Takayasu arteritis
Reading File
Finding Sources
Searching PubMed
"Takayasu arteritis"[MeSH Terms] AND management
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Reading File
Reading File
I now have comprehensive information. Let me compile the full detailed answer.
Takayasu Arteritis (TA)
Also known as pulseless disease or aortic arch syndrome, Takayasu arteritis is a granulomatous large-vessel vasculitis primarily affecting the aorta and its major branches. It is a panarteritis - involving all three layers of the vessel wall.
Epidemiology
- Predominantly affects young women (female:male ratio up to 9-10:1)
- Median onset age: 25 years; ~25% begin before age 20
- Most prevalent in Japan, China, India, and Southeast Asia (Japan: ~150/million/year vs. 8-25/million in Western Europe/North America)
- HLA associations: HLA-Bw52, Dw12, DR2, and DQw1 in Japanese patients; different associations in Korean and Indian populations
- Non-HLA susceptibility loci identified: SVEP1, CFL2, VPS8, chr13q21
- In Mexican patients, prior exposure to Mycobacterium tuberculosis has been implicated
- Firestein & Kelley's Textbook of Rheumatology, p. 1973
Pathogenesis
The disease results from an autoimmune process targeting large elastic-containing arteries. The key immunopathological features include:
- Panarteritis with infiltration of dendritic cells, T cells (αβ, γδ, and cytotoxic), NK cells, and macrophages
- The majority of lymphocytes are perforin-secreting killer lymphocytes (T cells and NK cells)
- T cell receptors are oligoclonal, suggesting response to a specific but unknown antigen
- Growth factor-driven mesenchymal cell proliferation leads to intimal hyperplasia, fibrosis, and arterial stenosis or occlusion
- Local matrix metalloproteinase synthesis predisposes to aneurysmal dilation
- Chronic inflammation leads to aneurysm formation, stenosis, or thrombosis - more frequently than in GCA
TA and GCA are now thought to represent a disease spectrum with nearly identical pathology - differentiated primarily by age at onset (TA: <50 years; GCA: ≥50 years).
- Robbins, Cotran & Kumar Pathologic Basis of Disease; Braunwald's Heart Disease
Morphology / Histopathology
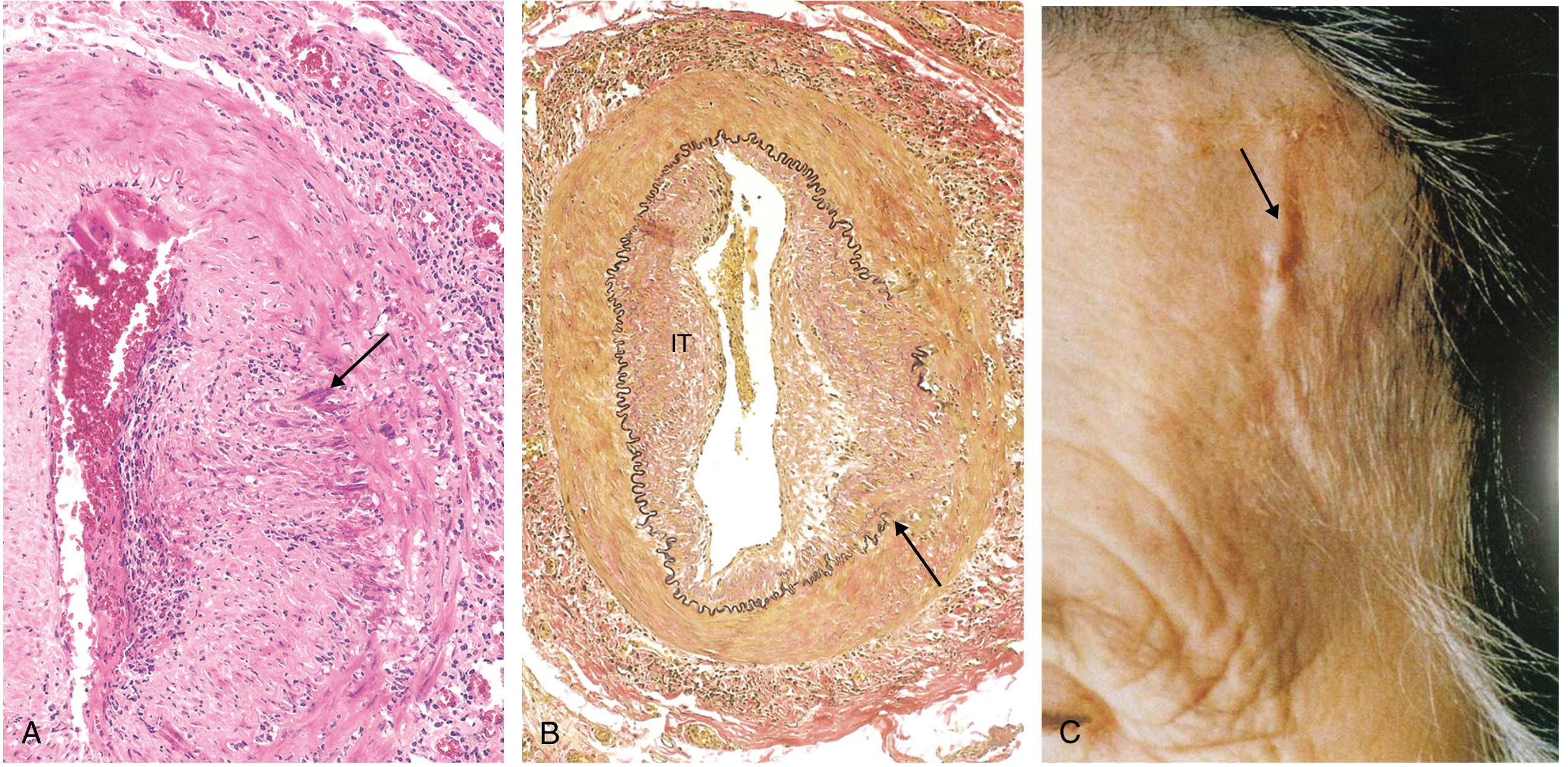
Histopathology: (A) granulomatous inflammation with giant cells; (B) intimal thickening (IT) with preserved but distorted internal elastic lamina
- Irregular thickening of the vessel wall with intimal hyperplasia
- Histology ranges from adventitial mononuclear infiltrates and perivascular cuffing of vasa vasorum → to intense mononuclear inflammation in the media → to granulomatous inflammation with giant cells and patchy medial necrosis
- As disease progresses: collagenous scarring with chronic inflammatory infiltrates in all three layers
- Late phase: intimal proliferation with superimposed atherosclerosis, medial necrosis with scarring, adventitial fibrosis
- Aortic root involvement can cause dilation and aortic valve insufficiency
- Robbins Pathology, p. 482; Braunwald's Heart Disease, p. 1162
Vascular Distribution
The most commonly affected vessels:
| Vessel | Frequency |
|---|---|
| Left subclavian artery | 93% |
| Aorta (any segment) | 65% |
| Carotid arteries | common |
| Renal arteries | common |
| Vertebral arteries | common |
| Pulmonary arteries | up to 50% |
-
90% have stenotic/occlusive lesions; ~25% have aneurysms
- 53% of patients have lesions both above and below the diaphragm
- Lesion types: stenotic (93%), occluded (57%), dilated (16%), aneurysmal (7%)
- Stenotic lesions are ~4x more common than aneurysmal
Numano/Lupi-Herrera Angiographic Classification (Types I-VI) categorizes involvement from isolated aortic arch disease to combined thoracoabdominal involvement.
Clinical Features
Phase 1 - Pre-pulseless (Systemic/Inflammatory Phase)
Nonspecific systemic symptoms:
- Fever, night sweats, malaise, fatigue, weight loss
- Arthralgia/myalgia
- Elevated ESR and CRP
Phase 2 - Pulseless (Occlusive/Vascular Phase)
Vascular symptoms dominate (full table below):
| Feature | At Presentation (%) | Ever Present (%) |
|---|---|---|
| Vascular signs | 50 | 100 |
| Bruit | - | 80 |
| Upper limb claudication | 30 | 62 |
| Lower limb claudication | 15 | 32 |
| Hypertension | 20 | 33 |
| Unequal arm BP (>10 mmHg) | 15 | 50 |
| Carotidynia | 15 | 32 |
| Aortic regurgitation | - | 20 |
| CNS symptoms | 30 | 57 |
| Lightheadedness/syncope | 20 | 35 |
| Visual abnormality | 10 | 30 |
| Stroke | 5 | 10 |
| Constitutional | 33 | 43 |
- Firestein & Kelley's Textbook of Rheumatology, Table 89.9
Key physical findings:
- Absent or diminished radial/carotid pulses ("pulseless disease")
- Blood pressure discrepancy between arms (>10 mmHg is significant)
- Subclavian or aortic bruit
- Carotidynia (tenderness over carotid arteries, up to 25%)
Cutaneous manifestations (in <10% of patients):
- Erythema nodosum (most common)
- Pyoderma gangrenosum-like ulcerations (well described in Japan, often precede diagnosis by ~3 years, predominantly upper extremities)
- Livedo reticularis, purpura
- Sweet syndrome (reported association)
Pregnancy: Higher risk of gestational hypertension, pre-eclampsia, and eclampsia. Tight BP control and correction of renal artery stenosis are important.
ACR Classification Criteria (1990, updated 2022)
ACR 1990 Criteria (≥3 of 6 = sensitivity 90.5%, specificity 97.8%):
- Onset before age 40 years
- Limb claudication
- Decreased brachial artery pulse
- Unequal arm blood pressure (>10 mmHg)
- Subclavian or aortic bruit
- Angiographic evidence of narrowing/occlusion of aorta or its primary branches or large limb arteries
The ACR/EULAR 2022 updated criteria incorporate imaging findings more formally and reflect a broader patient population.
- Firestein & Kelley's Textbook of Rheumatology, Table 89.8
Investigations
Laboratory:
- Elevated ESR and CRP (active disease)
- Normochromic normocytic anemia
- Raised platelet count
- No specific serologic marker; ANA/ANCA typically negative
Imaging (comparison below):
| Technique | Advantages | Disadvantages |
|---|---|---|
| Conventional angiography | "Gold standard" image quality; allows angioplasty at same time | Invasive; radiation; cannot visualize vessel wall |
| MRA | Excellent quality; noninvasive; no radiation; visualizes vessel wall thickness | Not gold standard; pacemaker contraindication |
| CTA | Excellent image quality | Radiation; IV contrast; cannot measure wall |
| Ultrasonography | Noninvasive; can visualize vessel wall edema | Operator-dependent; obesity limitation |
| ¹⁸F-FDG-PET | Measures vascular inflammation intensity | Radiation; poor vascular anatomy; IV contrast |
- Firestein & Kelley's Textbook of Rheumatology, Table 89.10
MRA is now preferred for initial and follow-up imaging. PET-CT can detect early active arteritis before luminal changes appear but notably does not always correlate with clinical and MRI disease activity in TA.
Imaging Examples
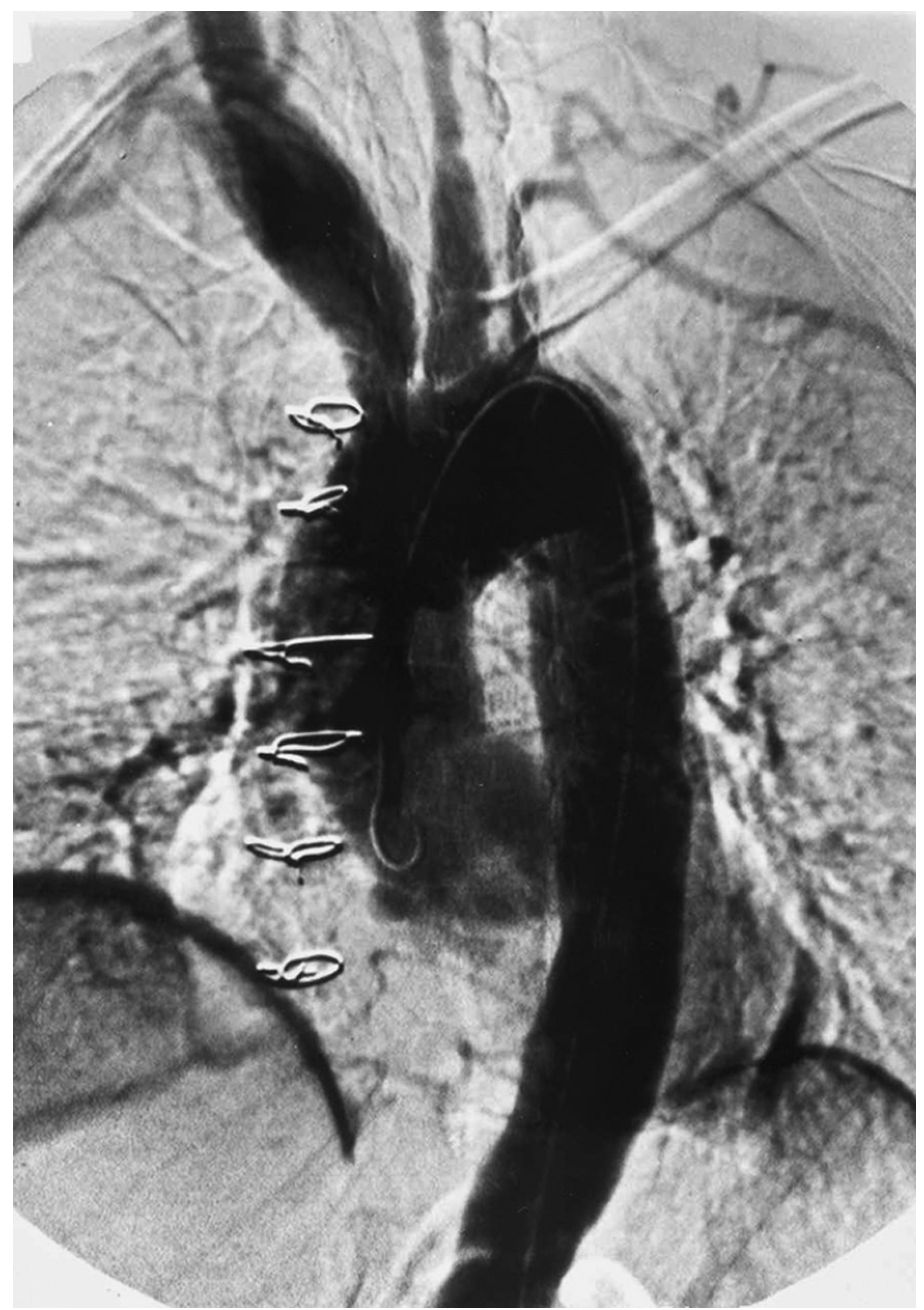
Conventional angiogram showing multiple TA changes including aortic root dilation, aneurysmal dilation of innominate artery, and occlusion of distal left common carotid. (From Firestein & Kelley's, Fig. 89.11)

MRI sagittal section showing thickening of the ascending and descending thoracic aorta in a 26-year-old woman with TA. (From Firestein & Kelley's, Fig. 89.12)
Differential Diagnosis
- Giant cell arteritis (GCA) - most difficult to distinguish; primary differentiator is age <50 (TA) vs ≥50 (GCA)
- Cogan's syndrome (keratitis + vestibuloauditory dysfunction)
- Syphilitic aortitis (exclude with FTA-ABS)
- Atherosclerosis
- IgG4-related disease
- Inflammatory bowel disease-associated vasculitis
- Sarcoidosis, radiation-induced arteritis, Behçet's disease
- Congenital coarctation, Marfan's syndrome, Ehlers-Danlos
Treatment
Glucocorticoids (First-line)
- Prednisone 1 mg/kg/day (Andrews' Diseases of the Skin recommends tapering over 8-12 weeks to ≤20 mg/day)
- ~85% of patients present with active disease
- Initial dose continued 4-12 weeks before gradual taper
- ~two-thirds achieve remission, but >half later relapse
- Relapses especially common when prednisone falls below 20 mg/day
- 86% of patients experience glucocorticoid-related adverse events at 10-year follow-up
Steroid-sparing Agents
- Methotrexate: 0.3 mg/kg/week (start ≤15 mg/week, increase to 25 mg/week) - moderately effective; most patients still need 5-10 mg/day prednisone
- Azathioprine: 2 mg/kg/day
- Mycophenolate mofetil: 2000 mg/day
- Cyclosporine, leflunomide
Biologic Therapies (Refractory Disease)
- Anti-TNF agents: Infliximab (5 mg/kg IV), etanercept - effective but rarely curative; relapses common on stopping
- Tocilizumab (IL-6 receptor antagonist): effective in individual patients, but a small RCT (n=18) showed no effect on time-to-relapse vs. placebo; disease progression masked by normalized inflammatory markers has been reported
- Tofacitinib (JAK inhibitor): emerging evidence showing higher complete remission rates at 6 and 12 months vs. methotrexate, lower relapse rates, longer relapse-free survival
- Rituximab: used in refractory cases (also for IgG4-related disease)
- Abatacept, ustekinumab: suggested as potential options
- Firestein & Kelley's, p. 1976; Andrews' Diseases of the Skin
Surgical / Endovascular Interventions
- Percutaneous transluminal angioplasty (PTA) for significant stenoses
- Bypass surgery for critical occlusions
- Aortic valve and root replacement if significant aortic regurgitation
- Important: Ideally perform during disease remission to reduce restenosis risk
- Coronary ostial stenosis may require coronary artery bypass grafting
Prognosis
- 15-year survival: >95% overall (Japan 96.5%; US 94-96%)
- Survival falls to 67% in patients with serious complications or progressive disease
- 74% report compromised daily activities; 23% unable to work
- 10-year survival in Korea: 87%
Recent Evidence (2024-2025)
A 2025 systematic review and meta-analysis on biologic therapies for large vessel vasculitis (PMID 40063878) evaluated the role of biologics including anti-TNF and anti-IL-6 agents. A 2025 systematic review on anti-TNF and anti-IL-6 treatments specifically for pediatric TA (PMID 40531440) addressed the therapeutic dilemma in children. A 2025 meta-analysis on angiographic types of TA (PMID 40982119) analyzed prevalence and clinical severity by Numano classification type. These recent papers suggest biologic therapies are increasingly established in refractory disease but optimal sequencing remains under investigation.
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease (p. 482); Firestein & Kelley's Textbook of Rheumatology (pp. 1973-1977); Braunwald's Heart Disease (pp. 1162-1165); Andrews' Diseases of the Skin Clinical Dermatology
This is a shared conversation. Sign in to Orris to start your own chat.