallow glenoid fossa - commonly compared to a golf ball on a tee.
Key dimensions:
- The glenoid articular surface creates a socket approximately 9 mm deep in the superoinferior direction and 5 mm deep in the anteroposterior direction
- The glenoid labrum (fibrocartilaginous rim) increases glenoid depth by 50%
- With the labrum, glenoid surface coverage extends to 75% of the humeral head vertically and 57% horizontally
- Biomechanical cadaveric testing confirms the labrum significantly alters the distribution of contact stresses when a compressive load is applied at 90 degrees of abduction
Because bony constraint is minimal, stability is primarily provided by the surrounding soft tissues - muscles, ligaments, and capsule.
- Campbell's Operative Orthopaedics 15th Ed 2026
Humeral head geometry: The humeral head is retroverted approximately 20-30 degrees relative to the shaft axis and tilted 130-150 degrees in inclination. This retroversion matches the anteversion/retroversion range of the glenoid and contributes to bony congruency during arm use.
3. Kinematics - Range of Motion
The Scapular Plane
The scapular plane is the preferred reference for shoulder kinematics. It is positioned 30 degrees anterior to the coronal plane and oriented perpendicular to the glenoid face. Motions in this plane are more natural and less likely to produce impingement because:
- The capsule and ligaments are in a neutral (non-twisted) state
- The deltoid and rotator cuff fibers are in optimal alignment
- The greater tuberosity clears the acromion more easily
Glenohumeral Motion
| Motion | ROM | Primary Muscles |
|---|---|---|
| Abduction | 120° GH + 60° ST = 180° total | Deltoid + supraspinatus |
| Forward flexion | 120-180° | Pectoralis major, anterior deltoid, biceps |
| Extension | ~60° | Latissimus dorsi |
| Internal rotation | 60-90° | Subscapularis, teres major |
| External rotation | 60-90° | Infraspinatus, teres minor, posterior deltoid |
| Adduction | 45-75° | Latissimus dorsi, pectoralis major, teres major |
Important note: Full abduction requires external rotation of the humerus to allow the greater tuberosity to rotate posteriorly and clear the coracoacromial arch. With internal rotation contractures, abduction is limited to approximately 120 degrees.
- Miller's Review of Orthopaedics 9th Edition
4. Scapulohumeral Rhythm
One of the most important kinematic concepts in shoulder biomechanics.
Definition: The coordinated, synchronous motion at the glenohumeral and scapulothoracic joints during arm elevation.
The 2:1 Ratio:
- For every 3 degrees of arm elevation, the glenohumeral joint contributes 2 degrees and the scapulothoracic joint contributes 1 degree
- Overall: 120 degrees GH + 60 degrees ST = 180 degrees total elevation
- This ratio is not constant throughout the arc - the first 30 degrees of motion shows variable contributions before the rhythm is established
Above 90 degrees: The proportion of scapulothoracic motion relative to glenohumeral motion increases progressively.
Clinical significance: Disturbance of normal scapulohumeral rhythm affects the biomechanics of the shoulder and may result in secondary impingement. This is the basis of "scapular dyskinesis."
- Rheumatology, 2-Volume Set (2022, Elsevier); Imaging Anatomy Atlas Vol.3
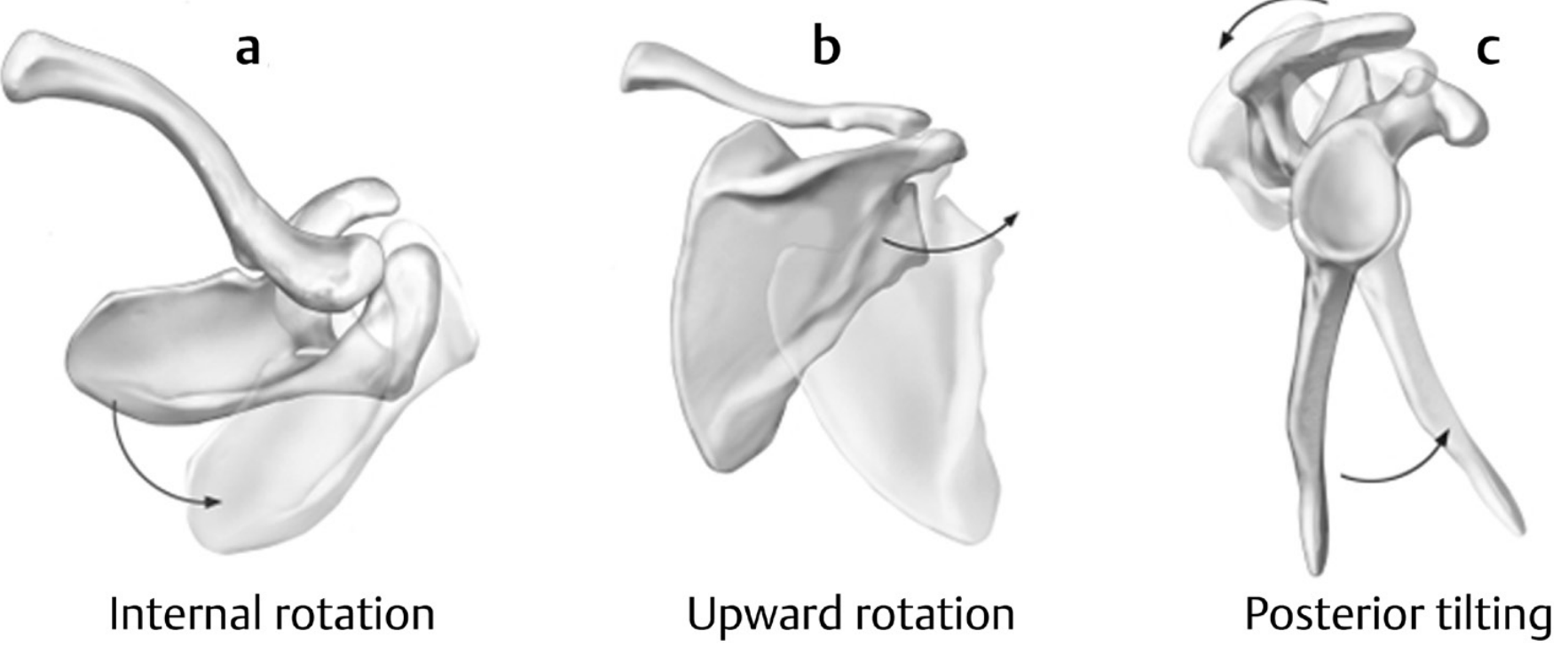
Scapular motions during arm elevation - Imaging Anatomy Atlas Vol.3
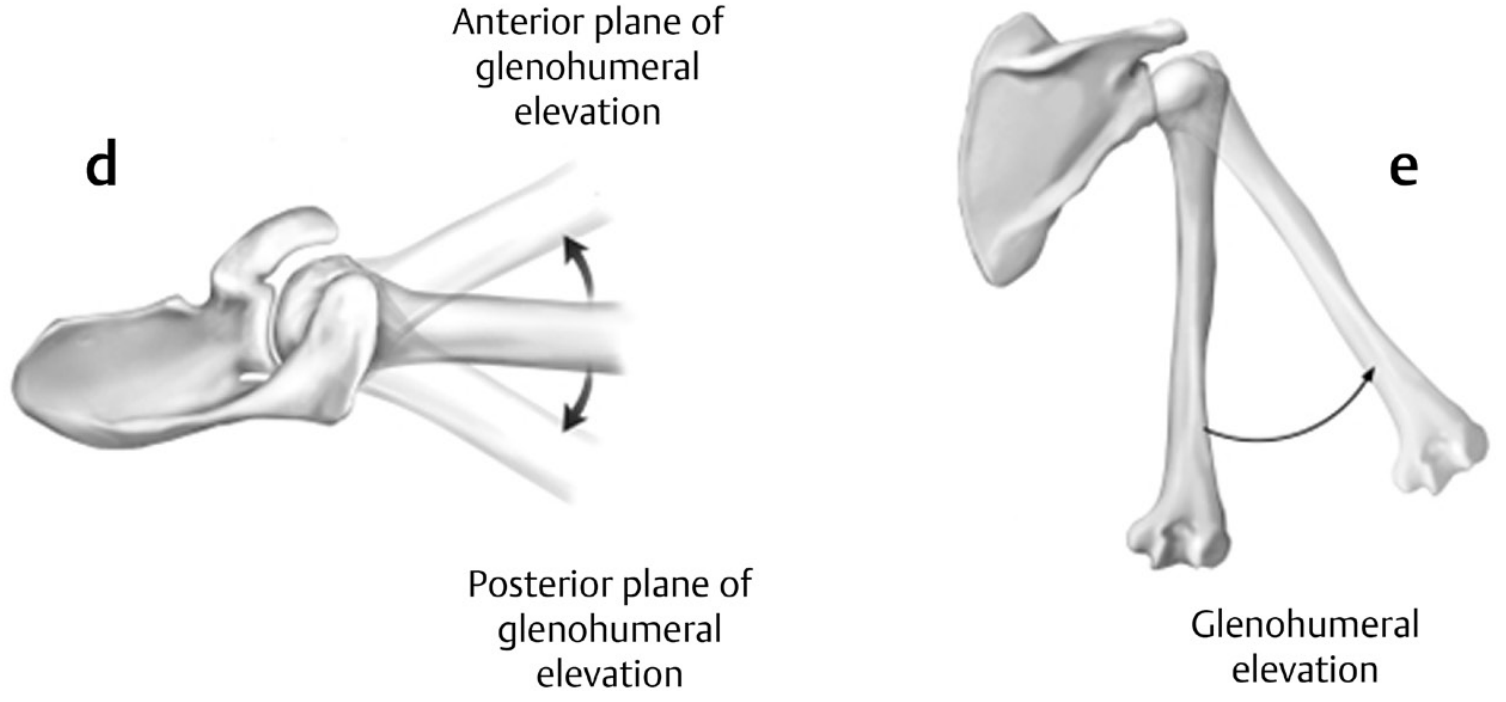
Planes of glenohumeral elevation - Imaging Anatomy Atlas Vol.3
5. Periscapular Joint Contributions
Sternoclavicular (SC) Joint
- A diarthrodial saddle joint containing an intraarticular disc
- Stabilized by posterior ligaments (primary AP restraint), anterior ligaments (primary restraint to superior displacement), and the costoclavicular ligament
- Motions: Clavicular elevation/depression (~35° arc), protraction/retraction (~35°), and posterior rotation around the long axis (~50° during full arm elevation)
- Couples posterior rotation of the clavicle with scapular upward rotation
Acromioclavicular (AC) Joint
- Stabilized by the AC ligament capsule (anteroposterior stability) and coracoclavicular ligaments (conoid and trapezoid)
- Conoid fibers are vertical; trapezoid fibers are nearly horizontal
- Both restrict superior clavicle migration; trapezoid resists posterior/lateral clavicular displacement
- Scapular motions at this joint: anterior/posterior tilting, internal/external rotation, upward/downward rotation
Scapulothoracic "Joint"
- Not a true synovial joint - a functional articulation between the scapula and thoracic wall formed by muscular attachments
- Primary motions: upward/downward rotation (glenoid moves up/down), anterior/posterior tilting, internal/external rotation, protraction/retraction
- Imaging Anatomy Atlas Vol.3
6. Static Stabilizers
6a. Glenohumeral Ligaments
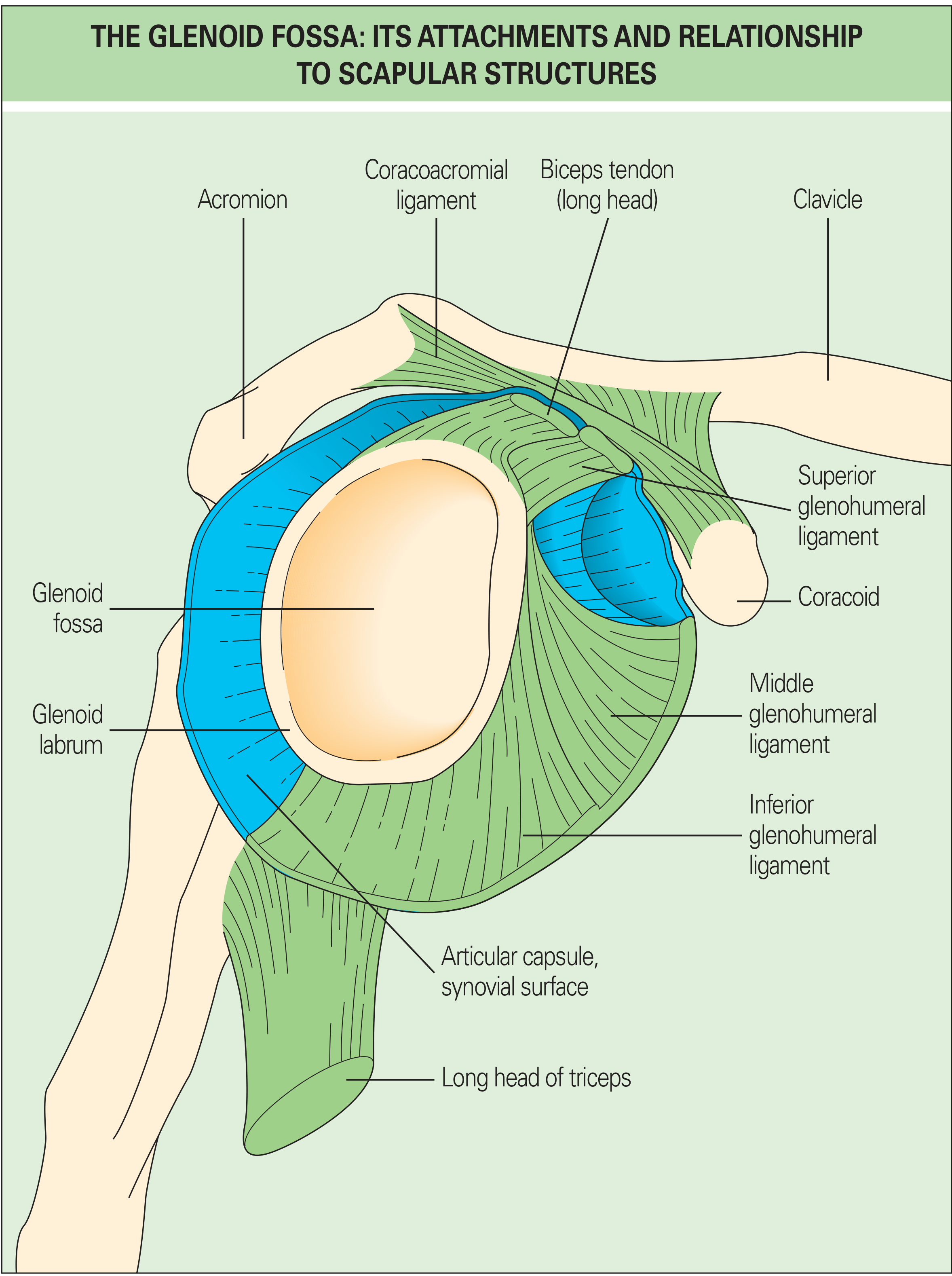
Glenoid fossa attachments - Rheumatology (Elsevier, 2022)
| Ligament | Primary Role |
|---|---|
| Superior GHL (SGHL) | Primary restraint to inferior subluxation at 0° abduction; primary stabilizer to anterior/posterior stress at 0° |
| Middle GHL (MGHL) | Limits external rotation at lower and middle ranges of abduction; minimal effect at 90° |
| Inferior GHL (IGHL) - anterior band | Primary stabilizer to anterior/posterior stress at ≥45° abduction - the most important ligamentous stabilizer |
| Inferior GHL - posterior band | Posterior stability in external rotation |
| Coracohumeral ligament (CHL) | Resistance to inferior displacement; part of the "rotator interval" |
Inferior GHL Hammock Mechanism: The IGHL complex forms a "hammock-type sling" around the inferior humeral head:
- With external rotation: anterior band tightens, posterior band fans out; hammock slides anteriorly and superiorly
- With internal rotation: the opposite occurs
- This is why anterior instability classically occurs in the abduction-external rotation (ABER) position
Rotator interval: Tightening of the rotator interval (SGHL + CHL) decreases posterior and inferior translation. The "comma sign" - a comma-shaped arc at the superolateral subscapularis insertion - consists of approximately 54% SGHL and 46% CHL and serves as a surgical landmark.
- Campbell's Operative Orthopaedics 15th Ed 2026
6b. Glenoid Labrum
- Dense fibrocartilaginous ring around the glenoid rim
- Forms a tight seal creating negative intra-articular pressure (suction effect) - a critical passive stabilizer
- Increases glenoid depth (see Section 2)
- Thicker cartilage at the glenoid periphery also adds to stability
6c. Joint Capsule
- Voluminous - does not restrict movement until extremes of motion
- Provides stability at end-range
- Ligament becomes taut as the humerus rotates in direction opposite to the ligament's position relative to the center of rotation
7. Dynamic Stabilizers and Force Couples
This is perhaps the most important concept in shoulder biomechanics for understanding function and pathology.
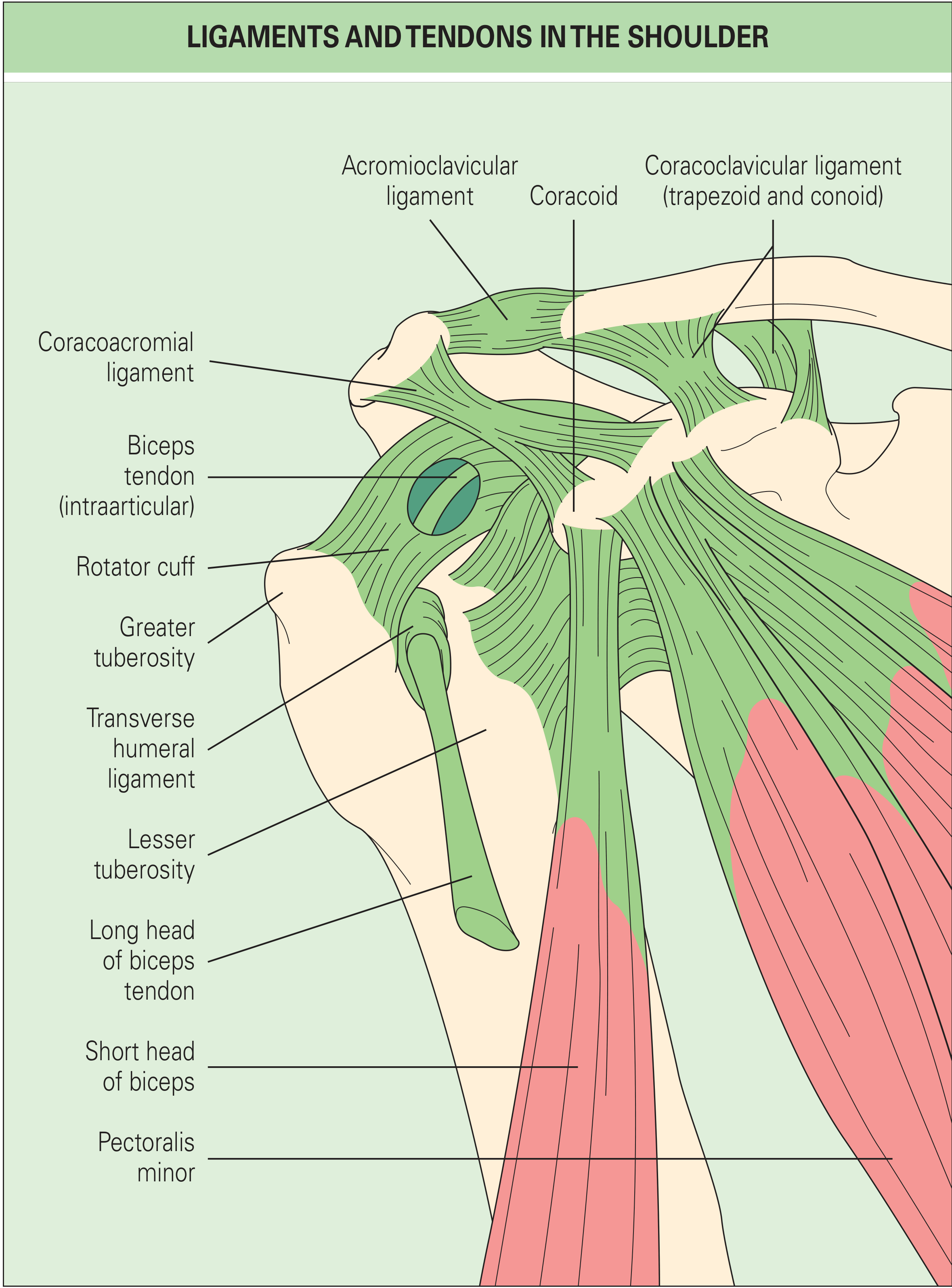
Ligaments and tendons of the shoulder - Rheumatology (Elsevier, 2022)
The Rotator Cuff: SITS Muscles
| Muscle | Action | Stability Role |
|---|---|---|
| Supraspinatus | Abduction initiator | Superior compressive force on humeral head |
| Infraspinatus | External rotation | Posterior compressive force; clears greater tuberosity in abduction |
| Teres minor | External rotation | Posterior inferior compressive force; important when other cuff tendons fail |
| Subscapularis | Internal rotation | Anterior compressive force; key member of transverse force couple |
Concavity Compression: The rotator cuff tendons act not just as rotators but - when acting together - compress the humeral head against the glenoid concavity. This mechanism ("concavity compression") keeps the humeral head centered in the glenoid throughout the arc of motion, providing dynamic mid-range stability where ligaments are lax.
The Two Force Couples
Force Couple 1 - Coronal Plane (Abduction force couple):
- Deltoid (superior force, tends to translate head superiorly) vs. Rotator cuff inferior fibers (inferior force, depresses the head)
- The rotator cuff acts as a force depressor to counterbalance the superior shear of the deltoid
- This is why an intact rotator cuff is required for effective deltoid-driven abduction
- A massive superior rotator cuff tear disrupts this couple, but some patients retain overhead function when the subscapularis-posterior cuff couple remains intact
Force Couple 2 - Transverse (Horizontal) Plane:
- Subscapularis (anterior) vs. Infraspinatus + Teres minor (posterior)
- Together, these provide a compressive force that centers the humeral head in the glenoid in the horizontal plane
- This explains why some patients with massive superior cuff tears retain reasonable function - as long as this transverse couple is intact
Scapular Force Couple:
- Upper trapezius (superior rotational force on clavicle and scapula) + Serratus anterior (inferior rotational force pulling the inferior scapular angle laterally) combine to produce upward rotation of the scapula during arm elevation
- Lower trapezius acts to depress the clavicle and further assist upward rotation
- This couple is critical for maintaining the glenoid beneath the humeral head as the arm rises - like a "ball on a seal's nose" (Rowe analogy)
Muscle Classification
Extrinsic muscles (control scapular position): Rhomboids, levator scapulae, trapezius, serratus anterior
Intrinsic muscles (control glenohumeral motion): Rotator cuff (×4), deltoid, pectoralis major, teres major, latissimus dorsi, biceps brachii
Muscle contributions to stability operate through three mechanisms:
- Dynamic scapular positioning - keeps the glenoid opposite the humeral head as the shoulder moves
- Capsular stiffening - muscle activity increases capsular stiffness and reduces glenohumeral translation
- Fine-tuning via force couples - directing forces through the joint to maintain the instant center of rotation
8. The Coracoacromial Arch and Subacromial Space
The subacromial space is only a few millimeters wide and contains:
- Long head of the biceps tendon
- Rotator cuff (especially supraspinatus)
- Subacromial bursa
The coracoacromial arch (acromion + coracoacromial ligament + coracoid) forms the ceiling of this space. During abduction, the rotator cuff and subacromial structures pass beneath this arch. Superior translation of the humeral head (from rotator cuff weakness, imbalance, or capsular tightness) reduces this space and causes impingement. The coracoacromial arch also acts as the superior restraint to humeral head translation (limiting superior subluxation when the rotator cuff is torn).
9. Kinetics - Joint Reaction Forces
The shoulder experiences significant compressive forces during activity:
- During abduction at 90°, the joint reaction force is approximately 0.89 × body weight just from arm weight
- Forces in overhead activities of daily living regularly exceed body weight
- The compressive force needed to resist superior translation during overhead work is generated almost entirely by the rotator cuff
- During throwing, the glenohumeral joint endures peak forces of 1,090 N (compressive) at late cocking, with significant distraction forces during deceleration
Shoulder arthrodesis position (optimal positioning to allow function if the joint must be fused): 15-20° abduction, 20-25° forward flexion, 40-50° internal rotation.
- Miller's Review of Orthopaedics 9th Edition
10. Clinical Biomechanical Correlates
| Condition | Biomechanical Basis |
|---|---|
| Supraspinatus tear | Loss of superior compressive force; disrupts coronal force couple; superior humeral migration |
| Subscapularis tear | Loss of anterior stabilizer of transverse force couple; anterior instability |
| Anterior dislocation | Failure of IGHL anterior band in ABER position; Bankart lesion/Hill-Sachs |
| Subacromial impingement | Superior humeral migration (reduced rotator cuff compression); disturbed scapulohumeral rhythm; decreased subacromial space |
| Scapular dyskinesis | Disrupted scapulothoracic rhythm; glenoid not properly positioned under humeral head; secondary impingement |
| SLAP tear | Labral failure; loss of suction effect; reduced glenoid depth; biceps anchor destabilization |
| Frozen shoulder | Capsular contracture - especially posterior and inferior capsule; restricted gliding; shifted center of rotation |
Summary
The shoulder achieves its extraordinary mobility through a deliberate trade-off: minimal bony constraint is compensated for by layered active and passive stabilizers. The glenohumeral joint relies on the labrum (suction/depth), capsulolabral ligaments (end-range restraint), rotator cuff concavity compression (mid-range dynamic stability), and precisely balanced force couples (continuous centering of the humeral head). The scapulothoracic articulation - coordinated via the trapezius-serratus anterior force couple - keeps the glenoid properly oriented throughout elevation, maintaining the 2:1 scapulohumeral rhythm. Disruption at any point in this chain - whether bony, ligamentous, or muscular - typically has biomechanical consequences that cascade through the entire system.
Sources:
- Campbell's Operative Orthopaedics, 15th Ed 2026
- Miller's Review of Orthopaedics, 9th Edition
- Imaging Anatomy Atlas Vol. 3 - Bones, Joints, Vessels and Nerves (THIEME)
- Rheumatology, 2-Volume Set (Elsevier, 2022)
This is a shared conversation. Sign in to Orris to start your own chat.