Hi
Hi! How can I help you today?
Uterine supports. Form shaw text book
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Here is a complete, organized answer on Uterine Supports based on standard gynecology textbook content (as covered in Shaw's and Berek & Novak's Gynecology):
Uterine Supports
The uterus is maintained in its normal anteverted-anteflexed position in the pelvis by a combination of ligamentous supports, muscular supports (pelvic floor), and the angle of the vaginal axis. These are broadly classified as:
Diagram
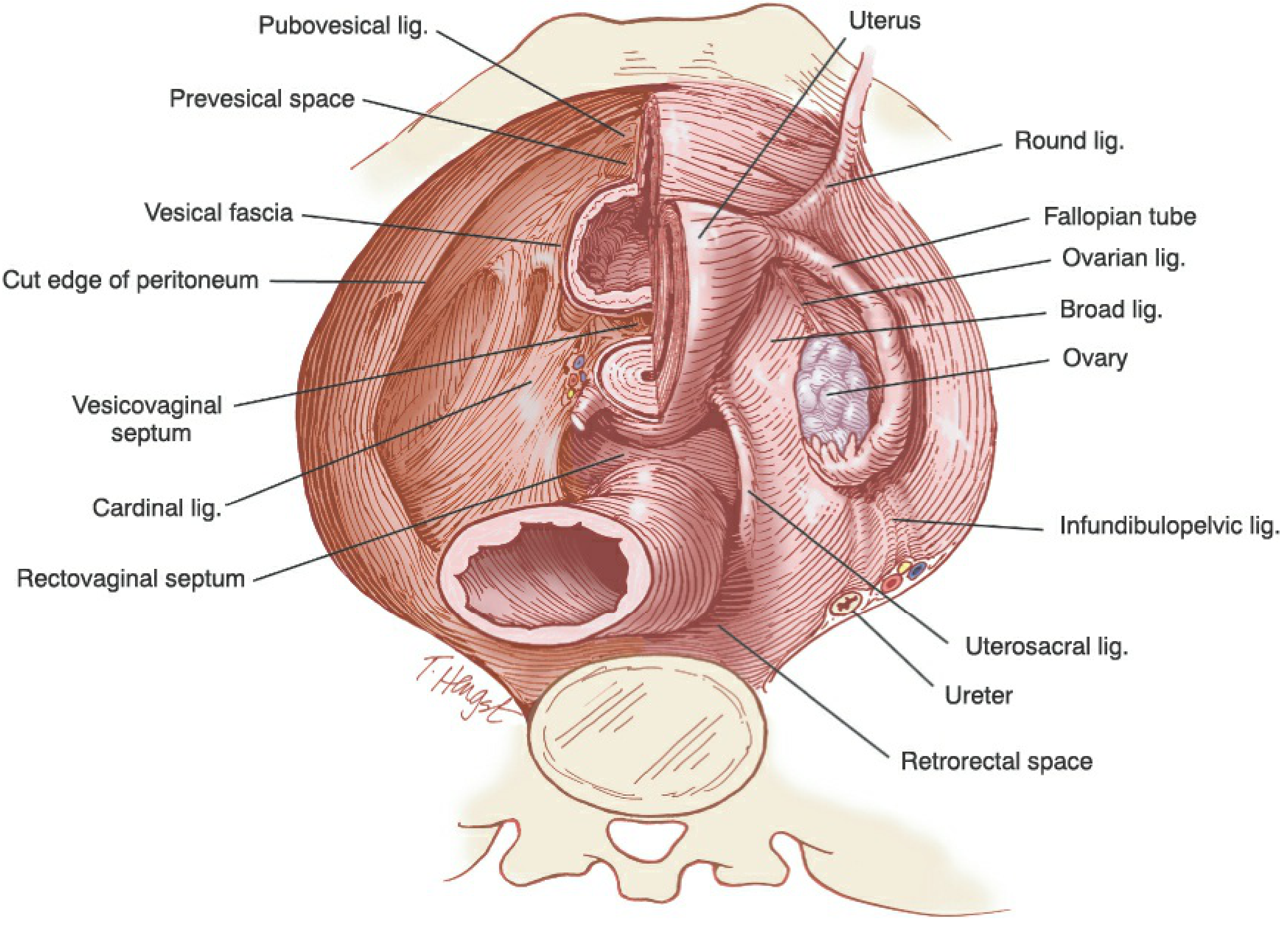
A. PRIMARY (MAIN) SUPPORTS - Ligaments at the Cervical Level
These are the most important supports and prevent uterine prolapse. They support the uterus at the level of the cervix and upper vagina.
1. Cardinal Ligaments (Mackenrodt's Ligaments / Transverse Cervical Ligaments)
- The most important supports of the uterus
- Condensations of endopelvic fascia running from the cervix and upper vagina laterally to the pelvic sidewall
- Prevent downward descent of the uterus
- The uterine artery runs within the cardinal ligament; the ureter passes beneath the uterine artery here ("water under the bridge" or "bridge over water")
- Ureter lies 2-3 cm lateral to the cervix at this point - a key surgical danger zone
2. Uterosacral Ligaments
- Run from the cervix and upper vagina posteriorly to the lateral sacrum
- They are the posterior components of the cardinal ligament complex
- Interdigitate with cardinal ligament fibers near the cervix
- Provide support to the cervix and upper vagina
- Contain parasympathetic nerve fibers (pelvic splanchnic nerves)
- Clinically used for vaginal vault suspension after hysterectomy
B. SECONDARY SUPPORTS - Ligaments That Maintain Position But Are Not the Main Supports
3. Round Ligaments
- Run from the uterine cornu, through the inguinal canal, to the labium majus
- Maintain the uterus in anteversion (not the main support against prolapse)
- Course inferolaterally toward the internal inguinal ring
- These do not prevent prolapse - they only help maintain anteversion
4. Broad Ligaments
- Double folds of peritoneum extending from the uterus laterally to the pelvic sidewall
- Carry the neurovascular pedicles (tubes, ovarian vessels, uterine vessels)
- Do not provide significant support against prolapse
- Superiorly extends into the infundibulopelvic ligament
5. Pubovesical (Pubocervical) Ligaments
- Run anteriorly from the cervix/upper vagina to the pubic bone
- Part of the endopelvic fascial condensation
- Help maintain anterior support
C. MUSCULAR SUPPORTS (Pelvic Floor / Pelvic Diaphragm)
These form the floor on which the uterus rests and are essential for preventing prolapse:
1. Levator Ani Muscle - most important muscular support
- Composed of: pubococcygeus, iliococcygeus, and puborectalis
- Forms a muscular sling around the vagina, urethra, and rectum
- The puborectalis maintains the anorectal angle and supports the vagina
2. Perineal Body
- Central tendinous point of the perineum
- Insertion point for multiple perineal muscles
- Loss of perineal body support leads to posterior vaginal wall prolapse
3. Endopelvic Fascia
- Fibroareolar tissue that follows blood supply to visceral organs
- Acts as a retroperitoneal mesentery
- Divided into:
- Parametrium - connects to the uterus (cardinal + uterosacral ligaments)
- Paracolpium - connects to the vagina
- The arcus tendineus fasciae pelvis (white line) runs from pubis to ischial spine and provides lateral paravaginal support
D. FUNCTIONAL SUPPORT - Vaginal Axis
- The normal posterior inclination of the vaginal axis directs intra-abdominal pressure onto the levator plate rather than through the pelvic outlet
- This is an important functional support mechanism
Clinical Significance - Defects in Support Lead To:
| Support Defect | Clinical Result |
|---|---|
| Cardinal/uterosacral ligament weakness | Uterine prolapse |
| Pubocervical fascia defect | Cystocele (anterior wall prolapse) |
| Rectovaginal fascia/septum defect | Rectocele (posterior wall prolapse) |
| Levator ani damage | Worsens all forms of prolapse |
| Perineal body deficiency | Perineal descent, rectocele |
Shaw's Classification of Uterine Supports (Traditional Framework)
In Shaw's Textbook of Gynaecology, the supports are classically described under three categories:
- Ligamentous supports (Cardinal, Uterosacral, Round, Broad ligaments)
- Muscular supports (Pelvic floor - levator ani, perineal muscles)
- Functional supports (Normal vaginal axis and intra-abdominal pressure dynamics)
The cardinal and uterosacral ligaments are emphasized as the primary supports preventing prolapse, while the round ligaments, though anatomically prominent, are functionally secondary (they maintain anteversion but do not prevent descent).
Source: Berek & Novak's Gynecology; standard Shaw's Gynaecology framework
This is a shared conversation. Sign in to Orris to start your own chat.