Acute Suppurative Otitis Media
Reading File
Finding Sources
Finding Sources
Searching PubMed
"acute otitis media" AND treatment
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
I now have comprehensive information to write a thorough, well-cited answer. Let me compile it:
Acute Suppurative Otitis Media (ASOM)
Definition
Acute suppurative (purulent) otitis media is a bacterial infection of the middle ear space arising de novo in a previously normal middle ear. It is characterized by vascular dilation and proliferation (manifested by tympanic membrane edema and erythema), mucosal edema, exudation, bacterial proliferation, white blood cell infiltration, and pus formation — Cummings Otolaryngology, p. 2703.
Epidemiology
- Among the most common bacterial infections of childhood; ~85% of all children experience at least one episode
- Incidence peaks at 6–24 months of age; by age 3, 50% of children have had ≥3 episodes
- Global incidence: ~10.8 new episodes per 100 people/year, with the highest burden in sub-Saharan Africa and lowest in central Europe
- Global AOM incidence is highest in children aged 1–4 years (61 episodes per 100 children/year)
— Cummings Otolaryngology, p. 3767; Harrison's 22e, p. 297
Pathogenesis
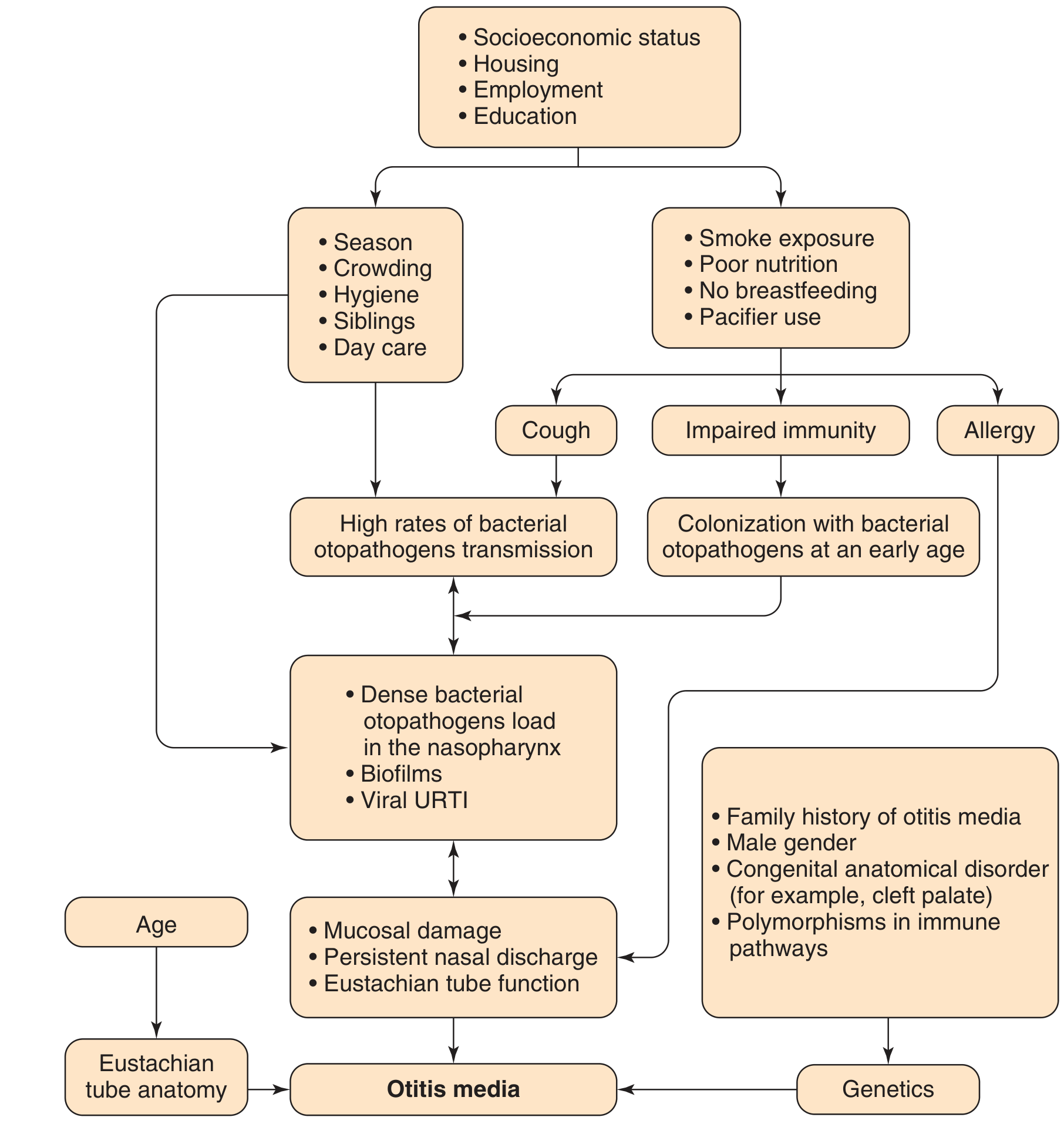
Sequence of events:
- A viral upper respiratory tract infection (URTI) causes edema and inflammation of the nasopharynx and eustachian tube
- Eustachian tube dysfunction → failure to drain secretions and equalize middle ear pressure → fluid collection
- Bacteria colonizing the nasopharynx ascend and infect the middle ear effusion
- Inflammatory cascade → suppuration
Why children are more susceptible: The infant's eustachian tube is shorter (13 mm vs. 35 mm in adults), wider, more floppy, and nearly horizontal (~10°), facilitating pathogen passage. As children grow, the tube elongates and the angle increases to ~45°, reducing susceptibility. — Cummings Otolaryngology, p. 3768
Biofilm formation: Bacteria such as nontypeable H. influenzae form sessile communities encased in exopolysaccharide matrices, protecting them from host immunity and antibiotics — a key mechanism for persistence and recurrence.
Microbiology
| Organism | Frequency |
|---|---|
| Streptococcus pneumoniae | ~30% |
| Haemophilus influenzae (nontypeable) | ~20% |
| Moraxella catarrhalis (Branhamella) | ~10% |
Impact of pneumococcal conjugate vaccines (PCVs): PCV7 (2000) and PCV13 (2010) significantly reduced S. pneumoniae-related AOM. As a result, the proportional burden from nontypeable H. influenzae and M. catarrhalis has increased. Non-vaccine pneumococcal serotypes have also emerged. — Cummings Otolaryngology, p. 3768; Red Book 2021, p. 1415
Viral co-pathogens include RSV, rhinoviruses, enteroviruses, coronaviruses, influenza virus, adenoviruses, and human metapneumovirus.
Risk Factors
Host factors: Age <2 years, male sex, craniofacial anomalies (cleft palate, Down syndrome), immunodeficiency, ciliary dyskinesia (e.g., cystic fibrosis), genetic predisposition, aboriginal ancestry, adenoid hypertrophy
Environmental factors: Daycare attendance, having older siblings, tobacco smoke exposure, low socioeconomic status, fall/winter season, pacifier use, bottle-feeding, crowded living conditions
Protective: Breastfeeding (exclusive ≥6 months)
Clinical Features
| Feature | Description |
|---|---|
| Otalgia | Primary complaint — may be severe; irritability in infants |
| Fever | Common, >102.2°F in severe cases |
| Otorrhea | If tympanic membrane has perforated |
| Hearing loss | Conductive type |
| Anorexia/irritability | Especially in young children |
Otoscopic findings:
- Bulging, inflamed, opacified tympanic membrane with obscured landmarks
- Immobility of tympanic membrane on pneumatic otoscopy / Valsalva
- New-onset otorrhea (not from external otitis)
Diagnostic criteria (AAP): AOM should be diagnosed with moderate-to-severe bulging of the TM or new-onset otorrhea; with mild bulging only if symptoms <48 h or intense erythema is present. AOM should not be diagnosed without middle-ear effusion. — Harrison's 22e, p. 297–298
Management
Pain Control
NSAIDs or acetaminophen for mild-to-moderate otalgia. Topical agents (benzocaine, lidocaine) provide brief additional benefit.
Antibiotic Decision
In up to 80% of children, AOM resolves without antibiotics. Indications for antibiotics:
| Age Group | Indication for Antibiotics |
|---|---|
| <6 months | All cases |
| 6 months – 2 years | Bilateral ear findings |
| ≥6 months | Otorrhea present |
| >2 years | Symptoms worsening/not improving within 48–72 h |
| All ages | Severe otalgia, otalgia ≥2 days, or fever >102.2°F |
— Harrison's 22e Table 37-1, p. 298
Antibiotic Regimens
| Situation | Drug of Choice | Alternatives |
|---|---|---|
| First-line | High-dose amoxicillin 90 mg/kg/day (max 3 g) | Cefdinir, cefuroxime, cefpodoxime, IM ceftriaxone |
| Amoxicillin in prior 30 days | Amoxicillin-clavulanate 90/6.4 mg/kg/day in 2 divided doses | — |
| Failure after 48–72 h | Amoxicillin-clavulanate, 2nd/3rd-gen cephalosporin, or IM ceftriaxone ×3 days | Refer to specialist if still failing |
| Adults | Amoxicillin + decongestants + analgesics | — |
Duration:
- <2 years or severe symptoms: 10 days
- 2–5 years, mild-moderate: 5–7 days
- ≥6 years, mild-moderate: 5 days
— Harrison's 22e, p. 298; Red Book 2021
Tympanostomy Tubes
Indicated for recurrent AOM (≥3 episodes in 6 months or ≥4 in 1 year). Associated with a modest reduction of ~1.5 AOM episodes/child in the first 6 months. Antibiotic prophylaxis is no longer recommended for recurrent AOM prevention. — Red Book 2021, p. 1415
Myringotomy
Can be performed to obtain culture material and reduce bacterial load in complicated or severe/refractory AOM.
Complications
Extracranial
- Acute mastoiditis — most common complication; suggested by post-auricular tenderness, mass, or displaced ear lobe. Rare (NNT ~5,000 antibiotic patients to prevent 1 case)
- Facial nerve paralysis
- Labyrinthitis / serous labyrinthitis
- Subperiosteal abscess (Bezold's abscess: tracks along sternomastoid; temporal root abscess)
- Petrous apicitis (Gradenigo's syndrome: VI nerve palsy + retro-orbital pain + otorrhea)
Intracranial
- Meningitis
- Brain abscess (intraparenchymal, epidural, subdural)
- Lateral (sigmoid) sinus thrombosis
- Otitic hydrocephalus
Spread may be by direct extension or hematogenous routes. Evaluation requires CT and/or MRI plus CSF analysis when indicated. Treatment includes appropriate IV antibiotics, myringotomy ± tube placement, and surgical drainage when necessary. — Cummings Otolaryngology, p. 2703
Prevention
- PCV13 vaccination — reduces pneumococcal AOM and mastoiditis
- Exclusive breastfeeding ≥6 months
- Avoidance of tobacco smoke exposure
- Reduction of pacifier use, daycare exposure when feasible
- Influenza vaccination — reduces viral URTIs that predispose to AOM
Recent Evidence
Recent systematic reviews (2024–2025) are relevant:
- Antibiotic prophylaxis for recurrent AOM — Davies et al. 2025, PMID 39394875: a systematic review/meta-analysis confirms modest efficacy of antimicrobial chemoprophylaxis but supports current guidelines discouraging routine prophylaxis
- Antibiotics to prevent AOM complications — Smolinski et al. 2024, PMID 38885271: meta-analysis found antibiotics modestly reduce infectious complications (e.g., mastoiditis)
Key sources: Cummings Otolaryngology Head and Neck Surgery (pp. 2703, 3767–3768); Harrison's Principles of Internal Medicine 22e (pp. 297–298); Red Book 2021 (p. 1415)
This is a shared conversation. Sign in to Orris to start your own chat.