Lipids & Fatty Acid Metabolism ● Classification & Functions: Define and classify lipids with suitable examples; Biological/Biomedical importance of lipids; Functions of lipids; Phospholipids of biological importance. ● Digestion & Storage: Digestion and absorption of lipids/fats; Biosynthesis & storage of fat; Role of liver in fat metabolism (fatty liver - causes and prevention). ● Oxidation & Ketones: Beta-oxidation of fatty acids (e.g., palmitic acid) and its energetics; Ketone body formation and their utilization; Causes of ketosis; Metabolic ketoacidosis. ● Lipoproteins & Cholesterol: Define, structure, classify lipoproteins and state their functions/significance; Cholesterol synthesis; Atherosclerosis.
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Lipids & Fatty Acid Metabolism - Comprehensive Notes
PART 1 - CLASSIFICATION & FUNCTIONS
Definition of Lipids
Lipids are a heterogeneous group of organic compounds of biological origin, composed primarily of carbon, hydrogen, and a smaller amount of oxygen. Some also contain nitrogen and phosphorus. They are sparingly soluble in water but preferentially soluble in organic solvents such as ether, chloroform, and benzene. A widely used indicator of lipid character is the octanol-water partition coefficient (typically 10^4-10^7 for most lipids).
The biological fate of lipids depends critically on their chemical structure and interactions with water. All lipids that interact with water are amphiphilic - they contain both polar (hydrophilic) and nonpolar (hydrophobic) regions.
- Medical Physiology (Boron & Boulpaep), p. 1375
Classification of Lipids
| Class | Examples | Key Feature |
|---|---|---|
| Simple lipids (esters of fatty acids with alcohols) | Fats (triacylglycerols), waxes | >90% of dietary fat |
| Compound/Complex lipids (contain additional groups) | Phospholipids, glycolipids, lipoproteins | Amphiphilic |
| Derived lipids (from hydrolysis of above) | Fatty acids, sterols, cholesterol, ketone bodies | Variable |
| Miscellaneous | Terpenes, carotenoids, fat-soluble vitamins (A, D, E, K) | Nonpolar |
Fatty acid subtypes:
- Saturated (no double bonds): Palmitic acid (C16:0), Stearic acid (C18:0)
- Monounsaturated (one double bond): Oleic acid (C18:1, omega-9)
- Polyunsaturated (PUFAs): Linoleic acid (C18:2, omega-6), Linolenic acid (C18:3, omega-3), Arachidonic acid (C20:4)
- Essential fatty acids: Linoleic and alpha-linolenic acid (must be obtained from diet)
Biological/Biomedical Importance & Functions of Lipids
- Energy storage - Triacylglycerols (TAGs) are the most concentrated energy store (~9 kcal/g vs 4 kcal/g for carbohydrates). Stored in adipose tissue, they fuel the body during fasting.
- Structural components - Phospholipids and cholesterol are essential components of all cell membranes (lipid bilayer), providing fluidity and selective permeability.
- Thermal insulation - Subcutaneous fat prevents heat loss.
- Mechanical protection - Perirenal fat cushions organs.
- Precursors of hormones - Cholesterol is the precursor to steroid hormones (cortisol, aldosterone, sex hormones) and vitamin D.
- Precursors of eicosanoids - Arachidonic acid is the precursor to prostaglandins, thromboxanes, and leukotrienes (important in inflammation).
- Absorption of fat-soluble vitamins (A, D, E, K) - dietary fat is required for their intestinal absorption.
- Signaling - Diacylglycerol (DAG) and inositol trisphosphate (IP3) are second messengers; ceramide is involved in apoptosis.
- Bile acid synthesis - Cholesterol is converted to bile acids required for fat digestion.
- Nervous system - Myelin sheath is rich in sphingomyelin and cerebrosides; essential for nerve conduction.
Phospholipids of Biological Importance
Phospholipids are the most abundant complex lipids. They have a glycerol (or sphingosine) backbone, two fatty acid chains, a phosphate group, and a polar head group. They are amphiphilic - ideal for membrane formation.
| Phospholipid | Head Group | Location/Function |
|---|---|---|
| Phosphatidylcholine (Lecithin) | Choline | Most abundant; outer leaflet of plasma membrane; lung surfactant (DPPC) |
| Phosphatidylethanolamine (Cephalin) | Ethanolamine | Inner leaflet; blood clotting |
| Phosphatidylserine | Serine | Inner leaflet; flips to outer surface during apoptosis (phagocytosis signal) |
| Phosphatidylinositol | Inositol | Second messenger generation (IP3/DAG pathway); anchors GPI-linked proteins |
| Phosphatidylglycerol | Glycerol | Mitochondrial membrane; precursor to cardiolipin |
| Cardiolipin | 2 phosphatidylglycerols | Inner mitochondrial membrane; required for oxidative phosphorylation |
| Sphingomyelin | Choline (via sphingosine) | Myelin sheath; outer plasma membrane leaflet |
| Platelet Activating Factor (PAF) | Choline | Potent inflammatory mediator |
Clinical pearl: Dipalmitoylphosphatidylcholine (DPPC/Lecithin) is the major surfactant component of lung alveoli. Its deficiency causes Respiratory Distress Syndrome (RDS) in premature infants.
PART 2 - DIGESTION & STORAGE
Digestion and Absorption of Lipids/Fats
Dietary fat is composed of >90% TAGs. Digestion occurs in a stepwise sequence:
Step 1 - Emulsification
- Mechanical churning of the stomach creates a coarse emulsion of fat droplets
- Bile salts (secreted from liver via gallbladder) emulsify fat, dramatically increasing surface area for enzyme action
Step 2 - Enzymatic hydrolysis
- Lingual lipase (minor; acid-stable) begins hydrolysis in the stomach
- Gastric lipase - acts at pH 2-6
- Pancreatic lipase - primary digestive enzyme; cleaves TAGs at sn-1 and sn-3 positions, producing 2-monoacylglycerol (2-MAG) + 2 free fatty acids. Requires colipase (pancreatic co-protein) to anchor to lipid droplet surface at pH 5.5-6.5 in duodenum
- Cholesterol esterase - hydrolyzes cholesteryl esters
- Phospholipase A2 (PLA2) - cleaves the sn-2 fatty acid from phospholipids, producing lysophospholipids
Step 3 - Micellar solubilization
As surface TAGs are hydrolyzed, lipolytic products (MAGs, free fatty acids, lyso-phosphatidylcholine, cholesterol) form multilamellar liquid crystal vesicles. Bile-salt micelles transform these into mixed micelles - the primary vehicle for delivering lipids to the absorptive surface of the jejunum.
Step 4 - Absorption across jejunal brush border
Mixed micelles diffuse through the unstirred water layer to the enterocyte brush border membrane. Fatty acids and 2-MAG diffuse across (some via fatty acid transport proteins - FATP4). Inside the enterocyte:
- Long-chain fatty acids (>14C) are re-esterified to TAGs in the smooth ER
- TAGs are assembled into chylomicrons (with apolipoprotein B-48, cholesterol, phospholipids)
- Chylomicrons are secreted via exocytosis into intestinal lacteals (lymphatics) → thoracic duct → bloodstream
Short and medium-chain fatty acids (≤12C) are absorbed directly into the portal blood without re-esterification.
- Medical Physiology (Boron & Boulpaep), p. 1381
Biosynthesis & Storage of Fat (Triacylglycerols)
De novo lipogenesis occurs primarily in the liver and adipose tissue, mainly in the fed state (high insulin:glucagon ratio).
Key steps:
- Glucose → Acetyl-CoA (via pyruvate dehydrogenase) in mitochondria
- Acetyl-CoA exits mitochondria as citrate, then is cleaved by ATP-citrate lyase back to acetyl-CoA in cytosol
- Acetyl-CoA → Malonyl-CoA: catalyzed by Acetyl-CoA Carboxylase (ACC) - the rate-limiting step; requires biotin and HCO3-; activated by citrate; inhibited by palmitoyl-CoA
- Fatty acid synthase (FAS) complex sequentially adds 2-carbon units from malonyl-CoA to produce palmitate (C16:0)
- Palmitate can be elongated and desaturated to other fatty acids
- Three fatty acids esterify glycerol-3-phosphate → Triacylglycerol (TAG)
Storage: TAGs are stored in adipocytes as large lipid droplets (essentially anhydrous - hence very energy-dense). During fasting, hormone-sensitive lipase (HSL, activated by glucagon/adrenaline) and adipose triglyceride lipase (ATGL) mobilize stored TAG via lipolysis → free fatty acids + glycerol enter blood.
| Feature | Synthesis | Degradation (β-oxidation) |
|---|---|---|
| When maximal | After carbohydrate-rich meal | During starvation/fasting |
| Hormonal state | High insulin/glucagon | Low insulin/glucagon |
| Major organ | Liver | Muscle, liver |
| Subcellular location | Cytosol | Mitochondrial matrix |
| Shuttle | Citrate (mito → cytosol) | Carnitine (cytosol → mito) |
| Coenzymes | NADPH (reduction) | NAD+, FAD (oxidation) |
| Inhibitor | Palmitoyl-CoA (inhibits ACC) | Malonyl-CoA (inhibits CPT-I) |
- Biochemistry, 8th ed. Lippincott Illustrated Reviews, p. 544-548
Role of Liver in Fat Metabolism - Fatty Liver
The liver is the central organ of lipid metabolism. Its major roles include:
- Synthesis of fatty acids, TAGs, cholesterol, bile acids, and phospholipids
- Packaging and export of lipids as VLDL
- Beta-oxidation of fatty acids; generation of ketone bodies
- Lipoprotein synthesis and secretion
Fatty Liver (Hepatic Steatosis)
Defined as abnormal accumulation of TAG in hepatocytes (>5% of liver weight).
Causes - any imbalance between fat input and fat export:
| Cause | Mechanism |
|---|---|
| Alcoholism (most common in adults) | Alcohol → acetaldehyde/acetate; excess NADH shifts metabolism toward fat synthesis, inhibits fatty acid oxidation, disrupts VLDL export |
| Obesity/Type 2 Diabetes | Excess free fatty acid flux to liver from insulin-resistant adipose tissue |
| High-fat/high-carbohydrate diet | Excess substrate for de novo lipogenesis |
| Starvation/Protein deficiency (kwashiorkor) | Impaired apolipoprotein B-48/100 synthesis → VLDL cannot be assembled/exported |
| Carbon tetrachloride (CCl4) toxicity | Inhibits VLDL secretion by damaging ER |
| Drugs (e.g., tetracycline, methotrexate, valproate) | Impair mitochondrial β-oxidation or VLDL secretion |
| Lipotrope deficiency | Lack of choline, methionine, or inositol impairs phosphatidylcholine synthesis → impaired VLDL assembly |
Prevention:
- Lipotropic factors (choline, methionine, betaine, inositol) - promote phospholipid synthesis needed for VLDL packaging
- Avoid alcohol and hepatotoxic drugs
- Weight loss, exercise in NAFLD
- Treat underlying diabetes/dyslipidemia
- Adequate dietary protein
PART 3 - OXIDATION & KETONES
Beta-Oxidation of Fatty Acids
Beta-oxidation is the major catabolic pathway for fatty acids, occurring in the mitochondrial matrix. It sequentially removes 2-carbon (acetyl-CoA) units from the carboxyl end of the acyl chain.
Step 0 - Activation (cytosol)
Fatty acid + CoA + ATP → Fatty acyl-CoA + AMP + PPi
Enzyme: Acyl-CoA synthetase (Thiokinase)
Cost: equivalent to 2 ATP (ATP → AMP + PPi; PPi is hydrolyzed to 2 Pi)
Step 1 - Transport into mitochondria (Carnitine Shuttle)
Long-chain fatty acids (>12C) cannot cross the inner mitochondrial membrane as CoA derivatives. They use the carnitine shuttle:
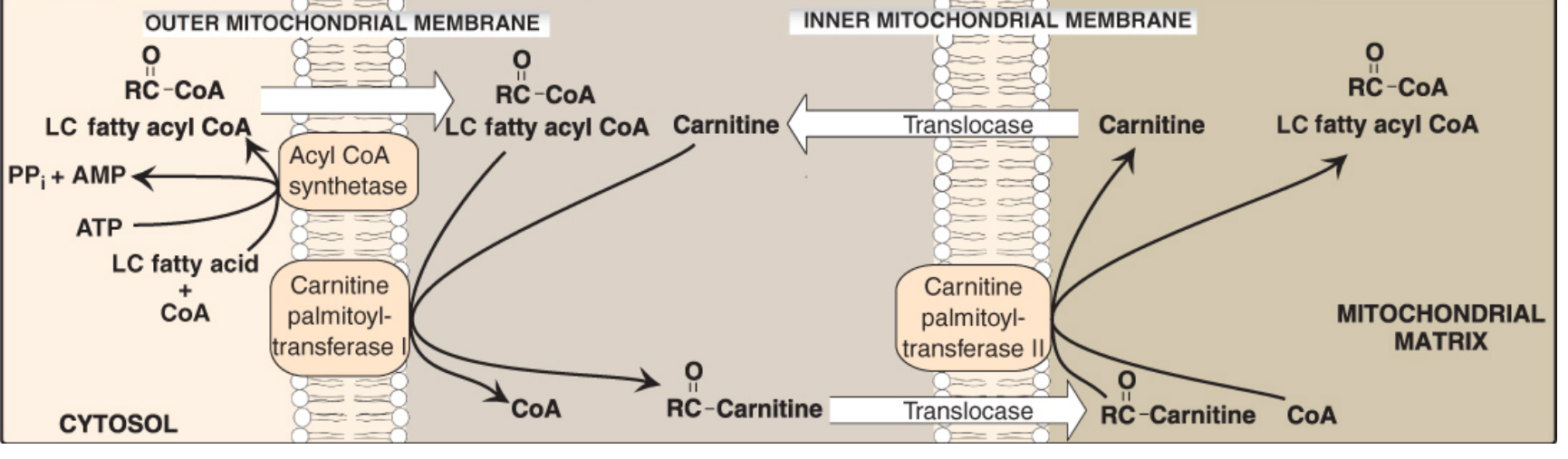
- CPT-I (outer membrane): Acyl-CoA + Carnitine → Acyl-carnitine + CoA
- Acyl-carnitine transported in; free carnitine out (by carnitine-acylcarnitine translocase)
- CPT-II (inner membrane): Acyl-carnitine + CoA → Acyl-CoA + Carnitine
- CPT-I is inhibited by malonyl-CoA (thus when synthesis is on, oxidation is off)
Fatty acids ≤12C cross freely without carnitine.
- Biochemistry, 8th ed. Lippincott Illustrated Reviews, p. 542-543
Step 2 - The Four Reactions of One β-Oxidation Cycle
| Reaction | Enzyme | Coenzyme | Product |
|---|---|---|---|
| 1. Oxidation | Acyl-CoA dehydrogenase | FAD → FADH2 | trans-Δ2-Enoyl-CoA |
| 2. Hydration | Enoyl-CoA hydratase | - | L-3-Hydroxyacyl-CoA |
| 3. Oxidation | L-3-Hydroxyacyl-CoA dehydrogenase | NAD+ → NADH | 3-Ketoacyl-CoA |
| 4. Thiolysis | Thiolase (β-ketothiolase) | CoA | Acetyl-CoA + shortened Acyl-CoA (2C shorter) |
Each cycle yields: 1 FADH2 + 1 NADH + 1 Acetyl-CoA
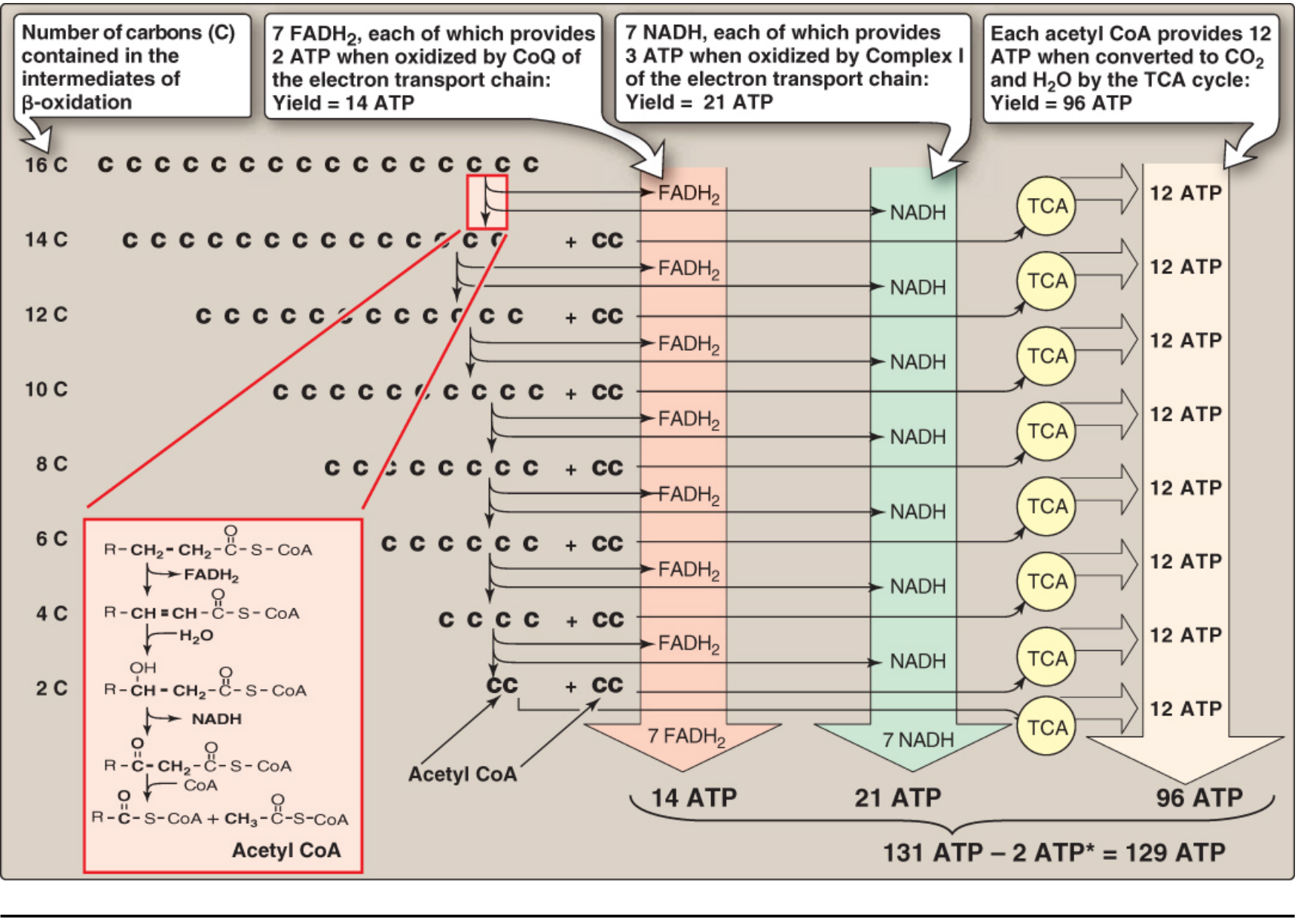
Energetics of Palmitate Oxidation (C16:0)
Palmitate (16 carbons) undergoes 7 cycles of beta-oxidation to yield 8 acetyl-CoA:
| Product | Yield per cycle x 7 cycles | ATP per molecule | Total ATP |
|---|---|---|---|
| FADH2 | 7 | × 2 ATP | = 14 ATP |
| NADH | 7 | × 3 ATP | = 21 ATP |
| Acetyl-CoA | 8 | × 12 ATP (via TCA) | = 96 ATP |
| Gross total | 131 ATP | ||
| Minus activation cost | -2 ATP | ||
| Net total | 129 ATP |
- Biochemistry, 8th ed. Lippincott Illustrated Reviews, p. 547-548
Note on newer P:O ratios: More recent values use FADH2 = 1.5 ATP and NADH = 2.5 ATP, yielding net ~106 ATP for palmitate. Exam questions may specify which to use.
Ketone Body Formation (Ketogenesis)
Ketone bodies are formed exclusively in the liver mitochondria from acetyl-CoA generated during beta-oxidation. This occurs mainly during fasting, starvation, prolonged exercise, and diabetes mellitus (insulin deficiency/resistance), when OAA is depleted and acetyl-CoA cannot enter the TCA cycle.
Three ketone bodies:
- Acetoacetate (the primary ketone body)
- β-Hydroxybutyrate (D-β-hydroxybutyrate - NOT a true ketone; most abundant in blood)
- Acetone (minor; volatile; excreted in breath; responsible for "fruity breath")
Pathway of synthesis:
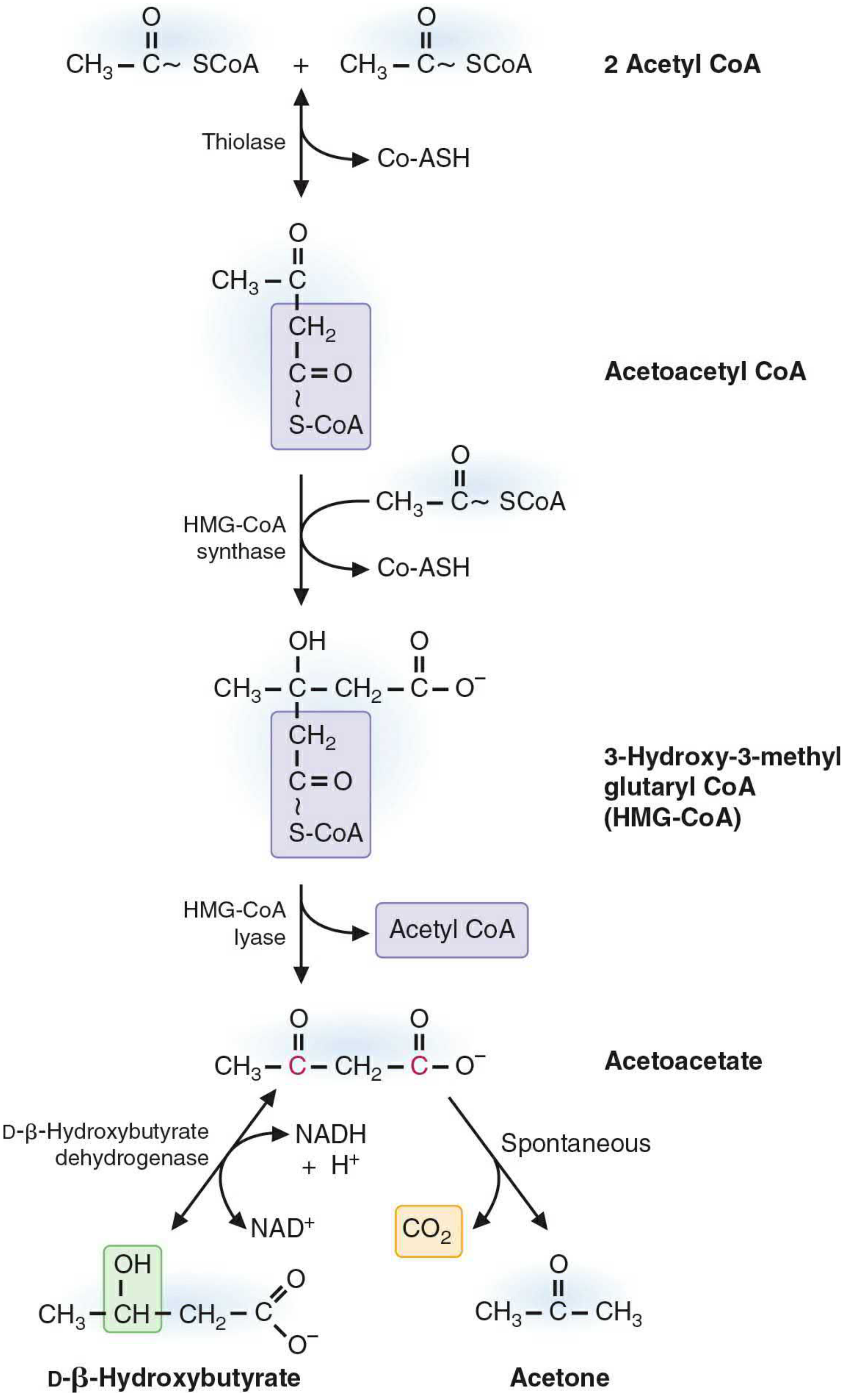
- 2 Acetyl-CoA → Acetoacetyl-CoA (Thiolase; reversible)
- Acetoacetyl-CoA + Acetyl-CoA → HMG-CoA (HMG-CoA synthase - mitochondrial isoform)
- HMG-CoA → Acetoacetate + Acetyl-CoA (HMG-CoA lyase)
- Acetoacetate + NADH → β-Hydroxybutyrate (β-hydroxybutyrate dehydrogenase)
- Acetoacetate → Acetone + CO2 (spontaneous decarboxylation)
The ratio β-hydroxybutyrate:acetoacetate is normally ~3:1, determined by the mitochondrial NADH/NAD+ ratio.
- Basic Medical Biochemistry, 6th ed. p. 1097-1098
Utilization of Ketone Bodies
The liver produces but cannot utilize ketone bodies (it lacks the transferase enzyme succinyl-CoA:3-ketoacid CoA transferase / thiophorase).
Utilization in extrahepatic tissues (brain, heart, skeletal muscle, kidney):
- β-Hydroxybutyrate → Acetoacetate (β-hydroxybutyrate dehydrogenase)
- Acetoacetate + Succinyl-CoA → Acetoacetyl-CoA + Succinate (thiophorase - the key enzyme absent in liver)
- Acetoacetyl-CoA → 2 Acetyl-CoA (thiolase)
- Acetyl-CoA enters TCA cycle → ATP
Ketone bodies are a vital alternative fuel, particularly for the brain during prolonged fasting (the brain cannot use free fatty acids directly but can use ketone bodies after adaptation).
Causes of Ketosis
Ketosis occurs when ketone body production exceeds peripheral utilization (blood ketones >1-2 mmol/L):
- Starvation/prolonged fasting - low carbohydrate, low insulin; OAA pulled into gluconeogenesis; acetyl-CoA diverted to ketogenesis
- Uncontrolled Type 1 Diabetes Mellitus - absolute insulin deficiency; uncontrolled lipolysis + impaired glucose uptake
- High-fat, low-carbohydrate diet (ketogenic diet)
- Alcoholism - excess NADH inhibits OAA availability; promotes ketogenesis
- Prolonged strenuous exercise - low insulin + high glucagon
- Vomiting/diarrhea leading to carbohydrate depletion
- Neonatal ketosis - high fat content of breast milk; limited hepatic glucose production
Metabolic Ketoacidosis
Diabetic Ketoacidosis (DKA) is the most important clinical form, occurring in Type 1 DM (and sometimes Type 2 DM):
Pathophysiology:
- Insulin deficiency → unrestrained glucagon action
- Lipolysis in adipose tissue massively accelerated → free fatty acids flood liver
- Hepatic beta-oxidation overwhelms TCA cycle capacity → ketone bodies accumulate
- Ketone bodies are organic acids → H+ accumulates → anion gap metabolic acidosis (pH < 7.35)
- Osmotic diuresis from hyperglycemia → dehydration, electrolyte loss
Biochemical features:
- Blood glucose >250 mg/dL
- Blood ketones elevated (acetoacetate + β-hydroxybutyrate)
- pH < 7.3, HCO3- < 15 mEq/L
- Increased anion gap = Na+ - (Cl- + HCO3-) > 12 mEq/L
- Ketonuria
- Fruity (acetone) breath
- Kussmaul breathing (deep, rapid - compensatory respiratory alkalosis)
Treatment: IV fluids, insulin, potassium replacement, monitor phosphate
PART 4 - LIPOPROTEINS & CHOLESTEROL
Definition & Structure of Lipoproteins
Lipoproteins are macromolecular complexes that transport hydrophobic lipids (TAGs, cholesterol esters) through the aqueous bloodstream. They consist of:
- Core: Hydrophobic lipids (TAGs, cholesteryl esters)
- Shell (surface): Amphipathic phospholipids (outer leaflet), free cholesterol, and apoproteins (apolipoproteins)
Apolipoproteins serve as:
- Structural stabilizers of the lipoprotein particle
- Ligands for cell surface receptors
- Activators or inhibitors of enzymes
Classification of Lipoproteins
Listed in order of increasing density (density = protein:lipid ratio):
| Lipoprotein | Density (g/mL) | Size | Major Lipid | Apolipoproteins | Origin | Function |
|---|---|---|---|---|---|---|
| Chylomicrons | <0.95 | Largest | TAGs (85-90%) | ApoB-48, ApoC-II, ApoE | Intestine | Transport dietary (exogenous) lipid to peripheral tissues |
| VLDL (Very Low Density) | 0.95-1.006 | Large | TAGs (55-65%) | ApoB-100, ApoC-II, ApoE | Liver | Transport endogenous (hepatic) TAGs to peripheral tissues |
| IDL (Intermediate Density) | 1.006-1.019 | Medium | TAGs + CE | ApoB-100, ApoE | From VLDL | Transient; taken up by liver or converted to LDL |
| LDL (Low Density) | 1.019-1.063 | Small | Cholesterol esters (45%) | ApoB-100 | From IDL | Deliver cholesterol to peripheral cells; "bad cholesterol" |
| HDL (High Density) | 1.063-1.210 | Smallest | Phospholipids, CE | ApoA-I, ApoA-II | Liver + Intestine | Reverse cholesterol transport; "good cholesterol" |
Key apolipoproteins and functions:
- ApoB-100: Ligand for LDL receptor (liver uptake of LDL/IDL)
- ApoB-48: Structural protein of chylomicrons (made in intestine)
- ApoC-II: Activates lipoprotein lipase (LPL) - essential for TAG clearance from chylomicrons and VLDL
- ApoE: Ligand for chylomicron remnant and IDL uptake by liver
- ApoA-I: Activates LCAT (lecithin-cholesterol acyltransferase) - esterifies cholesterol during reverse transport
Lipoprotein Metabolism
Exogenous pathway (dietary lipids):
Chylomicrons formed in intestine → lymphatics → blood → LPL on capillary endothelium (activated by ApoC-II) hydrolyzes TAG → fatty acids enter tissues → Chylomicron remnants taken up by liver (via ApoE/remnant receptor)
Endogenous pathway (hepatic lipids):
Liver secretes VLDL → LPL hydrolyzes VLDL-TAG → IDL → LDL (most IDL is converted to LDL in plasma)
LDL taken up by cells via LDL receptor (recognizes ApoB-100) → endocytosis → lysosomal hydrolysis → free cholesterol released for cell use
Reverse cholesterol transport:
HDL (nascent disc form) picks up cholesterol from cells → LCAT esterifies it (ApoA-I activates) → CE moves to core → mature spherical HDL → CE transferred to VLDL/LDL by CETP → eventually delivered to liver
Cholesterol Synthesis
All tissues synthesize cholesterol; liver, intestine, adrenal cortex, and reproductive organs are the major contributors. All carbons come from acetyl-CoA; NADPH provides reducing equivalents.
Overview of Pathway (starting from acetyl-CoA):
- Acetyl-CoA → Acetoacetyl-CoA (thiolase; cytosolic)
- Acetoacetyl-CoA → HMG-CoA (HMG-CoA synthase - cytosolic isoform)
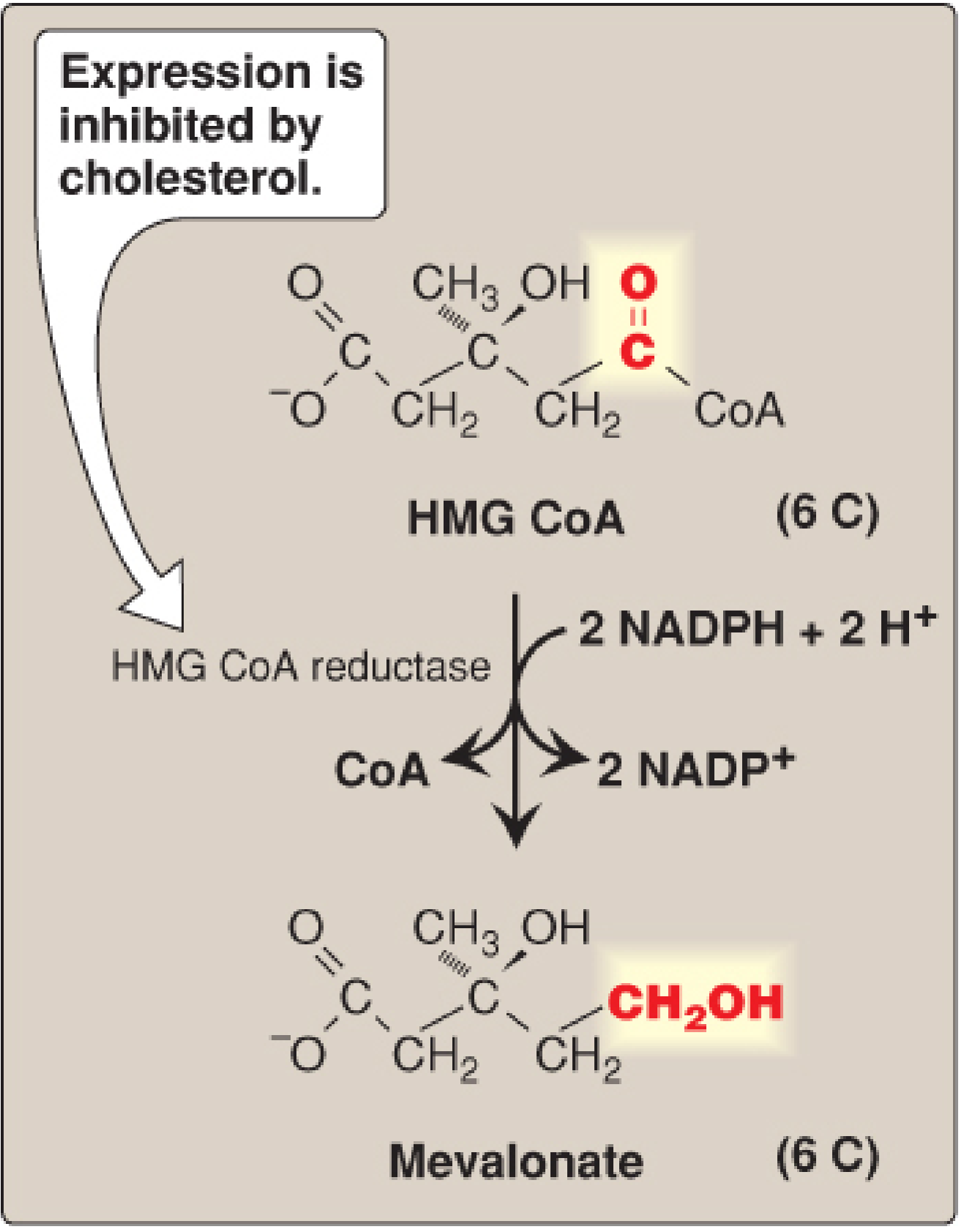
- HMG-CoA → Mevalonate (HMG-CoA reductase, requires 2 NADPH) - RATE-LIMITING STEP
- Mevalonate → Isopentenyl pyrophosphate (IPP) - active 5C isoprene unit (requires 3 ATP)
- 6 IPP → Squalene (30C; via farnesyl pyrophosphate, 15C)
- Squalene (30C) → Lanosterol (via squalene epoxidase + cyclase) → Cholesterol (27C; multi-step via SER)
- Biochemistry, 8th ed. Lippincott Illustrated Reviews, p. 618-626
Regulation of HMG-CoA Reductase:
- Sterol-dependent gene suppression: When cholesterol is high → SCAP-SREBP-2 complex retained in ER → reduced reductase gene transcription
- Accelerated enzyme degradation: High sterols → reductase binds INSIG → ubiquitination → proteasomal degradation
- Phosphorylation: AMPK (activated by AMP/low energy) phosphorylates and inactivates reductase; phosphatase activates it
- Hormonal: Insulin → dephosphorylation → activation; Glucagon/epinephrine → phosphorylation → inactivation
Pharmacological inhibition:
Statins (e.g., atorvastatin, simvastatin) are competitive inhibitors of HMG-CoA reductase → primary treatment for hypercholesterolemia. They also upregulate LDL receptors.
Atherosclerosis
Atherosclerosis is a chronic inflammatory disease of medium and large arteries characterized by subintimal deposition of lipids, smooth muscle proliferation, and plaque formation.
Pathogenesis (Response-to-Injury Hypothesis):
- Endothelial injury (from hypertension, smoking, hyperglycemia, LDL oxidation) → endothelial dysfunction
- LDL entry into intima → oxidized by reactive oxygen species → oxidized LDL (oxLDL) - highly atherogenic
- Monocyte recruitment: endothelium expresses adhesion molecules (VCAM-1, ICAM-1) → monocytes enter intima → differentiate to macrophages
- Foam cell formation: Macrophages take up oxLDL via scavenger receptors (unregulated uptake) → lipid-laden foam cells = "fatty streak" (earliest visible lesion)
- Smooth muscle cell migration from media to intima → proliferate and secrete extracellular matrix → fibrous plaque
- Plaque progression: necrotic core (dead foam cells), cholesterol crystals, calcification → complicated plaque/atheroma
- Plaque rupture → thrombosis → acute myocardial infarction or stroke
Role of Lipoproteins:
- LDL: High plasma LDL (especially oxidized LDL) is the primary atherogenic lipoprotein
- HDL: Performs reverse cholesterol transport; also anti-inflammatory and anti-oxidant. Epidemiologically, high HDL is protective; low HDL is a risk factor
- VLDL/IDL/Lp(a): Also atherogenic
Risk factors for atherosclerosis:
- Non-modifiable: Age, male sex, family history, genetic dyslipidemia
- Modifiable: Hypertension, hypercholesterolemia (esp. high LDL), diabetes mellitus, smoking, obesity, physical inactivity
- Familial hypercholesterolemia: Defective LDL receptors → LDL cannot be cleared → severe hypercholesterolemia (LDL 600-1000 mg/dL) → premature atherosclerosis before age 50
PCSK9 inhibitors (evolocumab, alirocumab) block PCSK9 enzyme which normally degrades LDL receptors; by inhibiting PCSK9, LDL receptor expression is preserved and LDL clearance is enhanced.
- Guyton and Hall Textbook of Medical Physiology, p. 2391-2403
Quick Summary Reference
| Topic | Key Enzyme | Rate-Limiting Step | Regulation |
|---|---|---|---|
| Fatty acid synthesis | ACC; FAS | ACC (malonyl-CoA synthesis) | Activated by insulin/citrate; inhibited by glucagon/palmitoyl-CoA |
| Beta-oxidation | CPT-I; acyl-CoA dehydrogenase | Carnitine shuttle (CPT-I) | Inhibited by malonyl-CoA (fed state) |
| Ketogenesis | HMG-CoA synthase (mito) | HMG-CoA synthase | Increased in starvation, DM, high fat diet |
| Cholesterol synthesis | HMG-CoA reductase | HMG-CoA reductase | Inhibited by sterols (SCAP/SREBP); by phosphorylation (AMPK); by statins |
Sources: Biochemistry, 8th ed. Lippincott Illustrated Reviews (primary); Medical Physiology (Boron & Boulpaep); Basic Medical Biochemistry, 6th ed.; Guyton and Hall Textbook of Medical Physiology
This is a shared conversation. Sign in to Orris to start your own chat.